

Anorectal issues commonly present to the Emergency Department (ED), however, the evidence around many of these conditions is sparse and practice varies widely. ED providers should have a grasp on the management and disposition of common anorectal complaints. In part one of this two-part series we will be focusing on issues related to hemorrhoids and anal fissures.
Where relevant, we will share expert opinion by Dr. H. Moloo (Division Head, Colorectal Surgery, The Ottawa Hospital), to provide context.
Hemorrhoids
- Hemorrhoidal vessels are normal structures that improve resting rectal tone and cushion the anal sphincters during defecation.1
- Symptomatic hemorrhoids result from dilatory distortion of the vascular channels and destructive changes in connective tissue. This results in various degrees of prolapse, which is thought to drive symptoms.2
- Recent case series and population studies do not back up classical risk factors like pregnancy, hard stool, and prolonged toilet time.1
- Symptomatic hemorrhoids can present with bleeding, pruritus, fullness, discharge, burning, and pain.2
- Up to half of hemorrhoids that can be visualized on anoscopy are not associated with symptoms.3
- Up to 5% of the US population suffers from symptomatic hemorrhoids at any given time.1
From Sandler RS, Peery AF. Rethinking what we know about hemorrhoids. Clinical gastroenterology and hepatology, 2019.
![]() Classification
Classification
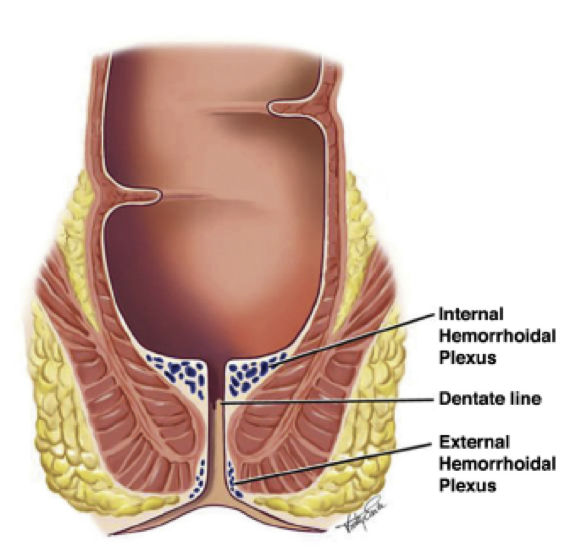
Hemorrhoids can be divided into 2 categories, based on whether the prolapsing culprit is proximal or distal to the dentate line.
- Internal hemorrhoids are proximal to the dentate line and are covered in columnar epithelium, which does not have pain fibers. These present with painless bleeding, fullness, discharge, and pruritis. The Goligher classification of internal hemorrhoids is based on prolapse and reducibility:
- Grade 1: do not prolapse at all
- Grade 2: prolapse with strain and self-reduce
- Grade 3: prolapse with strain and can be manually reduced
- Grade 4: irreducible, can become strangulated, presenting as acutely painful, necrotic, foul-smelling, ulcerated lesions.1
- External hemorrhoids are distal to the dentate line and are covered in anoderm, which has pain fibers. These present with bleeding, fullness, discharge, pruritis, and pain and burning on defecation.
- A colour change, swelling, and/or a palpable clot suggest a thrombosed external hemorrhoid, which is exquisitely tender on defection, intercourse, and even sitting or walking.2
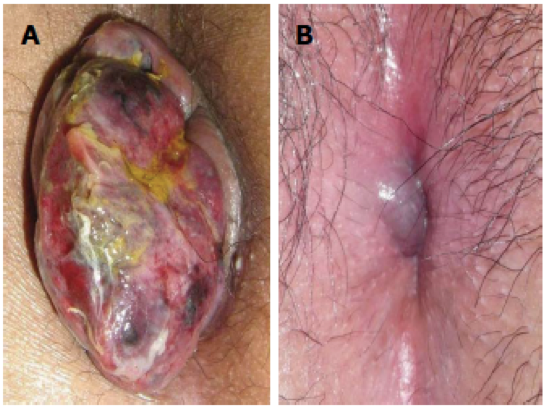
Complicated hemorrhoids. A: Strangulated internal hemorrhoid; B: Acutely thromboses external hemorrhoid. From Lohsiriwat V. Treatment of hemorrhoids: a coloproctologist’s view. World journal of gastroenterology, 2015.
