Securing definitive control of a threatened airway is a fundamental skill in the care of critically ill patients and remains an ever-popular topic of discussion in Emergency Medicine. As Emergency Medicine providers, we find few procedures as satisfying or potentially difficult as airway management; we continually seek to hone our skills to provide the best care possible for our patients. In this post, we will outline practice-changing, evidence-based anatomic predictors of difficult intubation and highlight recent literature that will improve your airway outcomes.
Assessing: The Anatomically Difficult Airway
Definition: “The Difficult Airway”
Traditionally, we have been taught that difficult airways correlate with the Cormack-Lehane classification system (grade I to grade IV), with grade III’s and IV’s being “difficult” and I’s and II’s presumably being “easy.” Interestingly, the division between easy and difficult intubation seems to actually lie within grade II views, which range from 1-99% of visualized glottic opening (termed “grade IIa” views) to only arytenoids visible (termed “grade IIb” views). Recent evidence suggests that only 4% of patients with grade IIa views are difficult to intubate, compared to 66% of grade IIb views.1
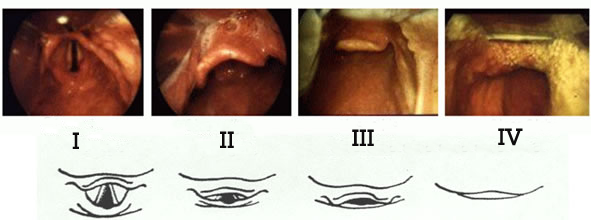
https://seattleclouds.com/myapplications/dukeg/ican/IntubatPosn.html
However, the CL classification is more so a surrogate for difficult intubation, since it functions primarily as a direct measure of difficult laryngoscopy, which does not necessarily correlate with how easy it will be to pass the tube. Increasingly, airway research is employing the Intubation Difficulty Scale (IDS), which includes the CL classification, the number of intubation attempts, clinicians involved, advanced airway adjuncts used, need for increased lifting force, the requirement for external laryngeal pressure, and whether the vocal cords are open or closed during laryngoscopy.
When we consider anatomically difficult airways, typically we can think about them in 3 main groups:
- Patients with clearly distorted anatomy (e.g., facial smash, severe angioedema, laryngeal cancers).
- Patients with apparently normal airways who have any number of difficult airway predictors (e.g., limitation in neck extension).
- Patients with completely normal, reassuring anatomy on airway assessment.
For patients who are not considered a “crash airway” (i.e., you have some time) without clearly distorted anatomy, we should be taking time to thoroughly assess for predictors of a difficult airway. Based on your assessment, you should ask yourself a few focused questions:
- Do you think intubation will be successful with RSI?
- If intubation is not successful, do you think you will still be able to oxygenate and ventilate this patient?
If you answer “no” to either of the questions above, you should consider changing your approach: use an airway adjunct, call for help, consider an awake intubation, avoid paralytics, RSI with a “double setup”, or proceed with a surgical airway. You can always refer to your local difficult airway algorithm for more information.
Predictors of Difficult Laryngoscopy/Intubation
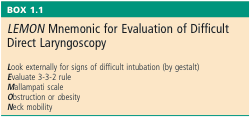
Classically, we have been taught that the primary predictors of a difficult intubation are “LEMON” (see below).
Rosen’s Emergency Medicine, 9th Ed.
Some of the best evidence we have to date shows that this test functions reasonably well as a screening test for all-comers of ED intubations. Hagiwara et al.2 published a multicenter, prospective, observational study examining the predictive characteristics of the LEMON score (without Mallampati) in 4034 patients undergoing ED intubation with either direct or video laryngoscopy (DL or VL). The prevalence of difficult intubation was 5.4% (95% CI, 4.7%-6.2%) in the DL group and 7.4% (95% CI, 5.6%-9.7%) in the VL group. They found that the overall positive LR was 1.6 and the negative LR was 0.13-0.3 for the LEMON score without the Mallampati component. However, this study had significant limitations, since it included all-comers (including the overtly difficult airways) and was self-reported data.
