This article discusses the patient perspective of early pregnancy loss in the ED. We will define the quality gap as it pertains to ED care for patients with early pregnancy loss. We will then look at patient-centered communication strategies for counseling and discharge of patients with early pregnancy loss in the ED.
Background
Early Pregnancy Loss (EPL) Definition
- A nonviable, intrauterine pregnancy with either an empty gestational sac or a gestational sac containing an embryo or fetus without fetal heart activity within the first 12 weeks and 6 days of gestation.1
- Interchangeable terms (1st trimester): miscarriage, spontaneous abortion, early pregnancy loss—no consensus on terminology, but ACOG favors the term EPL2
Incidence of EPL
- Nearly 1 in 5 pregnancies end in miscarriage, and usually in the first trimester of pregnancy up to 13 weeks gestation.3
- Approximately 80% of all cases of pregnancy loss occur within the first trimester.2
- First trimester bleeding occurs in approximately 1/3 of pregnancies (See Figure 1)—approximately 1/2 of these continue without further problems (See Figure 2).4

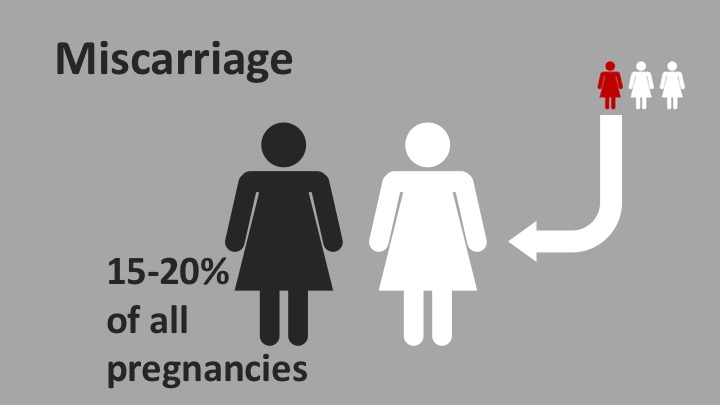
Figures 1 & 2. Infographics depicting the incidence of first trimester bleeding and early pregnancy loss. Figure 1 indicates that approximately 1 in 3 pregnancies will experience first trimester bleeding (FTB). Figure 2 depicts that approximately half of patients with FTB will have an uneventful pregnancy, but half (or 15-20% of all pregnancies) will experience early pregnancy loss (EPL).
Etiology and Risk Factors for EPL
- Approximately 50% of EPLs are due to fetal chromosomal abnormalities.5,6
- The most common risk factors among women experiencing EPL are advanced maternal age and a prior EPL.7
Understanding the patient perspective
- This should be important to us as Emergency Physicians because we see these patients every day.
- Larger centers may see 5-10 women per day with EPL, as is the case in our center.
- Understanding the patient perspective allows us to understand better what care patients expect and need in the ED, which can allow us to target interventions to improve their care.
Why do patients come to the ED when experiencing EPL
- A qualitative study of 67 women experiencing EPL determined their most common presenting symptoms and reasons they went to the ED:8
- Presenting symptoms:
- 85% vaginal bleeding—55.2% light spotting
- 3% cramping
- Reasons they went to the ED:
- 3% thought it was an emergency
- 4% didn’t know what else to do
- 5% didn’t have a doctor
- Presenting symptoms:
What do patients expect in the ED when experiencing EPL
- A survey of 141 women with first-trimester bleeding in the ED evaluated the maternal driving factors for seeking emergency care.9
- 8% (95% CI, 34-50.1%) stated the most common reason for the visit was to have an ultrasound and blood work performed to evaluate the well-being of their fetus.
- 34% (95% CI, 26.7-42.2%) simply wanted to know if they were having a miscarriage, with no specific method of evaluation mentioned.
- A minority ranked potentially emergent conditions: ectopic (3.5%), life-threatening hemorrhage (4.3%), or otherwise abnormal pregnancy (2.1%) as their chief concern.
- There was no indication as to whether POCUS performed by the ED physician or a radiology-performed ultrasound was preferred by patients.
Defining the quality gap with regards to EPL care in the ED
- Understanding the patient perspective and expectations of what they consider necessary care is key to defining the highest quality of care.
