There was a significant amount of pre-hospital research published in 2018; many trials were that will no doubt inform future guidelines and change practice. This post seeks to look at some of the historical features of prehospital research and give us a road map for how we got here.
Pre-Hospital Blood and Blood Products
 Original figure from author
Original figure from author
- We have known for 100 years that trauma patients needed blood.
- It has been the “unhappy lot of every surgeon in a casualty clearing station to have cases admitted under his care [which require immediate attention], but were in such a collapsed and exsanguinated condition that operation was out of the question.”
- “ the ideal time is as soon as the patient is seen” 1
So what recent data informs what type of blood products to give?
PROPPR Trial 2
 Taken from Holcomb et al.2
Taken from Holcomb et al.2
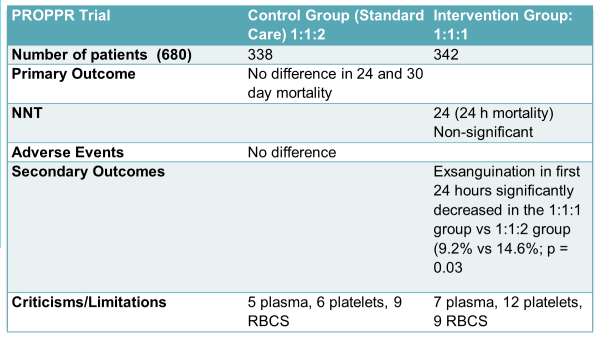
This study compared ratios of component blood therapy: Plasma, Platelets, pRBCs. In an attempt to inform us whether something resembling whole blood (1:1:1) is as safe as 1:1:2 (more red blood cells). The patients in the study didn’t get the exact ratios as described in the title, but this is a post on history, not intention to treat and per-protocol!
What actually happened in the study:
- In the 1st 24hrs, the 1:1:1 group received more total blood products (a median of 25.5 units of blood products, compared to 19 units in the other group), but similar total amounts of PRBCs
- 1:1:1 got 7 units plasma, 12 units platelets, 9 units PRBCs
- 1:1:2 got 5 units plasma, 6 units platelets, and 9 units PRBCs
 Original figure from author
Original figure from author
Bottom Line: Underpowered, but signal towards faster hemostasis in 24 hours with no increased complications in those receiving 1:1:1. Suggesting that a balanced transfusion or something resembling whole blood is safe.
So what about the prehospital world? If trauma patients need blood ASAP, should our prehospital and transport colleagues be initiating it? There’s a lot of logistics to sort out: how much, which components, refrigeration, what are the priorities in ATLS, lack of lab access, timing, etc. Let’s look at some NEW trials!
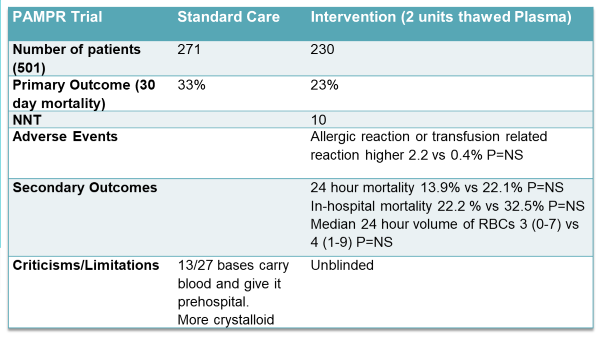
PAMPER Trial 3
 Taken from Sperry et al.3
Taken from Sperry et al.3
- This was a multicentre trial of 501 traumatized adult patients being transported via air medical
- They needed to have one episode of hypotension (SBP <90 mmHg) and/or tachycardia (HR >108 BPM) or any severe hypotension (<70 mmHg) to be included in the study
- They were given either 2 units of thawed plasma in addition to whatever the service typically did or standard of care (which could include RBCs)
- Median transport times were 40 minutes
What did they find?
 Original figure from author
Original figure from author
A 10% drop in mortality is a very large reduction for a single intervention (600 mls of plasma), but these findings are compelling. Can we do this with land-based ambulance services?
COMBAT Trial4
 Taken from Moore et al.4
Taken from Moore et al.4
- This was a single centre study of 125 adult trauma patients with SBP below 70 or an SBP between 71 and 90 with a heart rate of 108 thought to be due to bleeding.
- Randomly assigned to receive 2 units of frozen plasma or standard of care (NS)
- Median transport times <20 minutes from the time of injury
- 40% of patients in both arms received NO blood in the first 24 hours in the hospital
 Original figure from author
Original figure from author
Bottom Line: Non-Significant Difference. The 28-day mortality was 15% in the plasma group vs. 10% in the control group, p = 0.37
Interpretation
The Trauma Population best served by prehospital blood products is likely those with prolonged transport times
- Those with transport times >40 minutes will likely benefit
- Urban, rapid transport times = less benefit
- Rural/prolonged extraction, air medical = more benefit
- Logistics of carrying whole blood is a nightmare, it’s expensive, but perhaps component therapy is reasonable
- Lyophilized plasma, I think, will make a comeback–it’s available in Europe, the research groups in France have published extensively on it!
