
Case Presentation
A 30-year-old male presents to urgent care with a complaint of excruciating pain in his left hand. He is a gardener, and earlier that day had been mixing a solution of pesticides. He had been wearing gardening gloves to open the solutions, including a bottle of 20% hydrofluoric acid (HF). He noticed erythema starting to develop at the tips of his fingers several hours after preparing the pesticide, with increasing pain. At the time of his presentation, his hand looked like the picture below:

Throwing Caution To the Wind: Why Should We Care about Hydrofluoric Acid?
Hydrofluoric (HF) acid is a dangerous and highly corrosive inorganic acid, that has the ability to cause significant tissue damage.
HF acid is a common ingredient found in cleaning agents, rust removers, fertilizers, and pesticides.1 At high concentrations (>50%), the hydrogen and fluoride ions cause immediate tissue destruction and liquefactive necrosis, characterized by a white necrotic burn. Exposure of 2.5% of total body surface area to 100% HF has previously caused fatalities.2 Any substance capable of inflicting death after submerging a hand in a solution is worth talking about! Especially, since dilute HF acid concentrations (10-40%) are commonly found in household variants, and exposure to it can cause delayed pain and tissue destruction and profound progressive morbidity and mortality implications secondary to their systemic effects.3
HF acid penetrates quickly through the skin, where highly reactive fluoride ions form complexes with free calcium and magnesium. Cation scavenging results in hypocalcemia and hypomagnesemia, in addition to hyperkalemia secondary to potassium channel inhibition. These electrolyte abnormalities predispose patients to dysrhythmias, including ventricular fibrillation, which can result in death.4 Prior to death, the hallmark sign of HF acid burns is Pain Out of Proportion to the injury, as potassium ions leach from peripheral nerve endings.5
Suspecting Hydrofluoric Acid Injury: What next?
Work-up
As with any exposure, your assessment should begin with a complete history and physical exam. Through discussion, it is important to elicit specific details about the chemical used including concentration, time of exposure, route of exposure (cutaneous, ocular, ingestion, or inhalation), the surface area exposed, and treatments if any, that have already been initiated (i.e. decontamination).
Investigations that should be obtained include:
-
- Serum electrolytes: including ionized calcium, magnesium, and potassium. These should be monitored regularly, given the above pathophysiology.
- Venous Blood Gas (VBG): To detect metabolic acidosis.
- Electrocardiogram: To assess for prolonged QT or arrhythmias. Note – if HIGH-RISK patients*, they should be placed on cardiac monitoring.6
High-Risk*: An individual can be considered high-risk for systemic toxicity if they meet any of the following characteristics7:
-
- Any burns involving HF solution >50% concentration;
- Cutaneous involvement >5% of total body surface area regardless of HF concentration;
- Ingestion or Inhalation of HF.
If you have a high degree of suspicion or are worried about HF burns, consider calling poison control to consult a toxicologist.
