
Cerebral venous thrombosis (CVT) is a thrombotic disease of the cerebral veins and major dural sinuses. It is a rare kind of venous thromboembolism and can also be thought of as a type of stroke.
- CVT accounts for 0.5-1% of stroke cases.
- The annual incidence is 0.2 – 1.6 per 100,000 people.
- The median age of patients is 37 years and the female to male ratio is 3 to 1.
- Mortality is 5%.
- Significant morbidity is associated with delays in recognition.
- 85-90% of patients recover within 3-6 months after diagnosis but, up to 60% still continue to have problems with headache, fatigue, and cognitive issues (1, 2).
- At least 25% are unable to return to work.
Recently, thromboembolic events, including CVT, have been increasingly reported in COVID-19 patients (3, 4). They tended to have thrombosis of deeper veins and sinuses and many had fatal outcomes. With rising numbers of COVID-19 infections, it’s important to keep CVT on our differential as we see more cases come into the emergency department.
Risk Factors
- 85% of patients have at least 1 risk factor for the disease (5).
-
- Prothrombotic conditions
- Pregnancy & the post-partum period
- Oral contraceptive use
- Risk ↑ 6X & 30X if with obesity
- Antiphospholipid syndrome
- Inherited thrombophilia
- Malignancy
- Infections
- Ear, sinus, mouth, face and neck
- Inflammatory conditions
- e.g. vasculitis, IBD, SLE, sarcoidosis
- Trauma
- Head & neck injuries
- Venous catheterization
- Neurosurgical procedures
- Prothrombotic conditions
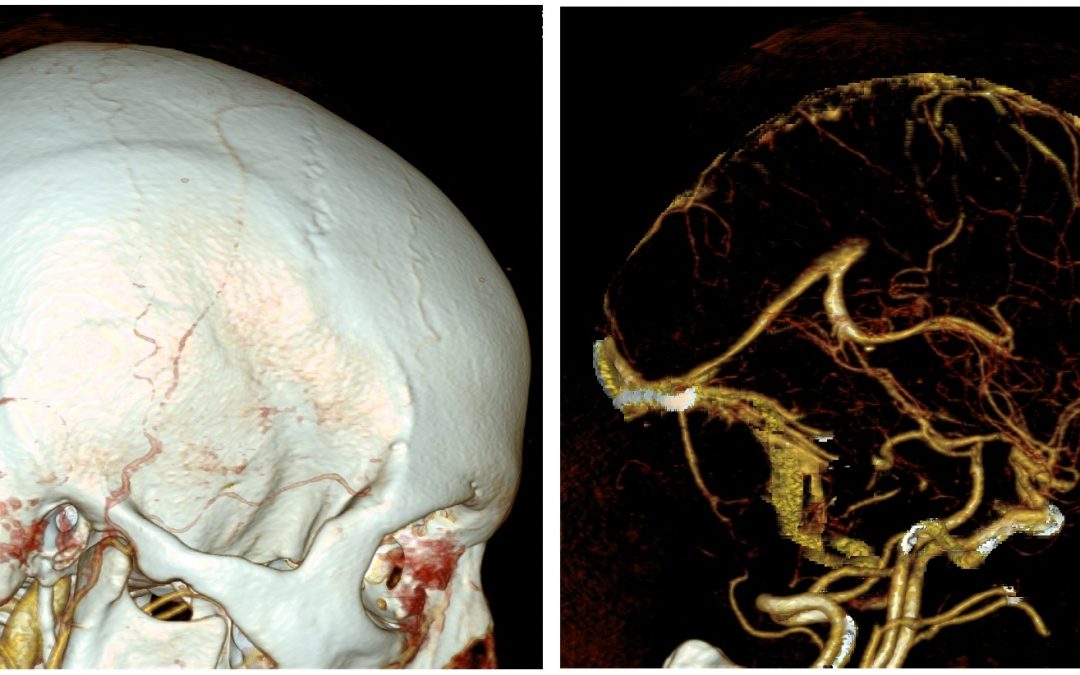
Anatomy
Cerebral veins are valveless and do not follow the same territory divisions as that of arteries. Blood will flow in any direction depending on the dominant pressure gradient.
The brain has cortical veins that drain into a system of venous channels called the dural sinuses (6, 7).
- Superficial cortical veins drain into the superficial sinuses, which include:
- Superior sagittal sinus
- Inferior sagittal sinus
- Sigmoid sinus
- Transverse sinus
- Cavernous sinus
- Deep cortical veins join to form the great cerebral vein (vein of Galen), which drains into the straight sinus.