Epinephrine in cardiac arrest
The cornerstone of ACLS medications, the reason you have someone setting a timer, the best drug, with the most evidence, that you give because it is good, and does beneficial things for our patients ….Right? Right?
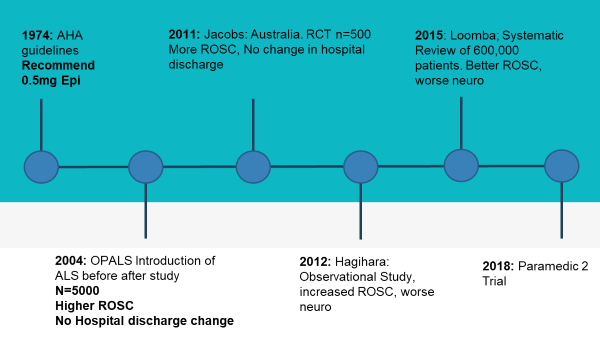 Original figure from author
Original figure from author
For an extensive review of epinephrine in cardiac arrest, please see Justin Morgenstern’s first10EM post. It should be required reading for every Emergency Physician.
Paramedic-2 Trial5
 Taken from Perkins et al.5
Taken from Perkins et al.5 Original figure from author
Original figure from author
Bottom Line: Epinephrine results in more ROSC, no difference in good neurological outcomes, and a greater proportion of bad neuro outcomes.
Interpretation
- NNT for ROSC was 112.
- Immediate high-Quality CPR and Early Defibrillation should be the mainstay of ACLS.
- The optimal dose of epinephrine is not known (if any). Upcoming trials are planned with lower dose epinephrine for out of hospital cardiac arrest.
Prehospital Airway Management
In Ontario:
- ACPs (advanced care paramedics) may perform endotracheal intubation and supraglottic airway placement.
- PCPs (primary care paramedics) may use supraglottic airways only.
- Most endotracheal intubations done in Ontario currently by ACP medics are in cardiac or traumatic arrest patients.
Questions Remain:
- Patient Safety: The available evidence does not suggest there is a benefit to patients. Outcomes such as rate of ROSC, survival at 72 hours, or intact neurological outcome from the hospital have not been shown with out-of-hospital intubation
- Training and Skills retention: The minimum number of intubations required to reach competency varies by the training program. There is currently no minimum required number of intubations once “on the road” to be certified. Airway courses and CME are available for paramedics to train and these are typically done yearly.
- Exact numbers are not available, but a convenience sample of ACPs attending airway courses in Ottawa and Kingston would indicate paramedics in Eastern Ontario attending these courses intubate on average 1-3 times per year.
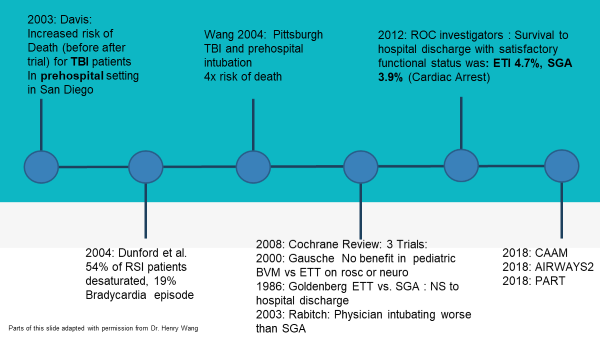 Original figure from author
Original figure from author
CAAM Trial6
 Taken from Jabre et al.6
Taken from Jabre et al.6
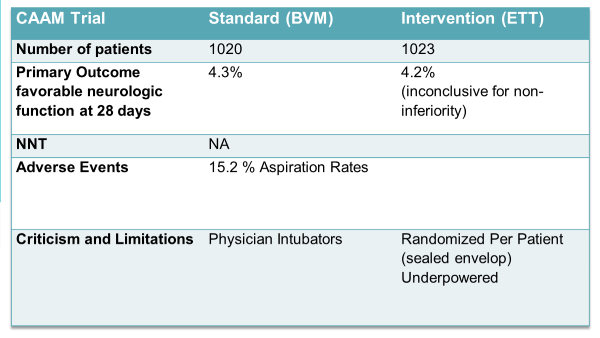 Original figure from author
Original figure from author
Bottom Line: It’s really hard to give a bottom line on this paper as it’s an inconclusive result for non-inferiority. Ryan Radceki said it best “BMV is not inferior, but not non-inferior, to ETI. This is why everyone hates Journal Club.”