- Understanding the patient experience allows us to explore their care needs, and it is integral to the definition of Quality.
Quality Gap
- In 2001, The Institute of Medicine (IOM) published “Crossing the Quality Chasm,” and they noted that a large gap existed between the current care and the highest quality of care that could be provided to patients.10
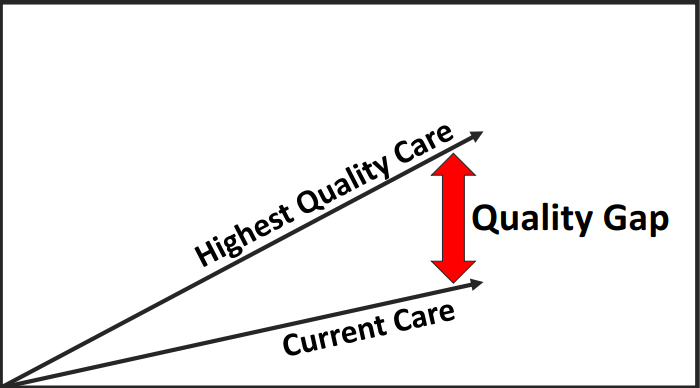
Figure 3. Defining the Quality Gap.
- The “Quality Gap” is defined as the difference between the highest quality of care and current care.
- The highest quality of care is often defined by clinical practice guidelines, best evidence, and traditionally has been shaped by what healthcare providers think their patients need.
- Current care is based on what is actually happening. What care is actually being delivered?
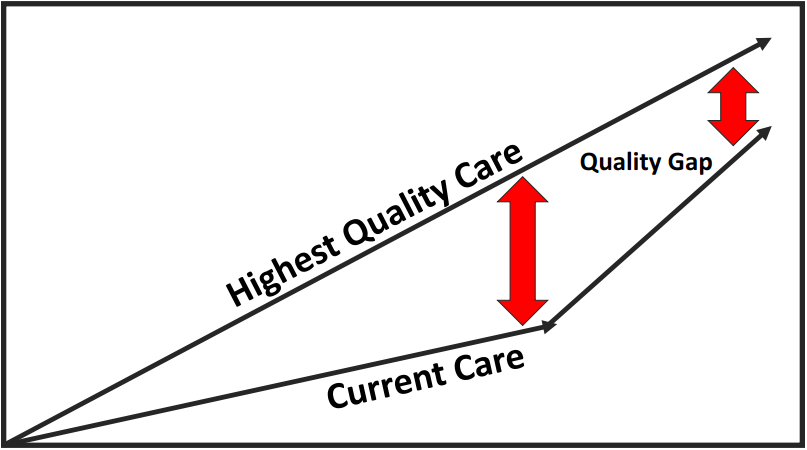
Figure 4. Closing the Quality Gap.
- Our goal is to close the gap, and this can be done by clarifying the patient’s perspective, and identifying what the patient needs to define better what the “Highest Quality Care” really is.
- Also, we can try to understand the patient experience, to better understand how our current care varies from this ideal.
The Six Domains of Quality
- The IOM defined the six domains of quality in “Crossing the Quality Chasm,” and the Agency for Healthcare Research and Quality (AHRQ) summarizes the six domains as follows:11
- Safe: Avoiding harm that originates from the care that is meant to help patients.
- Effective: Providing services based on scientific knowledge to all who could benefit and refraining from providing those services to patients not likely to benefit (avoid underuse and misuse).
- Timely: Reducing waits and sometimes harmful delays for both those who receive and those who give care.
- Efficient: Avoiding waste including waste of equipment, supplies, ideas, and energy.
- Equitable: Providing care that does not vary in quality because of personal characteristics such as gender, ethnicity, geographic location, and socioeconomic status.
- Patient-centered: Providing care that is responsive to and respectful of individual patient preferences, needs and values, and ensuring that patient values guide all clinical decisions.
The Eight Dimensions of Patient-Centered Care (PCC)
- Years of research by the Picker Institute and Harvard Medical School led to what is known as the eight dimensions of PCC, described by the Picker Institute in 1987.
