

In part one of a two-part series on vector-borne illnesses, we seek to take a deep dive into Lyme disease and Malaria. For more on the other vector-borne illnesses, check out part two!
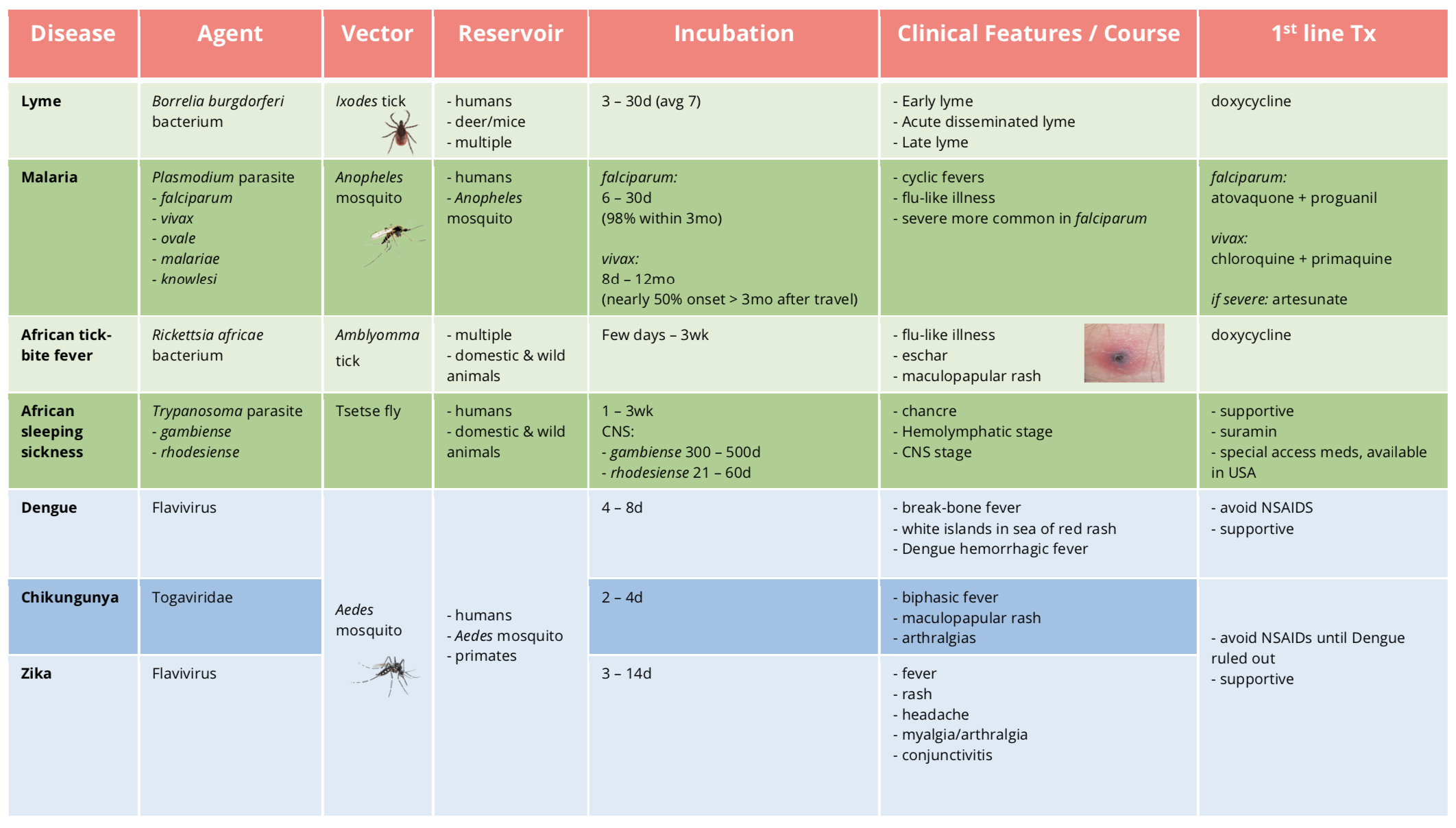
Table 1 | Summary of agent, vector, reservoir, incubation period, common symptoms, and first-line treatment for vector-borne illness causing fever and rash. d: day(s), wk: week(s), mo: month(s).
The only helpful way to distinguish between all these illnesses is the incubation period and distribution (Table 2).