Management – Internal Hemorrhoids
The American Society of Colon and Rectal Surgeons (ASCR) suggests warm water (“sitz”) immersion, oral analgesia, stool softener, and high fibre as first-line management of hemorrhoids.4 However, of these therapies, only fibre has any literature surrounding its use. A systematic review in 20065 identified 7 studies with a total of 378 patients looking at fibre for hemorrhoids: the most recent was performed in 1996 and overall there were concerns with blinding, concealment, and loss to follow-up. Overall, however, the meta-analysis showed fibre having statistically significant benefit for bleeding (RR=0.5) and overall improvement (RR=0.53) with a minimal side effect profile. Local practice at The Ottawa Hospital (TOH) is to recommend 25-30g of fibre a day.16
Of note, the ASCR does not recommend topical preparations for hemorrhoid therapy as there are no studies evincing benefit and these medications carry the risk of sensitization and contact dermatitis.4
Phlebotonics
Phlebotonics are a diverse family of plant-derived and semisynthetic compounds whose proposed method of action is to strengthen blood vessel walls, increase venous tone, improve lymphatic drainage, and normalize capillary permeability. Though not common in Canada, they can be used to treat varicose veins and symptomatic hemorrhoids. A Cochrane meta-analysis and systematic review of phlebotonics for hemorrhoids6 found 24 studies involving 2334 patients. Multiple formulations, variable quality, multiple endpoints, and multiple confounders mean that results should be interpreted with caution. However, there was a statistically significant benefit for the reduction of bleeding (OR=0.12), discharge (OR=0.12), and overall benefit (OR=15.98), with a beneficial trend for pain and pruritis. There was a minimal side effect profile involving gastrointestinal discomfort. The only phlebotonic approved for sale in Canada is MPFF (micronized purified flavonoid fraction) under the trade name VenixxaTM, which was used in 13 of the 24 studies included in the Cochrane review. It is sold over the counter. A single box costs approximately 32$ and contains a full course of treatment (1500mg BID for 4 days, then 1000mg BID for 3 days).7
Management – External Hemorrhoids
Much of the literature around hemorrhoids focuses specifically on internal hemorrhoid management. Regarding external hemorrhoids, and specifically thrombosed external hemorrhoids, there is significant practice variation around incision and expression of clot. A single systematic review without meta-analysis8 identified only two papers comparing surgical and supportive therapy for thrombosed external hemorrhoid: while surgical outcomes were promising (significant difference in resolution of symptoms after four days), the procedures performed were overwhelmingly excision of clot and hemorrhoid, as opposed to incision. Given the real risk of bleeding, wound infection, prolonged pain, and poor wound healing, incision and expression of clot is not recommended in the ED, and surgical consultation should be considered if immediate pain relief is desired.16
Anal Fissures
Anal fissures are local defects (or ulceration) in the anoderm that should be visible on inspection. They present with rectal bleeding and significant pain, often triggered by defecation but lasting for several hours after the event; this pain is thought to be the result of hypertonic anal sphincter spasm and resultant ischemia.9
Fissures have a waxing and waning course, with a high rate of recurrence in 1 year. They may be primary, which the ASCR defines as less than 8 weeks, or chronic, which are persistent for longer than 8 weeks and display chronic changes such as hypertrophied anal papillae, sentinel skin tags, cryptitis, or anal fistulae.9,10 The pathophysiology of fissures is controversial, as are classical risk factors such as hard stool, increased resting rectal tone, and anal trauma. Crohn’s patients are especially prone to anal fissures.9 Fissures are most commonly midline, either posterior or anterior: multiple anal fissures, as well as fissures that are offset from midline, may represent manifestations of systemic disease, such as Crohn’s, TB, syphilis, or HIV.11

Primary fissure. From Wienert V, Raulf F, Mlitz H. Anal fissure. Springer, 2017.

Chronic fissure displaying several changes of chronicity. From Wienert V, Raulf F, Mlitz H. Anal fissure. Springer, 2017.
Management
The ASCR recommends supportive therapy as first-line management for fissures, with surgical management reserved for those that fail.12 A Cochrane review and meta-analysis of conservative anal fissure management in 201213 revealed a crowded field: 75 RCTs with 15 agents, involving 5031 patients. Multiple outcome measures, issues with randomization, allocation, and concealment, with an overall GRADE score of “low,” limit the reliability of its included studies. ED-available therapies included in this systematic review included sitz baths, topical lidocaine, topical hydrocortisone, fibre, and smooth muscle relaxing agents.