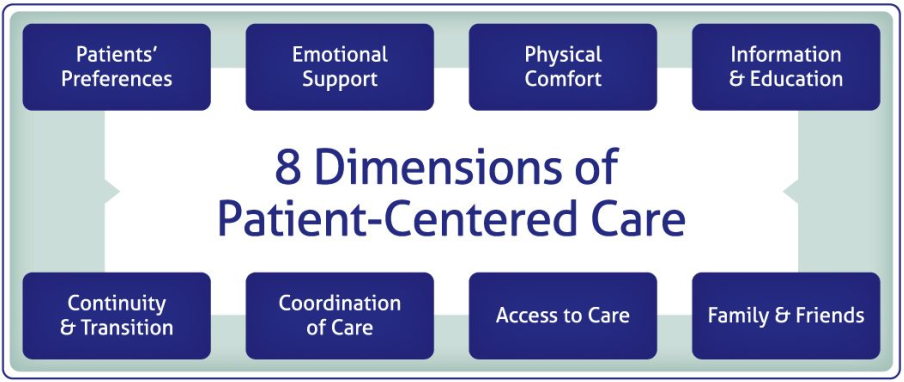
Figure 5. The 8 Dimensions of Patient-Centered Care.
- These dimensions, or principles, of PCC, were developed after thousands of interviews with patients, physicians, other hospital staff, and family members regarding their health-care experiences. The objective was to determine what matters most to patients, and this was synthesized into these eight principles.
- Considering the eight principles can be helpful when attempting to identify targets for improvement that make our care more patient-centered.
Patient Experience Literature
- Recurring themes are apparent in the patient experience literature that may allow us to improve aspects of our care from the patient’s perspective.
- Most studies use a qualitative methodology and either surveys or semi-structured interviews.
- Some notable studies from the patient experience literature and ED-specific literature, identify key themes that were problematic from the patient perspective.
- Specifically, communication problems and a lack of emotional support have been identified by patients as problematic during their hospital stay.12
- In the ED, a systematic review identified the most common problematic themes were related to communication, wait times, and empathy.13
Patient Experience with EPL Literature
- With regards to EPL in the ED, notable studies from the patient experience literature have identified similar key themes as problematic from the patient perspective.
- Most patients have reported mixed feelings about their ED experience during pregnancy loss, reporting chaos, a lack of communication, or a lack of emotional support as issues.8
- The use of judgmental or rude language was also identified as negative.
- However, clear communication and receiving information were identified as positive aspects of their ED care.
- Specifically, emotional needs and knowledge gaps were identified as problems and may be targeted for improvement.
- Women experiencing EPL often describe their miscarrying experience as a loss of life or the death of a baby, and the emotional burden associated with that loss has been described. (MacWilliams, 2016)
- Importantly, if ED providers don’t acknowledge the importance of the pregnancy loss, it can lead to marginalization, and negative perceptions of the overall care received.
- Emotional support and communication are again identified as key themes.
- Unfulfilled needs may generate dissatisfaction with the ED care received, and these fit into needs related to physical health, cognitive needs, and emotional needs. (Emond, 2019)
- Physical health relates to reducing delays in diagnostic testing, and scheduling follow-up appointments.
- Cognitive needs relate to receiving information during their visit, such as causes of EPL, frequency, and test results.
- Addressing emotional needs was important to patients, and many felt there was a gap between the intensity of their emotions and the care provided in the ED.
EPL and PCC Recommendations for Improvement
- A systematic review of 27 studies of patient experience with early pregnancy care identified key targets for improvement related to:14
- Information, communication, and education
- Emotional support
- Involvement of significant other
- Continuity and transition
- This is supported by NICE 2012 Guidelines regarding EPL care, noting the importance of:1
- Providing support and information tailored to the care women receive.
- This should relate to the extent of pain and bleeding, and the impact on fertility
- Both the US National Perinatal Association (2017) and the Canadian Public Health Agency (2017) have made similar recommendations.
- Provincially, the Ontario Provincial Council for Maternal and Child Health (PCMCH) developed recommendations for healthcare providers and staff to guide the provision of compassionate care to patients with EPL in the ED.15
- The PCMCH recommendations indicate that care should:
- Meet psychological and emotional needs
- Provide an empathetic, caring environment
- And they note that compassionate care acknowledges the loss of life
Integrating Lessons from the Patient Experience to provide PCC
- The patient experience literature can guide us on key areas for improvement in our clinical practice when caring for patients with EPL.