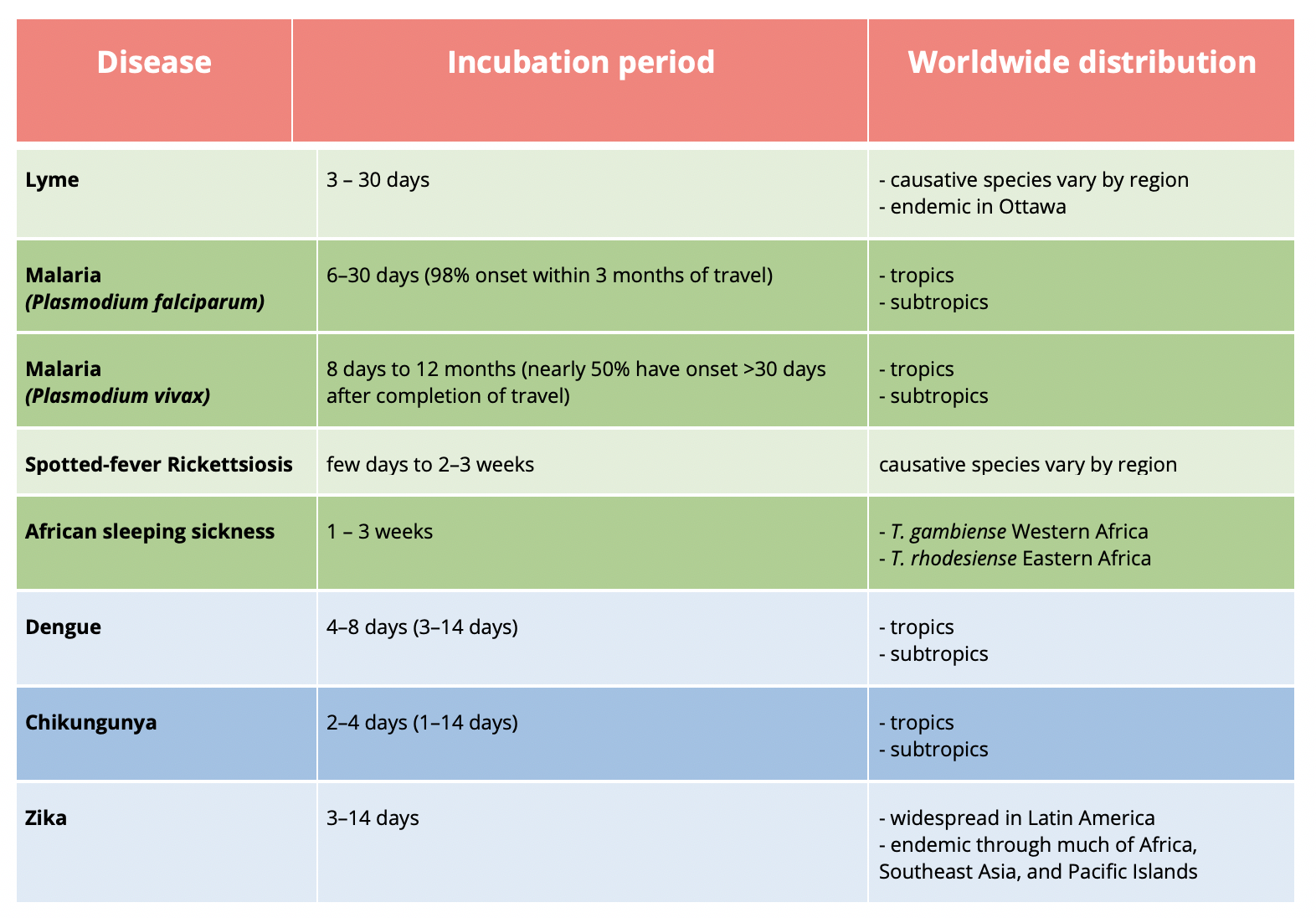
Table 2 | Summary of factors to differentiate between vector-borne illness including incubation period and worldwide distribution. Modified from Yellow Book [11].
Lyme Disease
For a deep dive into Lyme disease and the literature, check out this great post by Dr. Mike Ho.
- Vector
- Ixodes scapularis (most common), pacificus, ricinus, or persulcatus)
- Agent
- spirochete bacterium Borrelia burgdorferi
- Reservoirs
- multiple
- most common: deer and mice
- To learn more about the Lyme life cycle, click here.

Figure 1 | Size of nymph stages of the Ixodes tick at various hours of feeding on the left and the adult female at various stages of feeding on the right. Modified from Ogden et al (2017).
Risk of transmission of Lyme disease:
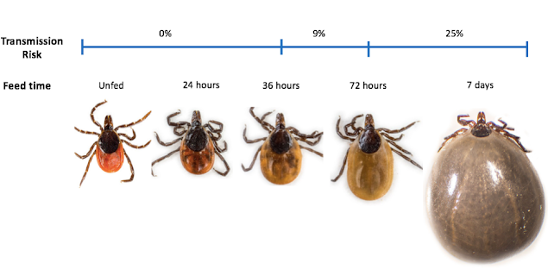
Figure 2 | Ixodes tick at various stages of feeding and risk of transmission. Obtained from https://emottawablog.com/2016/11/what-we-know-about-lyme-disease/.