Recently, JAMA and Cochrane review articles have been published examining evidence-based predictors of difficult DL intubation in adult patients presenting with an apparently normal airway.3,4 The JAMA review included 62 high quality, operating room studies (n = 33559) and had an overall incidence of difficult DL intubation of 10% (8.2-12%). The conclusions of both the JAMA and Cochrane reviews are similar:
- No test or composite score is sensitive enough to rule out a difficult airway.
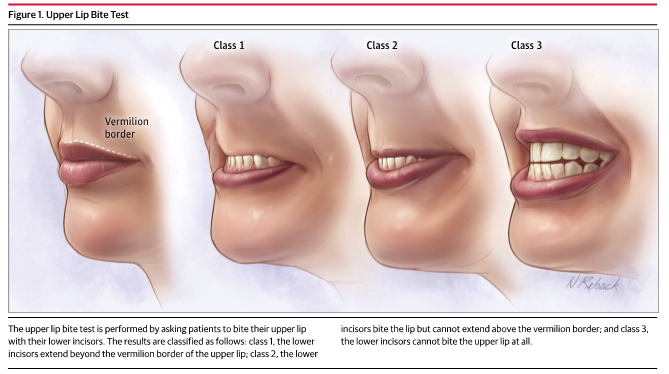
- The most specific test for predicting difficult DL was the upper lip bite test (shown below).
Scales, D. C. et al. Will This Patient Be Difficult to Intubate? Jama 321, 493 (2019).
An upper lip bite test class 2 or 3 was strongly associated with difficult DL: positive LR 12 (95% CI, 6.9-20), negative LR 0.42 (95% CI, 0.30-0.59). This positive LR changes patients with a 10% baseline pre-test probability of difficult intubation to approximately 60%.
For both reviews, grade 3 and 4 modified Mallampati scores were not strongly associated with difficult DL: positive LR 4.1 (95%CI, 3.0-5.6), negative LR 0.52 (95% CI, 0.45-0.60). A recent review article expands on the poor test characteristics of the modified Mallampati score for predicting difficulty with various airway adjuncts and in various populations.5 Overall, this is a poor test which is difficult to perform and has poor inter-rater reliability. We should probably not be employing or relying on Mallampati scores in the ED.
Finessing: Improving Your RSI Outcomes
First Pass Success
First pass success (FPS) during intubation has traditionally been considered a surrogate outcome: Does the patient really care if you don’t get the tube on the first try? Isn’t it fine to just come out, bag them, and then try again? A recent review article highlights that FPS as an outcome is likely much more patient-centered than we once thought.6 One study in particular identified that ≥3 intubation attempts were associated with a multitude of complications for in-hospital patients undergoing intubation:7
- More hypoxia (70% vs. 10.5%)
- More severe hypoxia (28% vs. 1.9%)
- More esophageal intubations (51.4% vs. 4.8%)
- More regurgitation (22% vs. 1.9%)
- More aspiration (13% vs. 0.8%)
- More bradycardia (18.5% vs. 1.6%)
- More cardiac arrests (11% vs. 0.7%)
Considering that the majority of ED providers only intubate with a FPS rate of 82%, what evidence is there to help ED physicians improve their FPS?
Driver et al. published a retrospective, single-center, observational trial which compared Bougie use to ETT/stylet in improving FPS for a cohort of 757 patients presenting to the ED undergoing intubation with MacIntosh laryngoscopy.8 Results showed that FPS was 95% (93-97%) for the Bougie group and 86% (79-93%) for the ETT/stylet group, with no other significant difference in patient-oriented outcomes. Although this was a single-center study and it is unclear what the distribution of difficult laryngoscopy/intubation was, this should be considered conclusive evidence that all ED physicians should be comfortable in using a Bougie and should consider making it routine.
For an in-depth analysis of the Driver et al. article, please see our journal club summary post here.