- We can use the literature to further guide our care for patients with EPL in the ED, and the 8 dimensions of PCC allow a framework for understanding how to operationalize National and Provincial recommendations (see Figure 6).
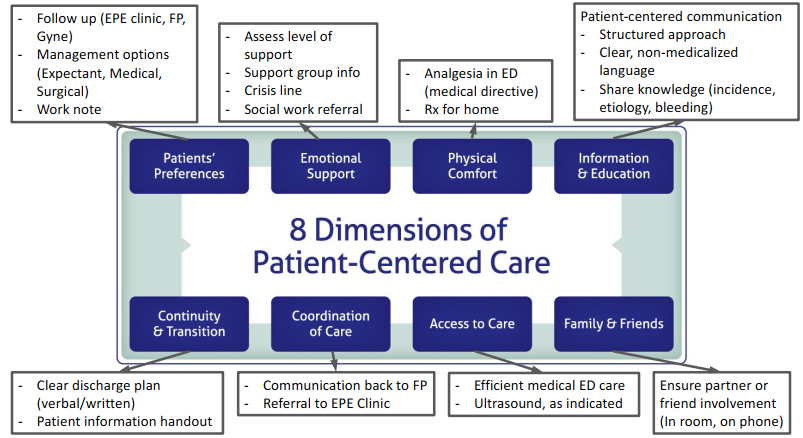
Figure 6. EPL and PCC Summary. An integrated model for how to provide PCC for patients with EPL in the ED. Recommendations are based on patient experience literature and National and Provincial recommendations.
Patient-centered communication strategies to improve care for patients with EPL
- The PCMCH recommends using a structured communication framework when informing patients that they have a confirmed or threatened EPL.
- Structured communication frameworks can help us break bad news (BBN) more effectively, and appropriately, which is important from the patient perspective.
- However, learning to BBN well can be protective for us as healthcare providers, as doing it poorly can have a negative emotional impact on the clinician,16 including feelings of:
- Guilt
- Anger
- Anxiety
- Exhaustion
- We owe it to ourselves to discover the best, or at least a better, way to BBN—we can do this by exploring how to apply structured communication frameworks.
Applying the SPIKES Model to Patients Experiencing EPL
- There are numerous structured communication frameworks for BBN, but the most commonly referenced is the SPIKES model.
- The SPIKES model was described in the early 1990s by Dr. Robert Buckman, and it continued to be refined over the next decade into six steps: Setting, Perception, Invitation, Knowledge, Emotions, and Strategy/Summary.17
- The following is a brief description of each step and practical suggestions for how to operationalize them when caring for a patient with EPL in the ED.
Setting
-
- Prepare by reviewing notes, inviting the patient to involve a significant other or friend.
- Ask if they want to call their partner to keep them involved during your discussion.
- Prepare the environment, ensuring time, and privacy.
- Try to have a private room with a door, and don’t talk in the hallway.
- Sit, don’t stand, as this increases the perception of time spent in the room.
- If you have an outstanding page, let the clerk know you will be having a sensitive conversation with another patient and will need to call the consultant back.
Perception
-
- Find out the patient’s perception of their illness.
- This is an important step in individualizing the communication with each patient, as it allows us to gauge how much information we need to share with the patient and what level of knowledge to provide.
- Use clear phrases, such as: “what do you think is going on?”; “what are you worried about today?”
Invitation
-
- This step asks for permission to share knowledge, including a diagnosis, and it serves as a way for patients to maintain their autonomy and queue them to actively listen for key information you are about to share with them.
- I think of this like a turn signal that you use while driving—you are about to change lanes, and you want to give adequate warning to other drivers on the road. Similarly, you and the patient are having a conversation—you’re both on the road—and you’re about to change lanes and perhaps share a new diagnosis.
- Signposting this change in the conversation makes it clear that you have information to share.
- Example phrases:
- “What do you know about bleeding in the first trimester?”
- “How much information do you want to know about early pregnancy loss?”
- “Can I give you some numbers that other patients find helpful?”