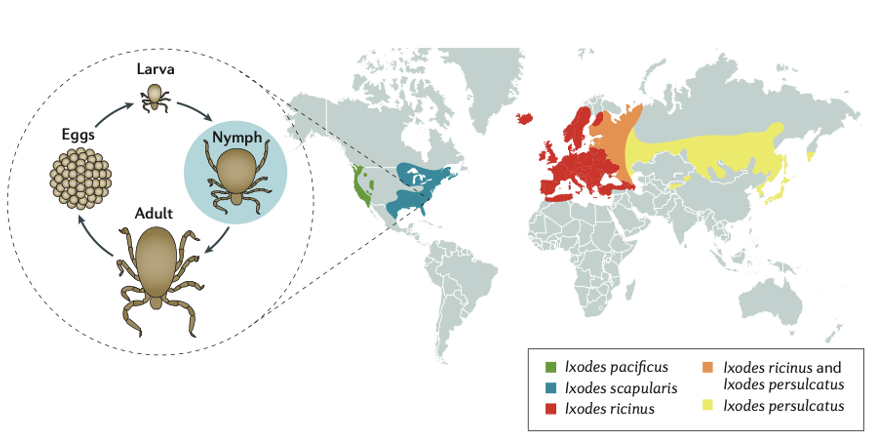
Figure 3 | Distribution of Ixodes species of tick. Obtained from Steere et al (2017).
The distribution of Ixodes tick depends on the species. On the east coast of North America, Ixodes scapularis is the most common. A recent study published online by the University of Ottawa in 2019 showed that “of the 194 adult and 26 nymphal black ticks tested, almost 30% were infected with B. burgdorferi…” This suggests that Ottawa is endemic for Lyme disease.
Lyme disease symptomology is separated into three stages; early (Table 3), acute disseminated, and late Lyme.
Erythema migrans is clasically heralded as the characteristic target rash, but is only present in 30% of Lyme disease cases. Other rashes including a uniform lesion, vesicular lesions, multiple annular lesions, and multiple patches are also possible. Note that when a rash is present, erythema migrans is the most common for all age groups, with the greatest prevalence at extremes of age and cardiac symptoms are most common in the 25 – 44 age group (Figure 7).
Early Lyme
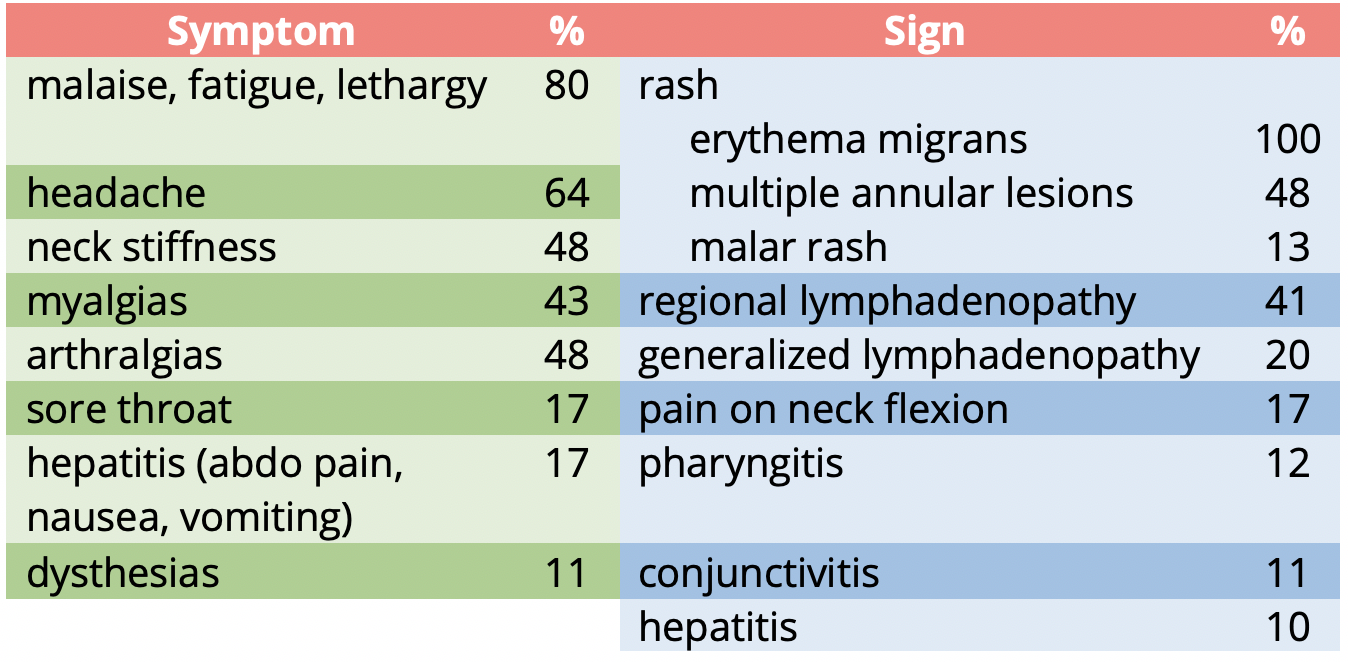
Table 3 | Signs and symptoms of Early Lyme Disease.
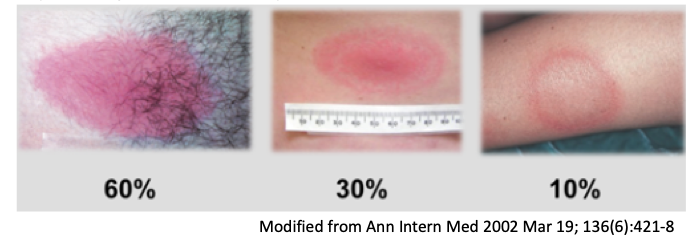
Figure 4 | Examples of erythema migrans rash in the first three days.
