

“The differences between expert performers and normal adults are not immutable, that is, due to genetically prescribed talent. Instead, these differences reflect a life-long period of deliberate effort to improve performance.”
– K. Anders Ericsson
What defines expertise, and how can we apply this to our field of emergency medicine?
When we look at other high-performance organizations such as professional sports, it becomes clear that these individuals have what is called the “performance mindset”. They do not simply show up to each practice expecting to be competent. Instead, they are obsessed with seeking feedback to improve their game. They practice deliberately. They use consistent, marginal gains to surpass their competition.
Rafael Nadal, one of the greatest tennis players alive, uses daily feedback from his coach to constantly improve his game. Why should doctors be any different? So here we seek to explore strategies of high performing organizations and how we can apply them to maximize our careers in emergency medicine.
Deliberate practice
The study of expertise was largely pioneered by Dr. Anders Ericsson, a Swedish cognitive psychologist. He studied experts in various domains from chess grandmasters, to Olympic athletes, and elite musicians. His research concluded that experts were almost always made, and not born.

The one common variable identified was how experts learn. He noticed that it wasn’t just the amount of hours that they practiced, but how deliberately they practiced. Nobody becomes an outstanding professional without experience, but extensive experience does not invariably lead people to become experts.1
How is deliberate practice different from regular practice?
- Emphasizes the quality of the practice, rather than the amount
- Requires immediate feedback from an experienced coach
- Takes place outside of the participant’s comfort zone
- Is purposeful and repetitive, not aimed at vague overall improvement
Let’s use golf as an example. Each time you go out with your friends, you remind yourself to try and work on your swing. However, you find it difficult to get feedback because you are constantly taking shots from different areas around the course. Deliberate practice would require you to take the same shot repeatedly from the same location on the course, modifying it each time using immediate and specific feedback from a coach or video capture device.
In medicine, deliberate practice can be applied broadly to mastering any skill. For example, laryngoscopy is inherently a difficult technique to master for a reason. There is often a period of many weeks between each opportunity, and any feedback that is received is often forgotten before the next attempt.
Applying the principles of deliberate practice, one approach would be to improve the quality of your feedback, for example, by using a video laryngoscope capable of recording the procedure. By keeping a video database of your intubations and having it reviewed by your group’s airway experts, you can keep a running list of tips and review this before each future intubation.
A second approach would be to practice laryngoscopy in rapid succession, applying immediate feedback between each attempt. This is not feasible in real life, therefore you would need to use either a simulated mannequin or cadaver lab. Having regular sessions of deliberate airway practice is a strategy to keep your performance from deteriorating over time.
Mental Practice
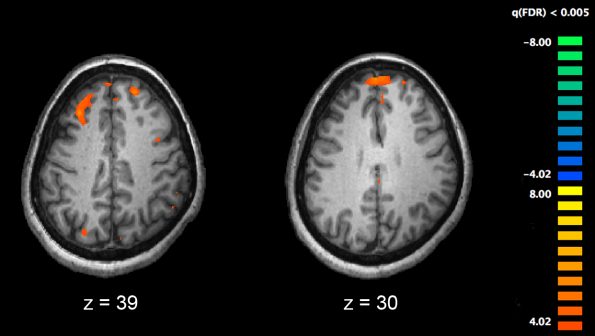
The next high-performance technique to explore is mental practice. This is defined as, “the cognitive rehearsal of a task in the absence of overt physical movement”. Mental practice has been used by elite athletes and musicians for decades and has been shown to be an efficient means of enhancing performance.2 Studies, primarily in rehabilitation literature, have shown that mental practice activates similar cortical pathways as physical motor activity.3
What does the evidence say about mental practice?
As you can imagine, there are few randomized controlled trials looking at this in medicine.
Looking at procedural ability, one RCT examined novice surgery residents performing virtual laparoscopic cholecystectomy.4 They randomized 20 participants to have either a 30 min mental practice session prior to the surgery, or 30 min of a traditional didactic lecture. The participants that took part in the mental practice session significantly outperformed their colleagues.