- The Institute for Healthcare Improvement suggests other communication techniques, including “Ask, Tell, Ask”:
- This covers three steps in the SPIKES model (Invitation, Knowledge, Emotions), and is described in a short video available here (link for video: https://www.youtube.com/watch?v=cTwektQpxUg).
Knowledge
-
- Impart knowledge clearly, avoid jargon, and use appropriate terminology.
- In the context of EPL, we want to convey that it is common, the natural history, potential risk factors or causes, and to convey our uncertainty in situations when we cannot confirm the loss.
- Use simple numbers or infographics (see Figures 1 & 2 above) to keep information clear.
- Practical Tip: I often draw these simple infographics on a piece of paper that I can give to the patient.
- I draw 3 people, circle 1; then I explain that 1 in 3 pregnancies will have first trimester bleeding (FTB).
- I draw an arrow away from that 1 person, draw 2 more people, circle 1, and I explain that about half of those women with FTB will continue with a normal pregnancy, but unfortunately, the other half will progress to lose that pregnancy.
- Bleeding is often the first sign that something is wrong, and often we don’t know when they first come to the ED which way things are going to go.
- Drawing this out for patients serves as a visual aid, and it supplements other written discharge instructions.
- Practical Tip: I often draw these simple infographics on a piece of paper that I can give to the patient.
Emotions
-
- Allowing patients to express their emotions is important.
- Pregnancy loss is a high-stakes patient encounter, from the patient’s perspective, as they have both physical and emotional needs.
- Acknowledging EPL as a loss of life is important for those with confirmed EPL, and avoiding the terms “abortion” and “fetus” are important when communicating with patients (both written and verbal).
- Using empathetic language with patients helps to acknowledge their feelings and show support.
- Examples from the PCMCH recommendations for verbal communication, specific to pregnancy loss, are as follows:

Figure 7. Examples of some “Dos and Don’ts” of verbal communication regarding EPL.
Strategy and Summary
-
- Making a plan for the future.
- In the ED, this means disposition and discharge planning.
- Arranging follow up—will this be with their family doctor, their obstetrician, or with an Early Pregnancy Evaluation Clinic.
- Ensuring adequate analgesia—discuss pain medications, consider a prescription for non-over the counter analgesia.
- Time off work—offer a work note, so they don’t need to continue to bleed or complete their loss while at work.
- Return to ED instructions—specifically, quantify the volume of bleeding that should make them come back for reassessment.
- ACOG guidelines indicate that counseling regarding bleeding should emphasize that they will likely experience bleeding heavier than menses, and may be accompanied by severe cramping. RTED if bleeding is soaking through two maxi pads per hour for 2 consecutive hours.2
- Summarize, and check for understanding.
- To summarize, the SPIKES framework is a patient-centered communication strategy that can improve our communication with patients experiencing EPL in the ED (see Figure 8).
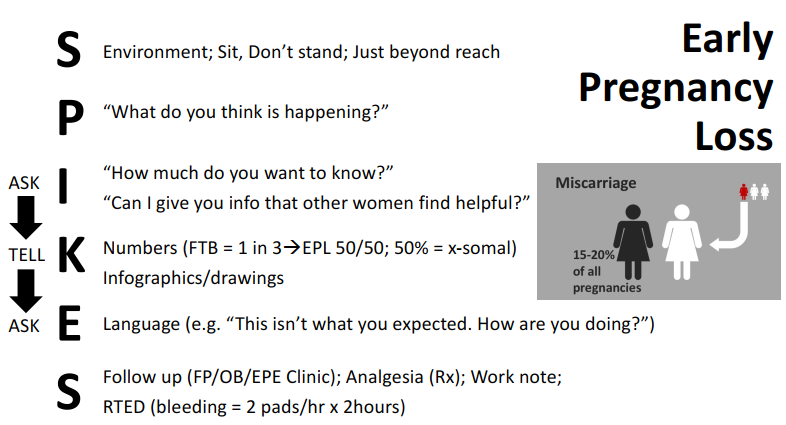
Figure 8. Summary of how the SPIKES model can be applied to facilitate patient-centered communication in patients experiencing EPL in the ED.