Acute Disseminated Lyme
Presentation:
- Neurologic
- Fluctuating meningoencephalitis
- Cranial neuropathy: Bells most common (bilateral Bells highly suggestive)
- Peripheral neuropathy
- Radiculopathy
- Cardiac
- AV block
- 49% 3°
- 16% 2°
- 12% 1°
- Myopericarditis
- Tachydysrhythmias
- Ventricular impairment
- AV block
- Arthritis
- Monoarticular arthritis
- Larger joints (knee)
- Less common shoulder, elbow, TMJ, ankle, wrist, hip, hands
- Arthrocentesis inflammatory arthritis
- Ophthalmic
- Conjunctivitis
- Keratitis
- Choroiditis
- Retinal detachment
- Optic neuritis
- Blindness
Late Lyme
- Arthritic
- Chronic arthritis 10%
- Neurologic
- Chronic encephalopathy
- Moderately severe memory and learning impairment
- Mild psychiatric symptoms: depression, irritability, paranoia
- Peripheral:
- Sensory polyradiculopathy
- Demyelinating lesions resembling multiple sclerosis
- Skin
- Acrodermatitis chronica atrophicans
- Chronic encephalopathy
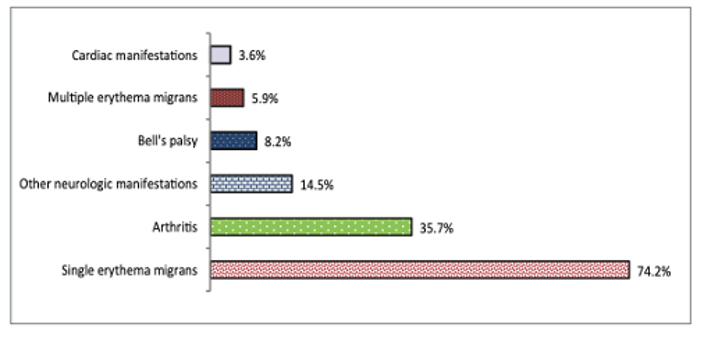
Figure 5 | Percentage of clinical manifestations for Lyme disease infections acquired in Canada, 2009 – 2015. From Gasmi et al (2017).
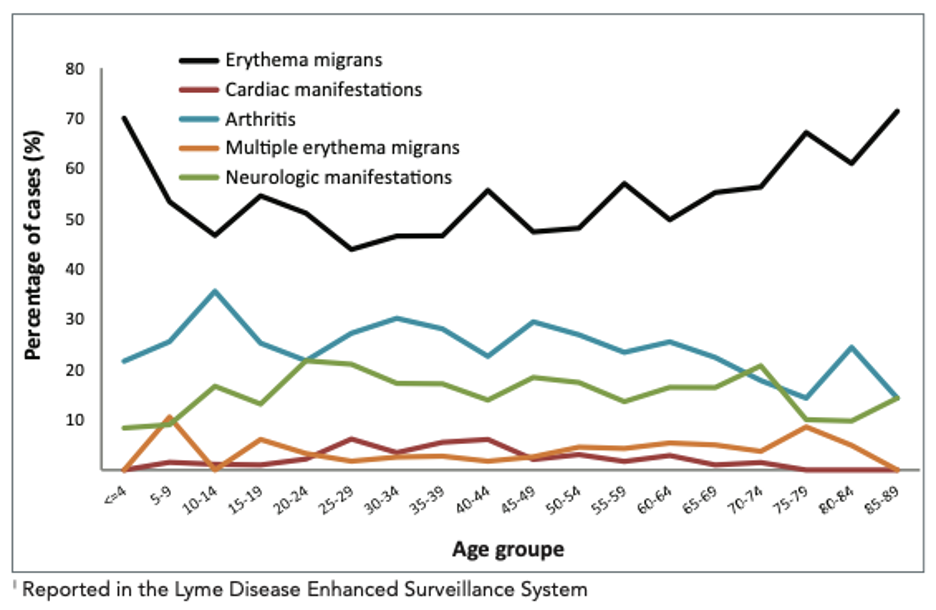
Figure 6 | Percentage of clinical manifestations for Lyme disease infections acquired in Canada by age group, 2009 – 2015. From Gasmi et al (2017).
Treatment
For guidelines on who to test, prophylaxis, and treatment in the Ottawa area, click here.