Preoxygenation and Apneic Oxygenation
For a full review and detailed approach to preoxygenation and apneic oxygenation, please see this reference below.9 The overall goals of proper preoxygenation should focus on recruitment and denitrogenation of the lungs, ideally bringing a patient’s spO2 as close to 100% as possible. If you have any concern of the patient suffering from shunt physiology (e.g., atelectasis, pulmonary edema, pneumonia), you should employ PEEP in one of these forms:
- BVM with a PEEP valve (typically set to 5-10cmH2O)
- NIPPV (BiPAP, CPAP)
- High Flow Nasal Cannula (HFNC) – Especially for patients who are not able to tolerate traditional forms of PEEP. Recent evidence suggests that HFNC is likely just as efficacious as NIPPV for preoxygenation.10
Classically, while performing RSI, ED providers have avoided ventilation following induction and before laryngoscopy of critically ill patients. The idea is that we sacrifice some degree of gas exchange for a theoretically decreased risk of gastric insufflation and aspiration. However, many have suggested that we should be focusing our efforts on treating the far more prevalent risk of hypoxia. The recent “PreVent” trial challenges the dogma of ventilation avoidance.11 This was an RCT including 401 adult ICU patients undergoing intubation, with the intervention group receiving BVM between induction and laryngoscopy and the control group receiving no BVM ventilation. Overall, they showed a significant difference in median lowest spO2 in the peri-intubation period, 96% (IQR, 87-99%) vs. 93% (IQR, 81-99%), and perhaps more importantly, a significant reduction in the incidence of severe hypoxemia (spO2 <80%), 10.9% vs. 22.8%, both favoring the BVM ventilation group. There was no significant difference in the incidence of aspiration between groups. However, the study was not powered to detect a difference in aspiration.
There are some important points to mention before we interpret the results. Importantly, they excluded all patients in whom “ventilation between induction and laryngoscopy was either required or contraindicated.” In addition, preoxygenation in this cohort of patients was suboptimal and heterogeneous, likely inflating the treatment effect (for more information, have a look at Table 2 in the study). This means we have to be cautious in interpreting this evidence.
Should we be bagging all patients during RSI? Probably not. But if they’re not at severely elevated risk of aspiration, and if there is any chance your patient will become hypoxemic during your intubation attempt, you should definitely consider ventilation after induction.
Lastly, while bagging, go with two thumbs down! A recent randomized crossover trial by Fei et al. looked at 103 obese, apneic patients undergoing general anesthetic, and looked at whether two-handed, thumbs down grip was better than the ‘EC clamp’ grip while using a ‘vent as bag’ technique (see below).12 Overall, they found the failure rate of ventilation to be 44% in the EC clamp compared to 0% in the thumb down grip (P<0.001). They also found that average tidal volumes were significantly lower for the EC clamp compared to two thumbs down: 371mL (SD 345) vs. 720mL (244) mL, (P<0.001).
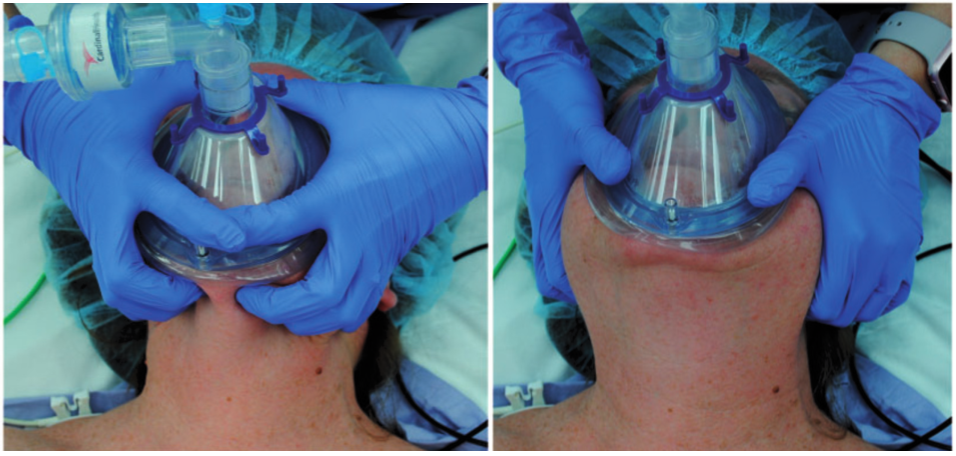
Fei, M. et al. Comparison of effectiveness of two commonly used two-handed mask ventilation techniques on unconscious apnoeic obese adults. Br. J. Anaesth. 118, 618–624 (2017).
