

An 84-year-old male presented to the ED after a fall. The patient is confused but he talks about the fire truck ride with the “lights”. He knows the city and the month, but doesn’t know why he’s here. On exam, he has long hair, a full beard, sunken cheeks, and bilateral raccoon eyes which were now almost at his jaw. He has bruising on his biceps, sternum, abdomen, and thighs, at various stages of healing. His clothes are soiled, and his toenails overgrown. He’s moving all four limbs spontaneously with increased tone, and cogwheeling in the upper extremities with a noticeable tremor at rest.
On review of his medical records, there were no hospital visits for over 20 years. Provincial database showed no blood work, no images, no other ED visits, and no medications filled in almost 4 years, including Parkinson’s medications. The nurse hands me his health card, which had expired 4 years ago, and says “doesn’t he look different?” His health card shows him with a crew cut, clean-shaven and full cheeks.
An hour or so later the police arrive. The bank had called them due to concerns about the patient’s wellbeing. They reached his POA, who told them the patient falls “all the time” and is unclear how long the bruises under his eyes have been there, probably less than a week. They then said they needed to get back to work and hung up.
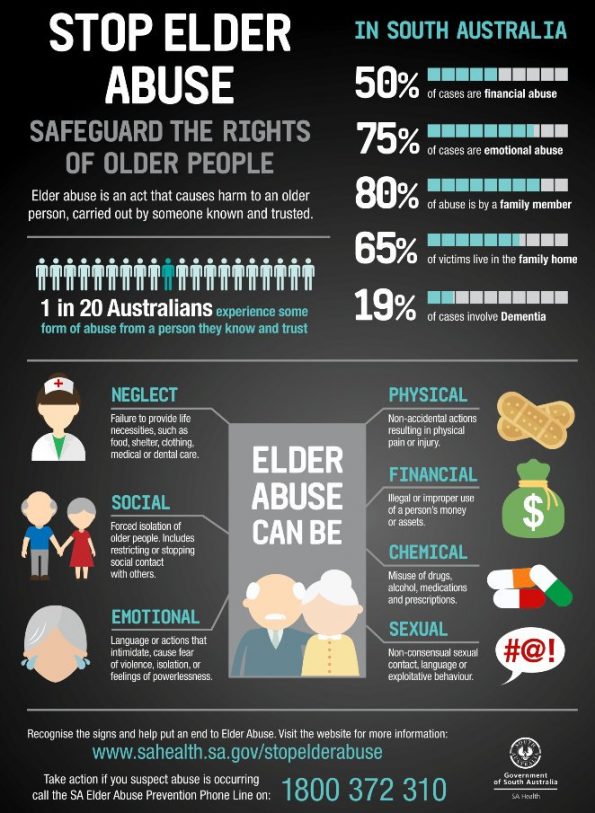
*This is a poster located in a public restroom at a healthcare facility in Australia
Elder Abuse
Elder abuse can be loosely defined as any action or inaction that results in harm or distress of an older person by someone they trust. It comes in many shapes and sizes, and in classic Rosen’s fashion, is summarized in a table:1

Current estimates place the incidence of elder abuse in Canada between 4 and 10%. Police reported violent crimes committed against seniors have been steadily increasing over the last decade. Over a third of those crimes were committed by a family member, and almost half of the victims sustained a physical injury. Women were slightly more likely to be injured (58%) than male seniors.2
If these are the crimes that are being reported, imagine what we are missing, given that less than one in five incidents of elder abuse are reported.3
True or False?
1. Elder abuse is a crime in Canada
False. It is not listed in the Canadian Criminal Code as a specific crime. There are various components that fall into other areas like assault, theft, or failure to provide the necessities of life.
2. Elder abuse is mandatory for physicians to report in Canada
False. In Canada, there are no federal laws making elder abuse reporting mandatory.
- HOWEVER, there are some provinces and territories that do.
- For individual provinces check out this great summary from the Canadian Centre for Elder Law (summary table pages 49-51)4
- If the patient is a resident of health care facility (LTC, NH, RH, etc)
- Mandatory in most provinces but not nationwide
- Who you report it to also varies by province (government versus social worker)
- If the patient is residing in community:
- Not mandatory to report except in Nova Scotia, Newfoundland and Labrador, and the Northwest Territories
- Most provinces state “may” report but no formal obligation or duty to report.
Furthermore, reporting could get you in trouble. From the CMPA statement on elder abuse, “physicians similarly do not have a duty to report a criminal offence related to elder abuse to the police. This would generally be considered a breach of confidentiality unless there was consent from the patient or substitute decision-maker”.5
Ontario mandatory reporting
Under the Long-Term Care Homes Act, health professionals are mandated to report the following to the Ministry of Health and Long-Term Care Director:6
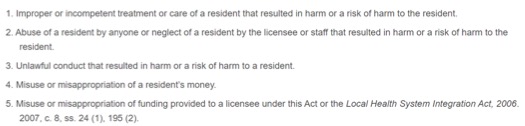
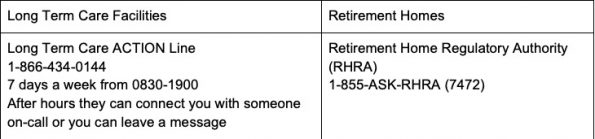
You can notify the Ministry based on what kind of facility the patient is in:7
The details of what is mandatory is interesting because it means that any harms that happens to a resident should be reported including harm by family members, other residents, and even visitors to other residents. This is something that may not be obvious that we need to report.