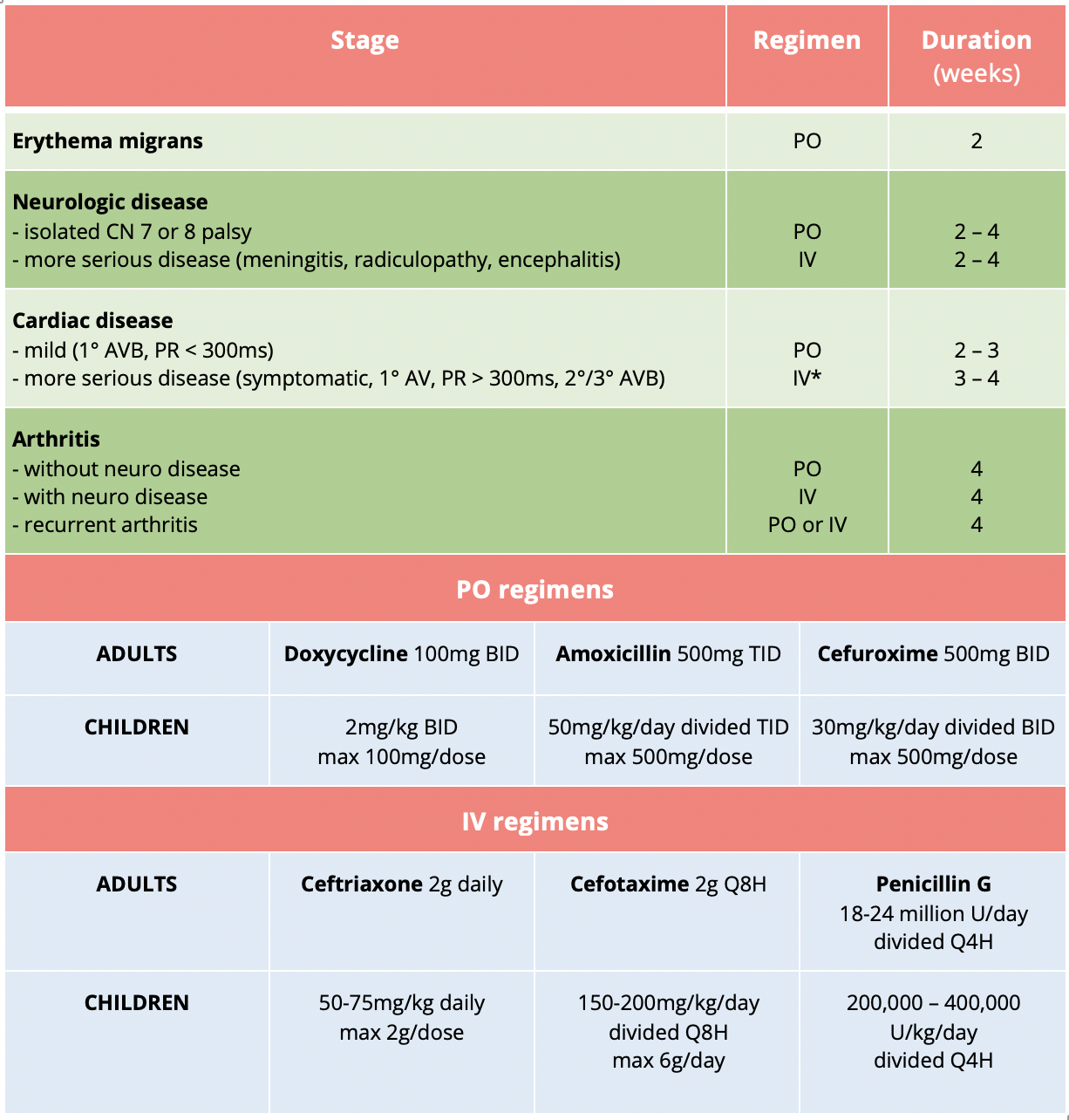
Table 4 | Treatment regimens for Lyme disease. Obtained from https://emottawablog.com/2016/11/what-we-know-about-lyme-disease/.
*IV antibiotics should be continue until high-grade AVB has resolved and PR < 300ms. The patient can then be switched to PO to complete the course.
Malaria
- Vector
- Female Anopheles mosquito
- Agent
- Plasmodium falciparum
- Africa: 99.7% falciparum
- Plasmodium vivax
- South-East Asia: 53% vivax
- Americas: 75% vivax
- Plasmodium ovale
- Plasmodium malariae
- Plasmodium knowlesi
- Plasmodium falciparum
- Reservoirs
- Humans
- Mosquitoes
- Transmission
- Bite of infected Anopheles mosquito
- Blood transfusion
- Organ transplantation
- Needle sharing
- Vertical transmission in pregnancy
- To learn more about malaria’s life cycle, click here.
The World Malaria Report was released in 2019; with the worldwide incidence in 2018 being 228 million cases, 405,000 deaths (67% were children < 5 years), 11 million pregnancies were exposed leading to 872,000 low-birthweight children, and 24 million children were infected with Plasmodium falciparum alone.
The top countries for total malaria cases were Nigeria (25%), the Democratic Republic of the Congo (12%), and Uganda (5%). For vivax, 47% of cases were in India, 11% in Afghanistan, and 8% in Pakistan. From a mortality perspective; 24% occurred in Nigeria, 11% in the Democratic Republic of the Congo, and 5% in the United Republic of Tanzania. The full report can be found here.
Malaria typically causes fever and flu-like illness. Table 5 outlines the defining features of severe malaria, which is most often caused by P. falciparum.