How does mental practice hold up non-technical skills, such as teamwork behavior? A paper in 2016 looked at mental practice as a tool to enhance team-based trauma resuscitation.5 Participants were randomized to either 20 min of mental practice or 20 min of traditional ATLS training prior to a simulated trauma scenario. The participants in the mental practice group outperformed the control group on teamwork behavior.
How does one effectively perform mental practice?6
- Review cognitive aid (e.g. video of the procedure)
- Reflect on previous experiences
- Guided by a script
- Add tfidelity (standing)
- Perform in real-time, in as much detail as possible
If it’s been a while and you don’t have fresh experiences to draw off of, consider first reviewing a cognitive aid, such as a video of the procedure you want to learn. You should then reflect on your prior experiences. What do you remember went well? What did you find needed improvement? You should then consider using a procedure script, many of which can be found online or in textbooks such as Roberts and Hedges. You can add fidelity, such as standing, if that’s how you usually perform the procedure. Finally, you should perform it in real-time, recreating in your mind as much detail as possible.
“PETTLEP”
| P – Physical | Imagine all relevant physical characteristics |
| E – Environment | Imagine the environment in which the performance will occur |
| T – Task | Accurately reproduce all task steps |
| T – Timing | As much as possible, visualize steps in real time |
| L – Learning | Update visualization based on learning, experience, and changing task demands |
| E – Emotion | Conjure emotions that are likely to be experienced during the act itself; avoid debilitative emotions such as fear, panic |
| P – Perspective | Visualize from an internal, or first-person, perspective |
Rapid cycle deliberate practice
The next high-performance technique we’re going to discuss is rapid cycle deliberate practice. In this model, learners have multiple opportunities to try, learn, and immediately implement new skills in order to master a technique.
RCDP works best for metric based targets that you are looking to improve, such as:
- Time to defibrillation
- Minimizing peri-shock pauses
- Mastering the initial steps of neonatal resuscitation
Let me give you an example.
Say for instance you feel like your neonatal resuscitation (NRP) skills need a refresher. Let’s be honest – who doesn’t think this? With traditional simulation, you may find it a bit overwhelming if you get thrown into a complex neonatal resuscitation, when really what you are after is to improve your basic NRP fundamentals.
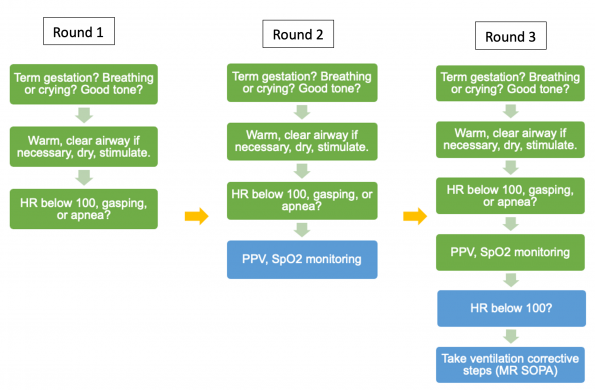
With RCDP, you bring the simulation facilitator into the room to provide continuous feedback. You start off easy, but with each successive round, you add layers of difficulty.
For example, your first run through starts off pretty good, you remember to warm, dry, and stimulate. However, when you notice the HR is below 100, you immediately start CPR instead of positive pressure ventilation. At this point, you stop, address this, and repeat the SIM starting from the beginning. Each round you add increasing difficulty until you achieve mastery of the skill.
Audit & Feedback
Audit and feedback is a widely used strategy for assessing and improving physician performance. It involves the measurement of performance on several metrics and feeds those results back to physicians for comparison against peers, prior performance, or other benchmarks.