Sitz baths
Sitz baths were found in a single 2006 study to have no significant difference in healing rates as compared to placebo, though patients expressed greater satisfaction with the former.14 15 minutes in lukewarm water QID PRN is a common approach, especially after each bowel movement.
Fibre and Topicals
A single study was identified looking at topical lidocaine as compared to topical hydrocortisone cream or fibre (in this case, bran). Both topical hydrocortisone and fibre had a statistically significant benefit for healing (OR 3.33) compared to lidocaine.13 As before, TOH’s colorectal team recommends 25-30g of fibre daily for the management of anal fissures.16
The two ED-available smooth muscle relaxing agents included in the Cochrane review were nitroglycerin and calcium channel blockers.13 Nitroglycerin was found to have a statistically significant benefit for healing with a modest ARR (13.4%) but a 30% increase in headache as compared to placebo (NNT of 7.5, NNH of 3.3, which is less than ideal). CCBs were found to have no statistically significant difference in nonhealing rates as compared to nitroglycerin, but with a much better side effect profile in general, and for headaches in particular.
Neither nitroglycerin nor CCBs seemed to exhibit a dose-dependent response.13 Nifedipine 0.3% ointment (with or without lidocaine) is therefore the smooth muscle relaxer of choice, to be applied TID and after defecation. In Canada, this preparation must be compounded as it is not available commercially. Some experts recommend combining it with a petroleum base to increase comfort.
Take Home Points
Hemorrhoids:
- Reconsider the diagnosis
- Fibre (25-30g daily) and oral analgesia are reasonable first line therapies
- Consider topical therapy, understanding the lack of evidence and risk of sensitization
- Consider MPFF at 1500mg BID for 4 days, then 1000mg BID for 3 days
- Consider outpatient referral for all hemorrhoidal disease
- Consider in-house surgical referral for strangulated grade 4 internal hemorrhoids
- Instead of incision and expression of clot for thrombosed external hemorrhoids, consider in-house surgical referral for excision
Anal fissures:
- Consider systemic disease in multiple fissures or fissures located off midline
- Consider oral analgesia, fibre, topical hydrocortisone, and topical nifedipine (0.3% TID and after defecation)
- Consider outpatient surgical referral
References
- Sandler RS, Peery AF. Rethinking what we know about hemorrhoids. Clinical gastroenterology and hepatology, 2019
- Lohsiriwat V. Treatment of hemorrhoids: a coloproctologist’s view. World journal of gastroenterology, 2015
- Riss S, Weiser FA, Schwameis K, Riss T, Mittlböck M, Steiner G, Stift A. The prevalence of hemorrhoids in adults. International journal of colorectal disease, 2012
- Davis BR, Lee-Kong SA, Migaly J, Feingold DL, Steele SR. The American society of colon and rectal surgeons clinical practice guidelines for the management of hemorrhoids. Diseases of the colon and rectum, 2018
- Alonso-Coello P, Mills E, Heels-Ansdell D, Lopez-Yarto M, Zhou Q,Johanson JF. Fiber for the treatment of hemorrhoids complications: a systematic review and meta-analysis. American journal of gastroenterology, 2006
- Perera N, Liolitsa D, Iype S, Croxford A, Yassin M, Lang P, Ukaegbu O, van Issum C. Phlebotonics for haemorrhoids (review). The Cochrane collaboration, 2012
- https://venixxa.ca accessed October 8 2019
- Chan KKW, Arthur JDR. External haemorrhoidal thrombosis: evidence for current management. Techniques in coloproctology, 2013
- Herzig DO, Lu KC. Anal fissure. Surgical clinics of North America, 2010
- Wienert V, Raulf F, Mlitz Anal fissure. Springer, 2017.
- Stewart DB Sr., Gaertner W, Glasgow S, Migaly J, Feingold D, Steele SR. The American society of colon and rectal surgeons clinical practice guideline for the management of anal fissures. Diseases of the colon and rectum, 2017
- Nelson RL, Thomas K, Morgan J, Jones A. Nonsurgical management of anal fissures (Review). The Cochrane collaboration, 2012
- Gupta PJ. Randomized, controlled study comparing sitz-bath and no-sitz-bath treatments in patients with acute anal fissures. ANZ journal of surgery, 2006



Trackbacks/Pingbacks