Summary and Recommendations
- Early Pregnancy Loss is a high-stakes patient encounter, as patients have both physical and emotional needs that are challenging to address in the ED.
- National and Provincial recommendations indicate that we need to provide patient-centered care that addresses both physical and emotional needs.
- While it is key to provide high-quality medical care, it is also vital to acknowledge the emotional burden of patients with EPL experience.
- The eight dimensions of patient-centered care provide a framework for how to improve care for patients with EPL in the ED.
- Patient-centered communication strategies help provide an informative and empathetic approach to counseling and discharge instructions.
References
- National Institute for Health, Excellence C. Ectopic pregnancy and miscarriage: Diagnosis and initial management in early pregnancy of ectopic pregnancy and miscarriage. NICE Clinical Guideline 154. December 2012.
- ACOG Practice Bulletin No. 200: Early Pregnancy Loss. Obstet Gynecol. 2018;132(5).
- Ventura SJ, Curtin SC, Abma JC, Henshaw SK. Estimated pregnancy rates and rates of pregnancy outcomes for the United States, 1990-2008. Natl Vital Stat Rep. 2012;60(7):1-21.
- Your Pregnancy: Special Considerations-Miscarriage. https://www.pregnancyinfo.ca/your-pregnancy/special-consideration/miscarriage/. Accessed July 10, 2018.
- Stephenson MD, Awartani KA, Robinson WP. Cytogenetic analysis of miscarriages from couples with recurrent miscarriage: a case-control study. Hum Reprod. 2002;17(2):446-451.
- Alijotas-Reig J, Garrido-Gimenez C. Current concepts and new trends in the diagnosis and management of recurrent miscarriage. Obstet Gynecol Surv. 2013;68(6):445-466. doi:10.1097/OGX.0b013e31828aca19.
- Nybo Andersen AM, Wohlfahrt J, Christens P, Olsen J, Melbye M. Maternal age and fetal loss: population based register linkage study. BMJ. 2000;320(7251):1708-1712.
- Baird S, Gagnon MD, deFiebre G, Briglia E, Crowder R, Prine L. Women’s experiences with early pregnancy loss in the emergency room: A qualitative study. Sexual & Reproductive Healthcare. 2018;16:113-117.
- Strommen J, Masullo L, Crowell T, Moffett P. First-Trimester Vaginal Bleeding: Patient Expectations When Presenting to the Emergency Department. Mil Med. 2017;182(11):e1824-e1826. doi:10.7205/MILMED-D-17-00108.
- Institute of Medicine. Crossing the Quality Chasm: a New Health System for the 21st Century. Washington, DC: The National Academies Press; 2001.
- Agency for Healthcare Research Quality. The Six Domains of Health Care Quality. https://www.ahrq.gov/talkingquality/measures/six-domains.html. Accessed January 23, 2019.
- Cleary PD, Edgman-Levitan S, Roberts M, et al. Patients evaluate their hospital care: a national survey. Health Aff (Millwood). 1991;10(4):254-267.
- Sonis JD, Aaronson EL, Lee RY, Philpotts LL, White BA. Emergency Department Patient Experience: A Systematic Review of the Literature. J Patient Exp. 2018;5(2):101-106.
- van den Berg MMJ, Dancet EAF, Erlikh T, van der Veen F, Goddijn M, Hajenius PJ. Patient-centered early pregnancy care: a systematic review of quantitative and qualitative studies on the perspectives of women and their partners. Hum Reprod Update. 2018;24(1):106-118. doi:10.1093/humupd/dmx030.
- Early pregnancy loss in the Emergency Department. http://www.pcmch.on.cahealth-care-providersmaternity-carepcmch-strategies-and-initiativesearly-pregnancy-loss-emergency-department. Accessed July 10, 2018.
- Bousquet G, Orri M, Winterman S, Brugiere C, Verneuil L, Revah-Levy A. Breaking Bad News in Oncology: A Metasynthesis. J Clin Oncol. 2015;33(22):2437-2443. doi:10.1200/JCO.2014.59.6759.
- Baile WF, Buckman R, Lenzi R, Glober G, Beale EA, Kudelka AP. SPIKES-A six-step protocol for delivering bad news: application to the patient with cancer. Oncologist. 2000;5(4):302-311.