A 2012 Cochrane review included 82 studies that looked at the clinical benefits of an audit and feedback program.8 They found that such a program leads to a median of 4.3% improvement in physician performance, with a moderate grade of evidence.
| Highest Ranked | Lowest Ranked |
| 72 hour ED return and ICU/OR admission rate | CT head utilization rate in minor head trauma |
| 72 hour ED return and admit rate | Time from PIA to patient left department |
| Emergency MD evaluation of quality of care I provide | % Consultations admitted > 24 hours |
| % of patients with an understanding of the plan for self-care and further medical care | CT head with chief complaint of headache |
|
Management of sepsis |
PE testing rate |
The review found that audit and feedback was most effective if:
- The physician is not performing well to start out with
- The person responsible is a supervisor or colleague
- It is given verbally and in writing
- It is provided more than once
- It includes clear targets and an action plan.
A 2020 survey of 104 emergency doctors across Canada found that overall, physicians are interested in audit and feedback activities. The survey asked these physicians to rank 49 performance metrics in order from most to least useful. Here you can see the top and bottom 5 metrics.9
The respondents also had strong views regarding who should have access to their practice data. They ranked the ED chief and ED quality committee in high preference, and interestingly the scheduler and hospital quality committee as low preference to have this data.
A strong audit and feedback program is not just the delivery of a “physician score-card”, but includes multiple feedback steps. Areas for improvement should result in non-punitive action plan, and metrics should be reassessed regularly to assess for improvement.10
Conclusions
In this post, we explored the science of what makes a high performer, and how you can use a few strategies to improve your game in emergency medicine. By practicing deliberately, seeking continuous feedback and using audit data to guide your learning, your growth curve should continue to accelerate and your patients will reap the benefits.
References:
- Ericsson, K., Krampe, R., Tesch-Römer, C. (1993). The Role of Deliberate Practice in the Acquisition of Expert Performance. Psychological Review 100(3), 363-406.
- Driskell, J., Copper, C., Moran, A. (1994). Does mental practice enhance performance? Journal of Applied Psychology 79(4), 481-492.
- Szameitat, A., Shen, S., Sterr, A. (2007). Motor imagery of complex everyday movements. An fMRI study. NeuroImage 34(2), 702-713.
- Arora, S., Aggarwal, R., Sirimanna, P., Moran, A., Grantcharov, T., Kneebone, R., Sevdalis, N., Darzi, A. (2011). Mental Practice Enhances Surgical Technical Skills. Annals of Surgery 253(2), 265-270.
- Lorello, G., Hicks, C., Ahmed, S., Unger, Z., Chandra, D., Hayter, M. (2016). Mental practice: a simple tool to enhance team-based trauma resuscitation. CJEM 18(2), 136-142
- Riggs, J., McGowan, M., Petrosoniak, A., Hicks, C. (2020). Mental practice as a novel learning strategy for donning and doffing personal protective equipment during the COVID-19 pandemic. CJEM.
- Hicks, C., Petrosoniak, A. (2018). The Human Factor Optimizing Trauma Team Performance in Dynamic Clinical Environments. Emergency Medicine Clinics of North America 36(1), 1-17.
- Ivers, N., Jamtvedt, G., Flottorp, S., Young, J., Odgaard‐Jensen, J., French, S., O’Brien, M., Johansen, M., Grimshaw, J., Oxman, A. (2012). Audit and feedback: effects on professional practice and healthcare outcomes. Cochrane Database of Systematic Reviews 6(6), CD000259.
- Gupta, R., Mercuri, M., McCulloch, A., Monteiro, S., Mastoras, G., Krywenky, A., Chan, T., Mondoux, S. (2020). Regional needs assessment for emergency physician audit and feedback. CJEM 22(4), 542-548.
- Dowling, S., Mondoux, S., Bond, C., Cheng, A., Kwok, E., Lang, E. (2020). Audit and feedback for individual practitioners in the emergency department: an evidence-based and practical approach. CJEM 22(4), 528-533.

