
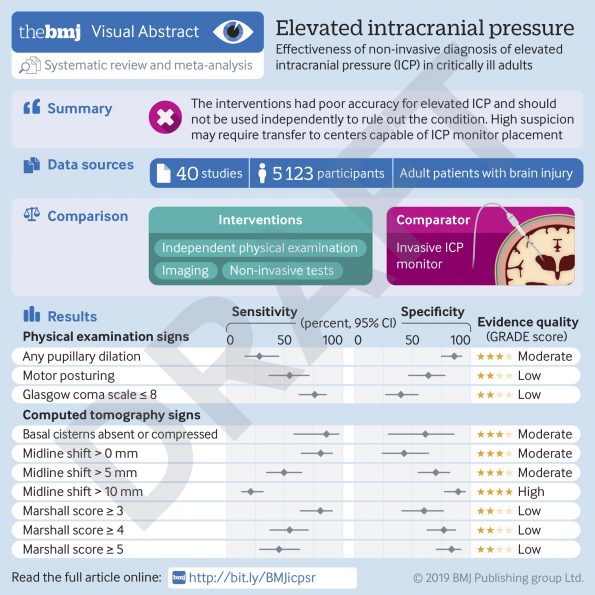
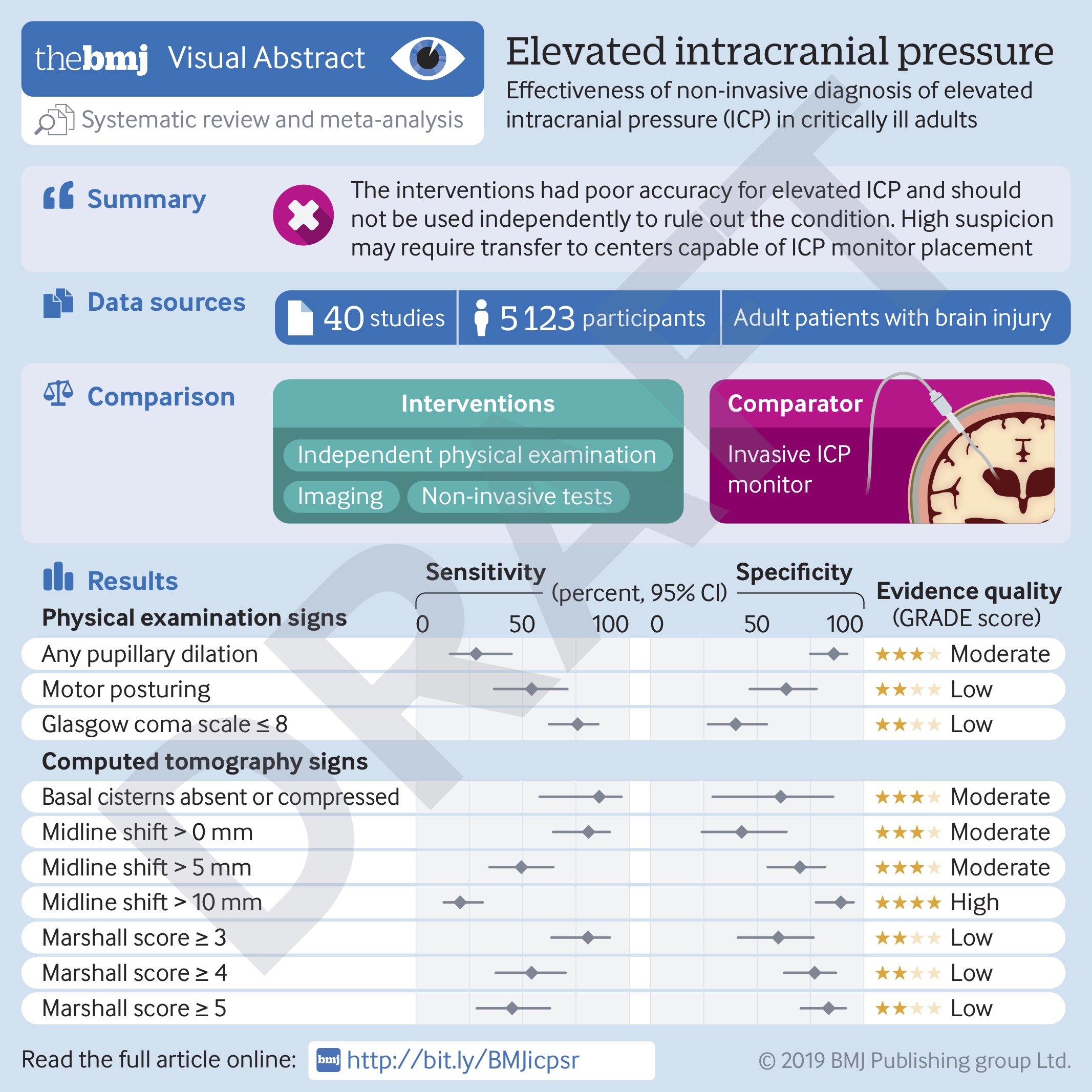
In the Emergency Department (ED) and Intensive Care Unit (ICU), we often encounter patients with brain injury. This includes patients with traumatic brain injury (TBI), subarachnoid hemorrhage (SAH), and intracerebral hemorrhage (ICH), among others [1]. In the ED and ICU, our management of these patients is namely focused upon the prevention of secondary brain injury, and this often involves avoidance of elevated intracranial pressure (ICP). Sustained elevated ICP can lead to cerebral ischemia, brain herniation, and death [2]. Definitive diagnosis of elevated ICP requires insertion of an invasive monitor, though this method can be associated with important complications, such as hemorrhage and infection [3, 4]. Therefore, ED and ICU clinicians are often tasked with using non-invasive tests for the diagnosis of elevated ICP, including physical examination, computed tomography (CT) imaging, and more recently, sonography of the optic nerve sheath diameter (ONSD) [5]. Clinicians may in fact base decisions around acute treatment or transfer to a specialized centre on such non-invasive indicators. However, the accuracy of these tests is unknown. We performed a systematic review and meta-analysis to evaluate these tests, as compared to the gold-standard of ICP ≥ 20 mmHg on an invasive ICP monitor.
Physical Examination
Several physical examination findings have been classically associated with elevated ICP. This includes pupillary dilation, motor posturing, and decreased level of consciousness. When evaluated in the available literature however, the pooled accuracy of these tools was found to be poor. Pupillary dilation (either monocular or binocular) had a sensitivity of 28.2%, but a specificity of 85.9%. Motor