- Both superficial and deep sinuses drain into the internal jugular vein, which goes back to the heart.
Venous sinuses also absorb cerebrospinal fluid (CSF). There are arachnoid granulations that project into the superior sagittal sinus and drain CSF into venous blood (6, 7).
Unlike other sinuses, the cavernous sinus lies in a plexus of veins, arteries and nerves (6). Cranial nerves (CN) 3, 4, 6 plus V1 and V2 branches of CN 5 traverse through this sinus. Thus, palsies of these specific nerves can occur with cavernous sinus thrombosis.

(Adapted from Thorell et al, 2015)
Path0physiology of Cerebral Venous Thrombosis
There are 2 proposed mechanisms, both result in increased intracranial pressure (ICP) (8, 9).
- Obstruction of the cerebral drainage system
- Causes increased venular and capillary pressures, which leads to decreased cerebral perfusion, disruption of the blood brain barrier and rupture of vessels
- Decreased CSF absorption
- Results in formation of a communicating hydrocephalus and increased ICP
In either case, cytotoxic edema, vasogenic edema and parenchymal hemorrhage ensue.

(Adapted from UpToDate, 2020)
Clinical Presentation
Patients with cerebral venous thrombosis can present in the acute, subacute or chronic phase (10).
- Acute ≤ 48h
- Subacute 48h – 30 days
- Chronic > 30 days
Symptomatology may reflect:
- Thrombus location
- ≥ 1 of 4 CVT syndromes

Cerebral Venous Thrombosis Syndromes
- Intracranial hypertension
- 90% have a localized and persistent headache
- Headache onset can be progressive or thunderclap in nature
- May show signs of increased ICP. For example, worse headache with bending over, coughing or performing a valsalva maneuver.
- Neurologic deficits
- Present in 37-44% of patients
- Motor findings are more common than sensory deficits
- Monoparesis, hemiparesis or bilateral weakness
- Seizure
- Seen in 30-40% of patients
- Either focal or generalized onset
- Encephalopathy
- Often in severe cases with significant hemorrhagic transformation and cerebral edema
- Usually from thrombosis of the straight sinus or in late presentations
- Large venous infarcts can also cause herniation and encephalopathy
Clinical presentation – Take home points:
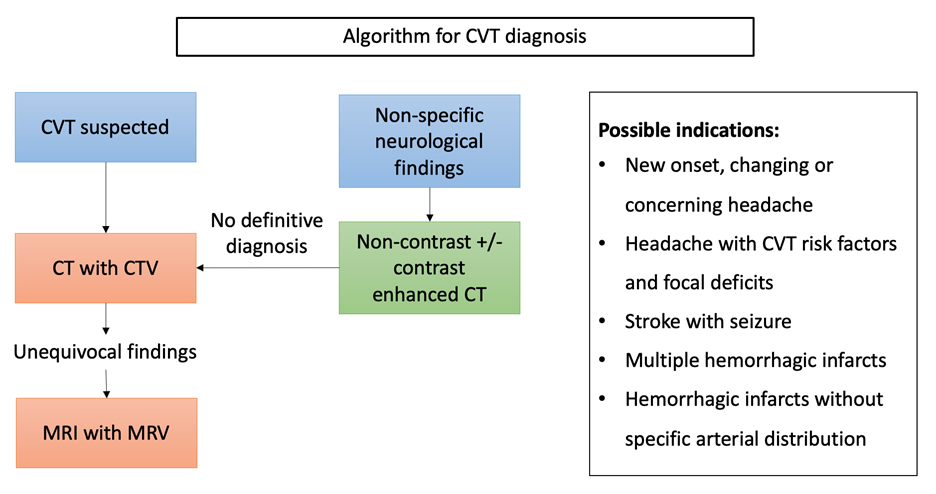
The following are triggers that would prompt further investigations for CVT.
- New onset, changing or concerning headache
- Headache with CVT risk factors and focal deficits
- Stroke with seizure
- Multiple hemorrhagic infarcts
- Hemorrhagic infarcts without specific arterial distribution
Diagnosis
The gold standard for diagnosis of cerebral venous thrombosis is MR venography (11, 12).