Treatment
Dermal Burns
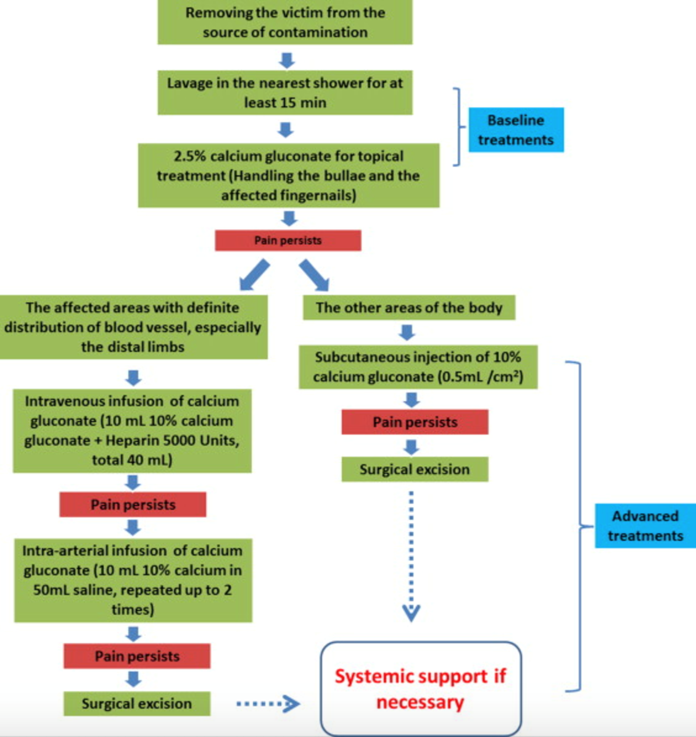
Treatment of dermal burns begins with thorough DECONTAMINATION.8 Decontaminate the patient by removing contaminated clothing and irrigating their body with copious amounts of water for a minimum of 30 minutes. If blisters are present, they will need to be de-roofed and irrigated. Nail beds may need to be exposed during irrigation, as they may harbor fluoride ions. Do not hesitate to perform a local digital block and remove the nail as HF readily infiltrates the nail plate and causes severe pain and tissue damage.9
After irrigation, the next step is NEUTRALIZATION of fluoride ions using 2.5% topical calcium gluconate gel.10 Neutralize fluoride ions by mixing 3.5g of calcium gluconate in 150 mL of water-based lubricant; apply generously to the affected area. Put a glove over the exposed dermal area, if it’s the hand that is affected or celophane wrap the region to keep the gel in place and prevent calcium loss. A reliable indicator of treatment effectiveness is pain relief.11 If topical calcium is not effective at reducing the pain within 30 minutes, calcium gluconate can be administered by local subcutaneous infiltration with 5-10% calcium gluconate to penetrate deeper tissues.10 When considering infiltration to finger pads, a prophylactic fasciotomy should be performed to prevent compartment syndrome.12 If after local infiltration, the patient’s pain is still not controlled, large quantities of calcium can be delivered directly to the tissue using an intra-arterial infusion of 10% calcium gluconate over 4 hours.10 Care and disposition should be coordinated with your local poison control center and plastic surgeons
While treating cutaneous injuries remember to monitor serum magnesium and calcium, and replace electrolytes accordingly.
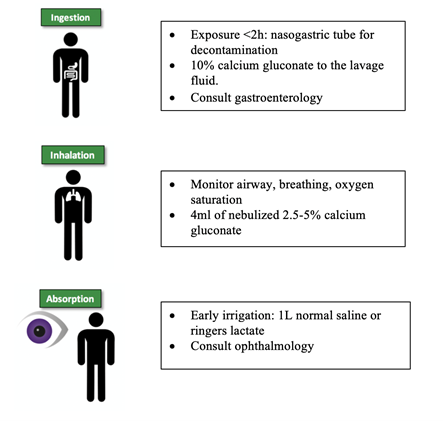
Ingestion/Inhalation/Absorption Injuries
Please consult your local Poison Control Centre for recommendations, and consult references 14 and 15.
Case Outcomes
The dilute pesticide used by this patient did not illicit pain until several hours after exposure. Toxicology was contacted and he was deemed to be a low-risk patient given that his burns covered <5% of total body surface area. After thorough irrigation, first and second digit nails were removed to allow for topical calcium penetration. Topical calcium was insufficient for pain control, as such local infusion of finger pads was completed following prophylactic fasciotomy. Plastic surgery was consulted, and the patient was expected to make a full recovery.
Clinical Pearls: Recognizing and Treating Hydrofluoric Acid
-
- HF Dermatological Burns can present hours after exposure.
- HF systemic toxicity is not to be underestimated. Arrhythmias, including VF, are of concern and can lead to death.
- Monitor Electrolytes (Calcium, magnesium, potassium), VBG, and ECG to monitor for systemic toxicity.
- Consult Toxicology
- Treatment is CALCIUM GLUCONATE to neutralize fluoride ion and prevent further tissue destruction.
References