Airways-2 Trial7
 Taken from Benger et al.7
Taken from Benger et al.7
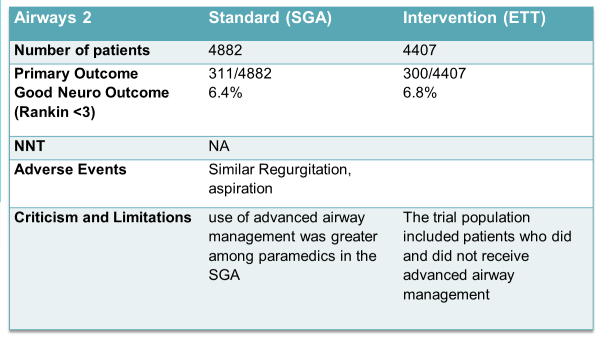 Original figure from author
Original figure from author
Bottom Line: Patients who received a supraglottic airway device compared with endotracheal intubation had a comparable neurological outcome at 30 days.
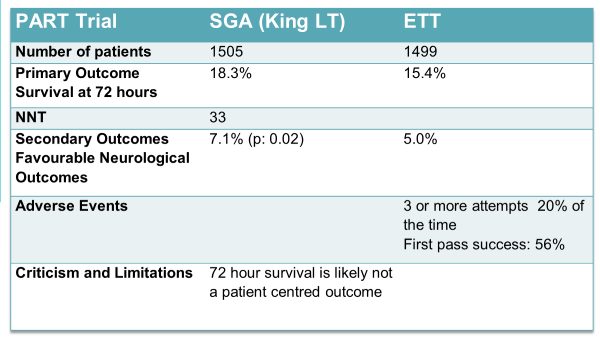
PART Trial8
 Taken from Wang et al.8
Taken from Wang et al.8
 Original figure from author
Original figure from author
Bottom Line: For the primary outcome of survival at 72 hours, the laryngeal tube was better than endotracheal intubation.
Interpretation
- The available evidence does not show a benefit to ETT vs. LMA in out of hospital cardiac arrest.
- Intubation is just one way of oxygenating and ventilating a patient, and LMAs should be thought of early in our airway and ventilation strategy.
- There are certain situations where ETT may be useful. Examples include soiled airway, complex anatomy, nasal intubation, use in place of tracheostomy, etc.
- Earlier defibrillation (when possible) and prompt, good quality CPR with minimal interruptions should be the main priorities of anyone responding to a cardiac arrest. The evidence so far isn’t great for much else!
References
- ROBERTSON LB, GORDON WATSON C. Further Observations on the Results of Blood Transfusion in War Surgery. Ann Surg. 1918;67(1):1-13. doi:10.1097/00000658-191801000-00001
- Holcomb JB, Tilley BC, Baraniuk S, et al. Transfusion of plasma, platelets, and red blood cells in a 1:1:1 vs a 1:1:2 ratio and mortality in patients with severe trauma: The PROPPR randomized clinical trial. JAMA – J Am Med Assoc. 2015;313(5):471-482. doi:10.1001/jama.2015.12
- Harbrecht BG, Daley BJ, Forsythe RM, et al. Prehospital Plasma during Air Medical Transport in Trauma Patients at Risk for Hemorrhagic Shock. N Engl J Med. 2018;379(4):315-326. doi:10.1056/nejmoa1802345
- Moore HB, Moore EE, Chapman MP, et al. Plasma-first resuscitation to treat haemorrhagic shock during emergency ground transportation in an urban area: a randomised trial. Lancet. 2018;392(10144):283-291. doi:10.1016/S0140-6736(18)31553-8
- Rees N, Finn J, Stallard N, et al. A Randomized Trial of Epinephrine in Out-of-Hospital Cardiac Arrest. N Engl J Med. 2018;379(8):711-721. doi:10.1056/nejmoa1806842
- Jabre P, Penaloza A, Pinero D, et al. Effect of bag-mask ventilation vs endotracheal intubation during cardiopulmonary resuscitation on neurological outcome after out-of-hospital cardiorespiratory arrest a randomized clinical trial. JAMA – J Am Med Assoc. 2018;319(8):779-787. doi:10.1001/jama.2018.0156
- Benger JR, Kirby K, Black S, et al. Effect of a strategy of a supraglottic airway device vs tracheal intubation during out-of-hospital cardiac arrest on functional outcome the AIRWAYS-2 randomized clinical trial. JAMA – J Am Med Assoc. 2018;320(8):779-791. doi:10.1001/jama.2018.11597
- Wang HE, Schmicker RH, Daya MR, et al. Effect of a strategy of initial laryngeal tube insertion vs endotracheal intubation on 72-hour survival in adults with out-of-hospital cardiac arrest a randomized clinical trial. JAMA – J Am Med Assoc. 2018;320(8):769-778. doi:10.1001/jama.2018.7044