

What is nurse-led ACLS (Advanced Cardiac Life Support)?
A resuscitation model where a nurse takes on a leadership role coordinating and running the ACLS algorithm as part of the overall resuscitation effort. Nursing leadership has always played an integral role in hospital resuscitations, however, it has traditionally been in an unofficial capacity. Nurse-led ACLS is a concept that has been gaining traction more recently in social media circles and some centres, but there is a fair amount of confusion over how this model actually works. In this post, I will try to dispel some of these misconceptions about nurse-led ACLS, and provide some supporting evidence (when available), then propose a model of nurse-led ACLS and allow you to compare it to other models currently in use in other centres.

How is nurse-led ACLS different?
First, lets compare traditional ACLS to nurse-led ACLS:
- In traditional ACLS the physician is the sole lead and is expected to remember to assign team roles, ensure high-quality CPR, coordinate resources, order ACLS therapies on time, review the patient’s medical conditions, figure out why they have arrested, think about the need to divert from the ACLS algorithm, call for consults and manage other physicians doing procedures.
- How many of us have ever thought: “that felt like a very long pulse check”, “wait, how long has it been since the last shock?”, “how have we only given epinephrine twice in the last 15 minutes?” or “did anyone actually give the amiodarone?” It has likely happened to all of us in some form or another.
- In nurse-led ACLS the lead physician can cognitively offload the ACLS component while still ensuring that treatments are delivered effectively. That physician can then go ahead and focus on the specific therapies best suited for this particular patient.
Dispelling the myths
Myth 1: Running ACLS is outside of the nursing scope of practice
-
- Registered nurses (RNs) are required to be certified in ACLS. The ACLS course is specifically created to teach the provider how to recognize and intervene on cardiac arrests and other cardiovascular emergencies through the application of ACLS principles1.
- The reality is that RNs carry the same certificate that physicians do, and are absolutely equipped to deliver high-quality ACLS.
- A study performed by Gilligan et al. compared the abilities of RNs to junior residents to run ACLS simulation scenarios and found similar performance2. Since we know that junior residents can be trained to run high-quality ACLS codes, this suggests that RNs can do the same.
- There is some evidence to suggest that nursing leadership is beneficial to resuscitation quality. Leary et al showed that the implementation of a nurse-physician dyad in their centre led to a reduction in room crowding without harming leadership clarity3.
- Clements et al. were able to demonstrate that nurse leaders could effectively manage patients with high mortality risk and that having a nurse leader could improve certain aspects of leadership and communication during traumas4,5. There are also overall associations between the emphasis of nurse empowerment and leadership, with higher hospital performance6.
Myth 2: The nurse is in charge of the entire resuscitation, not a physician
-
- This is a fundamental misunderstanding of the leadership model for nurse-led ACLS, and part of the reason that calling this model “nurse-led code” can lead to confusion.
- The model calls for a leadership dyad in which a nurse coordinates and runs the ACLS component of a cardiac arrest, while the lead physician focuses on trying to identify the underlying cause, perform “beyond-ACLS” diagnostic and therapeutic procedures and maintain overall control over the resuscitation without having to micromanage it.
Myth 3: Nurse-Led ACLS is only useful in resource-limited settings
-
- Nurse-led ACLS is definitely useful in resource-limited settings. That being said it is not limited to those scenarios. Higher resource settings have the luxury of more personnel, as well as more tools at their disposal. As a result, they can strive to perform more labour-intensive diagnostics and interventions that might otherwise be unfeasible.
- We know that high-quality CPR and early defibrillation are the pillars of ACLS1. One unintended consequence of performing “beyond ACLS” diagnostic and therapeutic interventions is the delay caused to core principles. We know that pausing CPR leads to a loss of perfusion and that it takes time to return to the pre-pause level of perfusion7,8.
- There are increased durations of rhythm checks with the use of POCUS, which is further worsened when the leader is the one performing the ultrasound9,10. This is problematic because we know that longer pauses in CPR lead to lower survival11. This is a classic example of task fixation.
- Task fixation leads to a loss of situational awareness, which in turn reduces the effectiveness of leadership. Nurse-led ACLS allows the maintenance of situational awareness which in turn prevents undue interruptions to the core life-saving principles, while still allowing for the performance of higher-level interventions.
Myth 4: Physicians are good at juggling ACLS and other tasks
-
- Task fixated physicians lead to a loss of situational performance and degradation of performance. While interruptions and multitasking is a common occurrence in medicine, it is actually a major source of medical error12,13.