Summary/Take Home Points
- LEMON (or “LEON” if you remove the Mallampati) is likely a good screening test for predicting difficult intubations for all-comers in the ED.
- Stop checking Mallampati! Please continue looking in the patient’s mouth for swelling, trauma, etc. But do not base your airway decisions on where the level of the tongue is in relation to the tonsillar pillars.
- Ask your patients to bite their upper lip. If they can’t bite past the vermillion border, you should be concerned that performing DL will be challenging.
- Never be reassured when patients do not have predictors of a difficult airway. There is no test with high enough sensitivity to rule out a difficult intubation effectively.
- Optimize your first attempt at intubation, because, after the first attempt, there’s good evidence to show that things get worse.
- Make using a Bougie routine. It’s cheap, it’s available, and it’s one of our airway adjuncts for a high-grade CL or a soiled airway. The more you use it, the better you become.
- Preoxygenate your patients well and have a very low threshold to employ PEEP, especially if you’re concerned about shunt physiology.
- If your patient is not at severe risk of aspiration, and if there’s any chance they may become even mildly hypoxemic during intubation, you should probably be bagging them after induction.
- BVM—two-person technique with two thumbs down every time!
References
- Brown, C. A. 3rd, Sakles, J. C. & Wick, N. The Walls Manual of Emergency Airway Management. (Wolters Kluwer, 2018).
- Hagiwara, Y., Watase, H., Okamoto, H., Goto, T. & Hasegawa, K. Prospective validation of the modified LEMON criteria to predict difficult intubation in the ED. Am. J. Emerg. Med. 33, 1492–1496 (2015).
- Scales, D. C. et al. Will This Patient Be Difficult to Intubate? Jama 321, 493 (2019).
- Roth, D. et al. Airway physical examination tests for detection of difficult airway management in apparently normal adult patients ( Review ) SUMMARY OF FINDINGS FOR THE MAIN COMPARISON. Cochrane Database Syst. Rev. (2018). doi:10.1002/14651858.CD008874.pub2.www.cochranelibrary.com
- Green, S. M. & Roback, M. G. Is the Mallampati Score Useful for Emergency Department Airway Management or Procedural Sedation? Ann. Emerg. Med. 1–9 (2019). doi:10.1016/j.annemergmed.2018.12.021
- Bernhard, M., Becker, T., Gries, A., Knapp, J. & Wenzel, V. First-SHot-is-the-Best-Shot. Anesth. Analg. (2015).
- Mort, T. C. Emergency tracheal intubation: Complications associated with repeated laryngoscopic attempts. Anesth. Analg. 99, 607–613 (2004).
- Reardon, R. F. et al. The Bougie and First-Pass Success in the Emergency Department. Ann. Emerg. Med. 70, 473-478.e1 (2017).
- Weingart, S. D. & Levitan, R. M. Preoxygenation and prevention of desaturation during emergency airway management. Ann. Emerg. Med. 59, 165-175.e1 (2012).
- Frat, J.-P. et al. Non-invasive ventilation versus high-flow nasal cannula oxygen therapy with apnoeic oxygenation for preoxygenation before intubation of patients with acute hypoxaemic respiratory failure: a randomised, multicentre, open-label trial. Lancet. Respir. Med. 7, 303–312 (2019).
- Casey, J. D. et al. Bag-Mask Ventilation during Tracheal Intubation of Critically Ill Adults. N. Engl. J. Med. NEJMoa1812405 (2019). doi:10.1056/NEJMoa1812405
- Fei, M. et al. Comparison of effectiveness of two commonly used two-handed mask ventilation techniques on unconscious apnoeic obese adults. Br. J. Anaesth. 118, 618–624 (2017).