posturing (defined by a Glasgow Coma Scale [GCS] motor score of 3 or less) had a sensitivity of 54.3% and a specificity of 63.6%. Finally, decreased level of consciousness (defined by a total GCS of 8 or less) had a sensitivity of 75.8% and a specificity of 39.9%. Taken together, the poor sensitivity of these physical examination findings suggests that none of them should be individually used to rule out the diagnosis of elevated ICP. Only pupillary dilation had a suitable specificity, but this may reflect the fact that this is often a later sign of elevated ICP. It is important to note that, in practice, we often use a combination of physical exam features to diagnose ICP, but such combinations were not evaluated in the available literature.
Imaging
The most common imaging modality used in the evaluation of patients with brain injury is computed tomography (CT). Similar to the physical examination, there are several classic signs on CT imaging that have been associated with elevated ICP, including absence or compression of the basal cisterns, and midline shift. When evaluated independently, these signs similarly showed poor accuracy for diagnosis of ICP ≥ 20 mmHg. Absence or compression of the basal cisterns had a sensitivity of 85.9%, but a specificity of 61.0%. Any midline shift had a sensitivity of 85.9%, and a specificity of 61.0%. This serves as an important reminder that patients with diffuse edema following brain injury can still have elevated ICP without evidence of shift on CT. Finally, significant midline shift (defined as ≥ 10mm) had a sensitivity of 20.7%, but a specificity of 89.2%. Again, the individual use of these CT signs for the diagnosis of elevated ICP should be recommended against. Importantly, CT may not even be available in all centres where these patients are evaluated.