In addition, “incompetent treatment that causes harm” is listed but neither incompetence nor harm are really defined. What about near misses, when something incompetent happened but no real harm occurs to the patient? For example, if there is a medication administration error where a patient receives too many or the wrong kind of pills? Not all overdoses are harmful, but some could be fatal. It would be helpful to have some discussion around what that means. Particularly because the Act says that if you fail to report abuse, you may be guilty of an offense and fined up to $25,000.
What about when it is not mandatory?
It is very difficult for physicians to watch a vulnerable person return to a harmful situation. We are left feeling somewhat useless and struggle to know if we are doing “the right thing.” When you are seeing a community dwelling elderly patient who you suspect is being abused, first assess their capacity. All persons are presumed to be capable unless proven otherwise, meaning they can understand information to make decisions for themselves (resources for assessing capacity 8-11).
Incapable patients
If you find that the patient is incapable, then you need to discuss any treatment plans with their power of attorney (POA) or substitute decision maker (SDM). Where this gets tricky is when you suspect the POA/SDM may be the perpetrator of the abuse because sadly there aren’t any laws prohibiting them from acting as the POA/SDM. If you have concerns, you can ask for proof of POA because they should have some form of documentation to prove it. If they cannot provide it, then they may still be an SDM. However, you can then look for alternate on the SDM hierarchy who is either higher or at the same level with equal decision-making status.10
Furthermore, the SDM must act in the “best interests of the patient”.12 Things like leaving against medical advice or preventing homecare services for personal hygiene from entering the home would likely not be in the best interests of the patient. If a physician feels an SDM is not acting in accordance with the Health Care Consent Act, the SDM can be challenged. This can occur through your local Consent and Capacity Board (CCB) or the Office of the Public Guardian and Trustee (OPGT) Guardianship Investigations team (1-800-366-0335). The OPGT can only act in situations where the patient is incapable, and in cases of elder abuse, they can apply for temporary guardianship of the abused patient.13 Another useful resource, if you have one, is your institution’s ethicist, who could provide you with advice and help mobilize the CCB.
Capable patients
People are allowed to make bad decisions, and in the emergency department we often see the consequences of those decisions. If the patient is capable, then they can choose to return to an unsafe situation. However, you should talk to your patient. Don’t dance around the issue. Voice your concerns. Ask for their consent to discuss your concerns with others like social workers, their family physician, or the police. If they agree, document the conversation and make some phone calls. If they don’t consent, offer them resources. Some examples of local and provincial resources are listed here. A national list put together by the Government of Canada can be accessed here (14).
Senior Safety Line
- 1-866-299-1011
- Available 24 hours a day/7 days a week in over 150 languages
- Provides contact and referral information for local agencies across the province that can assist in cases of elder abuse. Trained counsellors also provide safety planning and supportive counselling for older adults who are being abused or at risk of abuse. Family members and service providers can also call for information about community services.
Local Police Service
-
Most have an elder abuse division or section
- Ottawa Police Services – Elder Abuse section: 613-236-1222 EXT 5945 M-F 0800-1600
Elder Abuse Ontario
http://www.elderabuseontario.com
Fantastic website with resources for community, regional and national supports and services that are arranged by location
Elder Abuse Response/Referral Service Programs
Typically operated by local community centres or healthcare networks that can send teams to visit patients at home to ensure they are safe
References:
- Rosen, T. and Stern, M.E.(2017) Chapter 186 – Abuse and Neglect of the Geriatric Patient. Rosen’s Emergency Medicine: Concepts and Clinical Practice 9th Edition, Springer; 2017:2341-2348.
- https://www150.statcan.gc.ca/n1/pub/85-002-x/2018001/article/54978/03-eng.htm
- https://www.canada.ca/en/public-health/services/health-promotion/aging-seniors/elder-abuse.html
- https://www.bcli.org/project/practical-guide-elder-abuse-and-neglect-law-canada
- https://www.cmpa-acpm.ca/en/advice-publications/browse-articles/2016/elder-abuse-and-neglect-balancing-intervention-and-patients-right-to-confidentiality
- https://www.ontario.ca/laws/statute/07l08
- http://www.elderabuseontario.com/what-is-elder-abuse/legislation-reporting/
- https://www.cmpa-acpm.ca/en/advice-publications/browse-articles/2011/is-this-patient-capable-of-consenting
- https://www.cpso.on.ca/uploadedFiles/policies/policies/policyitems/capacity_consent_july07dialogue.pdf
- https://www.cpso.on.ca/Policies-Publications/Policy/Consent-to-Medical-Treatment
- Aid to Capacity Evaluation – Joint Centre for Bioethics http://www.jcb.utoronto.ca/tools/documents/ace.pdf
- http://www.royalcollege.ca/rcsite/bioethics/cases/section-1/elder-abuse-neglect-e
- https://www.attorneygeneral.jus.gov.on.ca/english/family/pgt/guardinvestigation.html
- https://www.canada.ca/en/employment-social-development/campaigns/elder-abuse/resources-province-territory.html