- Interruptions and multitasking leads to increased cognitive burden which leads to mistakes. A leadership dyad as well task delegation can decrease this burden.
- In the era of COVID-19, the approach to the airway is increasingly nuanced, and being able to offload ACLS may have a significant positive impact on capturing the airway.
Putting it all together
Let’s now see how this might look into practice:
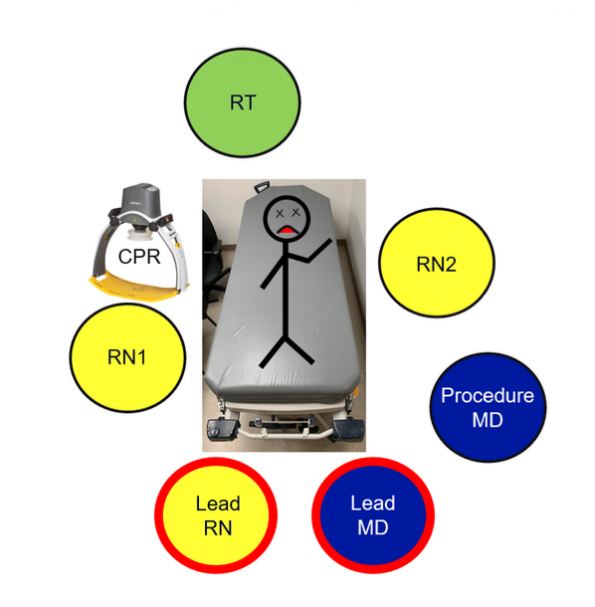
- The team composition
- Lead RN
- Lead physician
- Two bedside RNs
- One respiratory therapist
- Procedure MD
- Individuals tasked with high quality CPR (or mechanical CPR device)
- Role assignment
- The lead RN begins basic ACLS management through the coordination of CPR, pad placement, gaining IV access, delivering epinephrine every 4 minutes, making sure there is adequate ventilation, and delivering shocks and amiodarone as required.
- The lead physician may call for the procedure MD to move to the head of the bed for intubation or perform other procedures (arterial lines, gaining central access, POCUS). This frees the lead physician to step out, speak to family, look up the patient, or come up with more advanced patient-specific strategies.
- While this occurs, the lead RN keeps ACLS running smoothly and minimizing interruptions to CPR.
- At any time the lead physician can ask the lead RN to deviate from the ACLS algorithm in any way they see fit, and the lead RN would enact these changes by integrating them into the care of the patient.
- Leading by example
- There are a few centres that are currently employing this strategy of nurse-led ACLS.
- Rob Paquin and Allan Lai (Resus Tonight Podcast) showing a simulation of nurse-led ACLS that can be found here.
Take home points
- Nurse-led ACLS is a resuscitation model that utilizes a leadership dyad in order to reduce the cognitive burden of the lead physician.
- Nursing leadership may increase resuscitation performance, improve communication and reduce room crowding without creating confusion about leadership clarity.
- Having a nurse leader may reduce the risk of neglecting core ACLS principles while still allowing for the performance of higher-level diagnostic and therapeutic procedures
Nurse-led ACLS related podcasts
- Nurse Led ACLS. The Q Word Podcast. Episode 21, 2020. https://podcasts.apple.com/us/podcast/nurse-led-acls/id1407523803?i=1000463077647
- Nurse Led Code. Emcrit Podcast. Episode 204, 2017. https://emcrit.org/emcrit/nurse-led-code/
- ResusX Series – The Nurse Led Code. Resus Tonight Podcast. Episode 12, 2019. https://resustonight.com/index.php/2019/10/18/podcast-12-resusx-series-the-nurse-led-code/
References
- Heart and Stroke Foundation of Canada. https://cpr.heartandstroke.ca. Published 2020.
- Gilligan P. To lead or not to lead? Prospective controlled study of emergency nurses provision of advanced life support team leadership. Emergency Medicine Journal. 2005;22(9):628-632. doi:10.1136/emj.2004.015321.
- Leary M, Schweickert W, Neefe S, Tsypenyuk B, Falk SA, Holena DN. Improving Providers Role Definitions to Decrease Overcrowding and Improve In-Hospital Cardiac Arrest Response. American Journal of Critical Care. 2016;25(4):335-339. doi:10.4037/ajcc2016195.
- Clements A, Curtis K. What is the impact of nursing roles in hospital patient resuscitation? Australasian Emergency Nursing Journal. 2012;15(2):108-115. doi:10.1016/j.aenj.2012.01.002.
- Clements A, Curtis K, Horvat L, Shaban RZ. The effect of a nurse team leader on communication and leadership in major trauma resuscitations. International Emergency Nursing. 2015;23(1):3-7. doi:10.1016/j.ienj.2014.04.004.
- Guetterman TC, Kellenberg JE, Krein SL, et al. Nursing roles for in-hospital cardiac arrest response: higher versus lower performing hospitals. BMJ Quality & Safety. 2019;28(11):916-924. doi:10.1136/bmjqs-2019-009487.
- Berg R, Sanders A, Kern K, et al. Adverse hemodynamic effects of interrupting chest compressions for rescue breathing during cardiopulmonary resuscitation for ventricular fibrillation cardiac arrest. Circulation. 2001;104(20):2465-2470.
- Cunningham L, Mattu A, O’Connor R, Brady W. Cardiopulmonary resuscitation for cardiac arrest: the importance of uninterrupted chest compressions in cardiac arrest resuscitation. Am J Emerg Med. 2012;30(8):1630-1638.
- Clattenburg EJ, Wroe P, Brown S, et al. Point-of-care ultrasound use in patients with cardiac arrest is associated prolonged cardiopulmonary resuscitation pauses: A prospective cohort study. Resuscitation. 2018;122:65-68. doi:10.1016/j.resuscitation.2017.11.056.
- Maite A. Huis In t Veld, Allison MG, Bostick DS, et al. Ultrasound use during cardiopulmonary resuscitation is associated with delays in chest compressions. Resuscitation. 2017;119:95-98. doi:10.1016/j.resuscitation.2017.07.021.
- Cheskes S, Schmicker R, Christenson J, et al. Perishock pause: an independent predictor of survival from out-of-hospital shockable cardiac arrest. Circulation. 2011;124(1):58-66.
- Krimminger D, Sona C, Thomas-Horton E, Schallom M. A Multidisciplinary QI Initiative to Improve OR-ICU Handovers. Am J Nurs. 2018;118(2):48–59. doi:10.1097/01.NAJ.0000530248.45711.60
- Johnson M, Sanchez P, Langdon R, et al. The impact of interruptions on medication errors in hospitals: an observational study of nurses. J Nurs Manag. 2017;25(7):498–507. doi:10.1111/jonm.12486


Trackbacks/Pingbacks