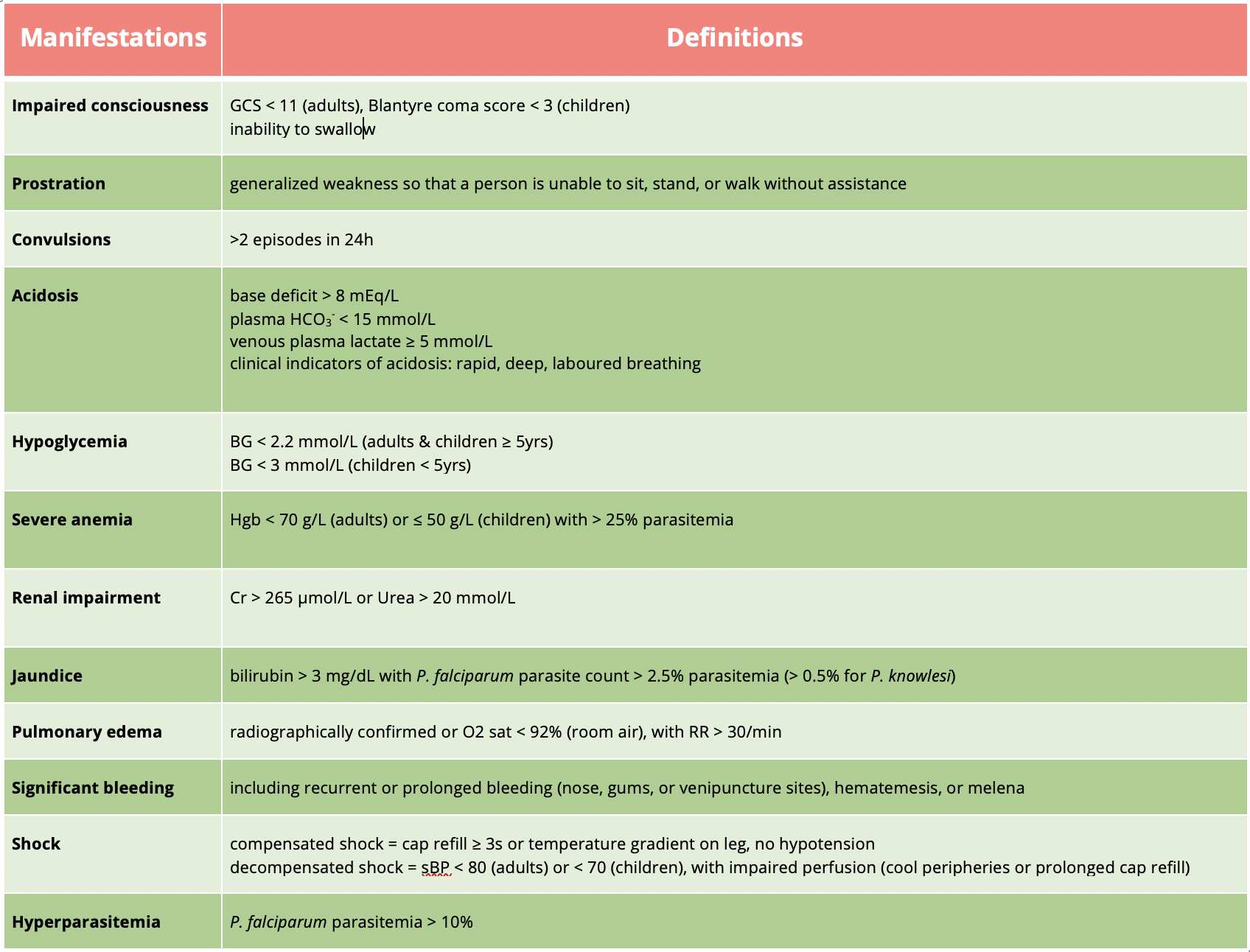
Table 5 | Severe malaria is defined as one or more of the above occurring in the absence of an identified alternative cause and in the presence of P. falciparum or P. knowlesi parasitemia. Adapted from UpToDate.
Treatment regimens are region-dependent and local guidelines for resistance patterns should be followed. At The Ottawa Hospital, treatment guidelines can be found in the Malaria Binder in the Emergency Department and are outlined below. If at any time, any oral antimalarial medication is vomited within 60min of administration, repeat the full dose. If vomiting recurs, call the physician to change to parenteral therapy.