Sonography of the Optic Nerve Sheath Diameter
ONSD sonography for the diagnosis of elevated ICP has been growing in popularity [6]. Unfortunately, the use of this tool has outpaced the evidence. We initially sought to conduct a meta-analysis of ONSD sonography, but we found that the threshold used for diagnosis of “elevated ICP” varied quite significantly between studies. As a result, we were limited to meta-analysis of the area under the receiver operating characteristic curve (AUROC), which was relatively high at 0.94. Unfortunately, while the AUROC can tell you the overall accuracy of a model or tool, its clinical utility is limited. For example, in the ED, we care far more about the sensitivity of a tool, rather than the AUROC, as we try to limit missed cases (false negatives). Given the significant lack of evidence surrounding the use of ONSD in elevated ICP, clinicians should exercise great caution in using it for clinical decision-making.
How can I use this evidence to care for my patients?
Truthfully, we set out to do this study so we could identify factors that were reliable in the diagnosis of elevated ICP. After all, we have been teaching these clinical signs in medical education for decades, and several guidelines suggest that they should be utilized in deciding which patients receive invasive monitoring [7, 8]. We were in fact surprised to find that, in isolation, these factors are not reliable. Therefore, regardless of the results of these individual tests, high suspicion of elevated ICP should prompt consideration of empiric therapy, and transfer to a center capable of invasive monitoring. In EDs, clinicians may be concerned about aggressively treating ICP [9]. Similarly, the use of invasive monitoring in ICUs worldwide vary considerably [10]. Realistically, the risks of ICP management and invasive monitoring are often outweighed by the concern of untreated, elevated ICP. The latter is what we should prioritize in the care of our patients with brain injury.
https://www.bmj.com/content/366/bmj.l4225
References
- Long B, Koyfman A. Secondary Gains: Advances in Neurotrauma Management. Emerg Med Clin North Am 2018;36:107-133.
- Citerio G, Andrews PJ. Intracranial pressure. Part two: Clinical applications and technology. Intensive Care Med 2004;30:1882-1885.
- Holloway KL, Barnes T, Choi S et al. Ventriculostomy infections: the effect of monitoring duration and catheter exchange in 584 patients. J Neurosurg 1996;85:419-424.
- Binz DD, Toussaint LG, 3rd, Friedman JA. Hemorrhagic complications of ventriculostomy placement: a meta-analysis. Neurocrit Care 2009;10:253-256.
- Rosenberg JB, Shiloh AL, Savel RH et al. Non-invasive methods of estimating intracranial pressure. Neurocrit Care 2011;15:599-608.
- Geeraerts T, Launey Y, Martin L et al. Ultrasonography of the optic nerve sheath may be useful for detecting raised intracranial pressure after severe brain injury. Intensive Care Med 2007;33:1704-1711.
- Carney N, Totten AM, O’Reilly C et al. Guidelines for the Management of Severe Traumatic Brain Injury, Fourth Edition. Neurosurgery 2017;80:6-15.
- Hemphill JC, 3rd, Greenberg SM, Anderson CS et al. Guidelines for the Management of Spontaneous Intracerebral Hemorrhage: A Guideline for Healthcare Professionals From the American Heart Association/American Stroke Association. Stroke 2015;46:2032-2060.
- Gottlieb M, Bailitz J. Does Mannitol Reduce Mortality From Traumatic Brain Injury? Ann Emerg Med 2016;67:83-85.
- Cnossen MC, Huijben JA, van der Jagt M et al. Variation in monitoring and treatment policies for intracranial hypertension in traumatic brain injury: a survey in 66 neurotrauma centers participating in the CENTER-TBI study. Crit Care 2017;21:233.