For non-severe P. falciparum:
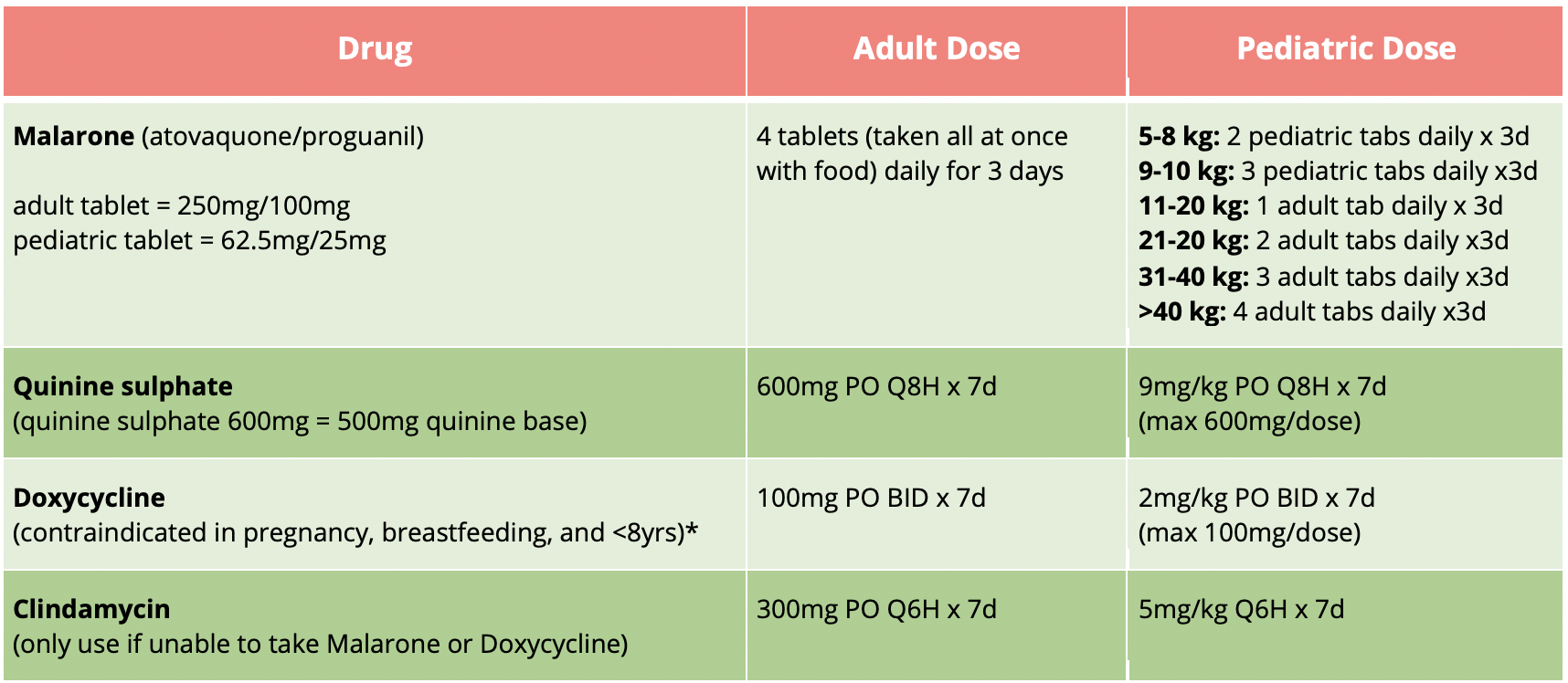
Table 6 | Oral antimalarial regimens for non-severe P. falciparum. *while doxycycline is contraindicated during pregnancy, it may be used during breastfeeding and in children <8yrs of age for the treatment of malaria if other options (i.e., Malarone and clindamycin) are not possible.
For severe P. falciparum:
Artesunate 2.4mg/kg IV STAT, then Q12H x 2 doses, then Q24H x 1 dose.
For non-falciparum:
- chloroquine phosphate 1000mg PO STAT, then 500mg 6h later, then 500mg daily x 2d.
- if patient cannot tolerate chloroquine, then:
- Malarone (atovaquone/proguanil) 4 tabs PO daily x 3d (administer with fatty food).
- in addition to chloroquine or Malarone, start primaquine 30mg PO daily x 14d if:
- G6PD level is document as normal
- patient is not pregnant/breastfeeding
Take home points:
Lyme
- Know the criteria for lyme diagnosis, prophylaxis, and treatment
- Lyme disease rashes may not always present as a classic target lesion
- Treat erythema migrans in endemic regions as Lyme disease without further testing
- Consider Lyme in a viral syndrome in non-winter months:
- Carditis
- Neuritis (facial nerve palsy, subacute meningitis)
- Arthritis
- Chronic Lyme disease is controversial and common in the media
Malaria
- Pitfalls:
- Not seriously considering the diagnosis
- Not recognizing fever in returning traveler as a MEDICAL EMERGENCY
- Not recognizing Malaria as a MEDICAL EMERGENCY
- Not appreciating how quickly a patient can become gravely ill
- Remember:
- Our role is to test and initiate treatment if positive
- If in doubt – treat as falciparum
- If in doubt – treat as resistant
- If someone has Malaria speak with ID
- If someone has falciparum DON’T SEND THEM HOME
1. Ho, Michael. What we know about Lyme Disease [online]. Available from https://emottawablog.com/2016/11/what-we-know-about-lyme-disease/. Accessed August 13 – September 10, 2020.References
2. CDC. Lyme Disease. Available from https://www.cdc.gov/lyme/index.html. Accessed August 13 – September 10, 2020. 3. Minnesota Lyme Association [online]. Available from https://mnlyme.org/about-lyme-disease/overview/ Accessed August 14, 2020.
4. Ogden, N. H., Lindsay, L. R., Morshed, M., Sockett, P. N., & Artsob, H. (2009). The emergence of Lyme disease in Canada. CMAJ, 180(12), 1221–1224.
5. Steere, A. C., Strle, F., Wormser, G. P., Hu, L. T., Branda, J. A., Hovius, J. W. R., et al. (2016). Lyme borreliosis. Nat Rev Dis Prim, 2(1), 586–19.
6. Tiny Predators in the Park: 1 out of 3 ticks tested in new Ottawa study carry Lyme Disease. (2020) [online]. Available from https://med.uottawa.ca/en/news/tiny-predators-park-1-out-3-ticks-tested-new-ottawa-study-carry-lyme-disease. Accessed August 24, 2020.
7. Walls et al. (2018) Rosen’s Emergency Medicine. (9th Edition) Philidelphia PA/USA: Elselvier
8. UpToDate. Lyme Disease [online]. Available from https://www.uptodate.com/contents/clinical-manifestations-of-lyme-disease-in-adults?search=lyme%20disease&source=search_result&selectedTitle=1~150&usage_type=default&display_rank=1. Accessed August 25, 2020.
9. Gasmi, S., Ogden, N. H., Lindsay, L. R., Burns, S., Fleming, S., Badcock, J., et al. (2017). Surveillance for Lyme disease in Canada: 2009–2015. Canada Communicable Disease Report, 43(10), 194–199.
10. Public Health Ontario. Ottawa Algorithm for Lyme Disease (2019) [online]. Available from https://www.ottawapublichealth.ca/en/professionals-and-partners/resources/Documents/Ottawa-Algorithm-for-Lyme-Disease_July2019.pdf. Accessed August 25, 2020.
11. CDC. Malaria [online]. Available from https://www.cdc.gov/parasites/malaria/index.html. Accessed August 13 – September 10, 2020.
12. CDC. Yellow Book (2020) [online]. Available from https://wwwnc.cdc.gov/travel/page/yellowbook-home. Accessed August 13 – September 10, 2020.
13. CDC. Malaria Life Cycle [online]. Available from https://www.cdc.gov/malaria/about/biology/index.html. Accessed August 20, 2020.
14. World Health Organization. World Malaria Report (2019) [online]. Available from https://www.mmv.org/newsroom/publications/world-malaria-report-2019?gclid=CjwKCAjwkoz7BRBPEiwAeKw3q9KxibQ9Snc7Iwg07NTuuQR7udMvDEoLS-6N1rWpiv_qhQtygNfl3RoCiCMQAvD_BwE. Accessed August 20, 2020.
15. Infectious Diseases and Pharmacy, The Ottawa Hospital. Malaria Binder (2019).
16. CDC. African Tick Bite Fever. [online] Available from https://wwwnc.cdc.gov/travel/diseases/african-tick-bite-fever. Accessed August 13 – September 10, 2020.
17. Cazorla C, Socolovschi C, Jensenius M et al (2008). Tick-borne Diseases: Tick-borne Spotted Fever Rickettsioses in Africa. Infectious Disease Clinics of North America 22(3): 531 – 544.
18. Faccini-Martinez A, Garcia-Alvarez L, Hidalgo M et al (2014). Syndromic classification of rickettsioses: an approach for clinical practice International Journal of Infectious Diseases. 28: 126 – 139.
19. CDC. African Sleeping Sickness. [online] Available from https://wwwnc.cdc.gov/travel/diseases/african-sleeping-sickness-african-trypansosomiasis Accessed August 13 – September 10, 2020.
20. Lundkvist, G. B., Kristensson, K., & Bentivoglio, M. (2004). Why Trypanosomes Cause Sleeping Sickness. Physiology, 19(4), 198–206.
21. CDC. African Sleeping Sickness [online]. Available from https://www.cdc.gov/parasites/sleepingsickness/diagnosis.html. Accessed August 31, 2020.
22. CDC. African Sleeping Sickness [online]. Available from https://www.cdc.gov/parasites/sleepingsickness/health_professionals/index.html#tx Accessed August 13 – September 10, 2020.
23. CDC. Dengue [online]. Available from https://www.cdc.gov/dengue/. Accessed August 13 – September 10, 2020.
24. CDC. Dengue [online]. Available from https://www.cdc.gov/dengue/areaswithrisk/around-the-world.html. Accessed September 1, 2020.
25. CDC. Chikungunya [online]. Available from https://www.cdc.gov/chikungunya/Accessed August 13 – September 10, 2020.
26. Diop D, Meseznikov G, and Sanicas M (2015). Chikungunya outbreaks from 2000 – 2015: A Review. MOJ Public Health; 2(6): 43 – 49. 27. CDC. Zika [online]. Available from https://www.cdc.gov/zika/Accessed August 13 – September 10, 2020.
28. Traer, Julia. Zika Virus – What we know and what we don’t [online]. Available from https://emottawablog.com/2017/05/zika-virus-what-we-know-and-what-we-dont/. Accessed September 2, 2020.
29. CDC. Zika [online]. Available from https://wwwnc.cdc.gov/travel/files/zika-areas-of-risk.pdf. Accessed September 2, 2020.
30. CDC. When to test Zika [online]. Available from https://www.cdc.gov/zika/pdfs/when-to-test-zika.pdf. Accessed September 2, 2020.
31. CDC. Data and Statistics on Zika in Pregnancy [online]. Available from https://www.cdc.gov/pregnancy/zika/data/index.html. Accessed September 2, 2020.


Trackbacks/Pingbacks