1. Laboratory investigations
D-dimer
- Raises the clinical suspicion of CVT but is not a good rule-out test because patients can have normal d-dimers, especially if they present later in the course of their disease
- Dentali et al, 2012 (13)
- A meta-analysis of 14 studies which included 1134 patients
- D-dimer had a sensitivity of 93.9% and a specificity of 89.7%
- Found specific risk factors for false negative D-dimer results:
- An isolated headache
- Delayed presentation past the acute phase
- Involvement of only a limited # of venous sinuses.
- Meng et al, 2014 (14)
- 233 patients with suspected CVT
- Prospectively looked at the diagnostic accuracy of D-dimer in the acute phase
- Showed D-dimer had a higher sensitivity and specificity at 94 and 98%, respectively
Lumbar puncture (LP)
- Only useful for ruling out other causes of headache such as meningitis because CSF is abnormal in 30-50% of CVT cases
- Can mimic other conditions like viral meningitis (15)
- ↑ white count
- ↑ red blood cell count
- ↑ proteins
- > 80% have ↑ opening pressure, which can also be observed in other conditions such as idiopathic intracranial hypertension
2. Neuroimaging
Non-contrast CT (NCCT)
- Detects both direct and indirect signs of CVT
- Direct signs are present in only 1/3 of cases
- Cord sign – curvilinear or linear hyperattenuation within a dural sinus along the tentorium
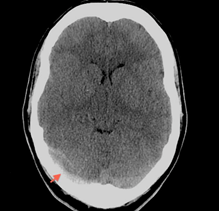
(Adapted from radiopaedia.org)
-
- Dense vein sign (dense triangle sign) – hyperattenuation with a triangular or round shape representing a clot
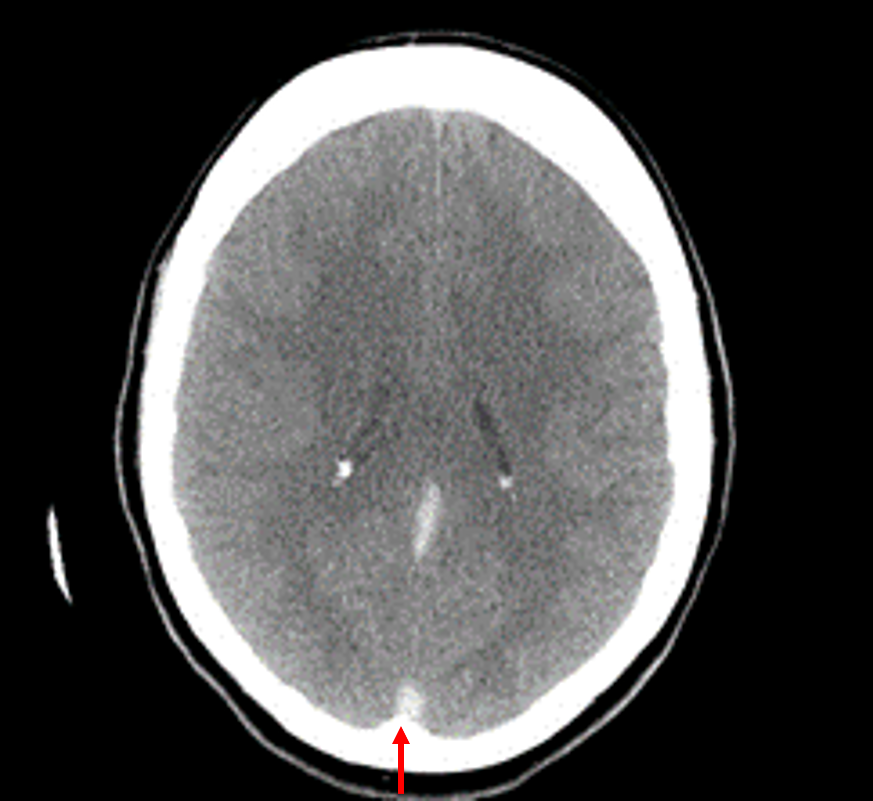
(Adapted from radiopaedia.org)
- Indirect signs:
- Significant contrast enhancement over the falx and tentorium
- Dilated venous structures
- Small ventricles
- Parenchymal abnormalities – such as hemorrhagic infarcts or cerebral edema
- Multiple infarctions or infarctions in several arterial distributions
- Bilateral lesions and edema
Contrast-enhanced CT (CECT)
- The thrombus appears as a filling defect
- Empty delta sign – triangular pattern of contrast enhancement surrounding a central area of hypodensity
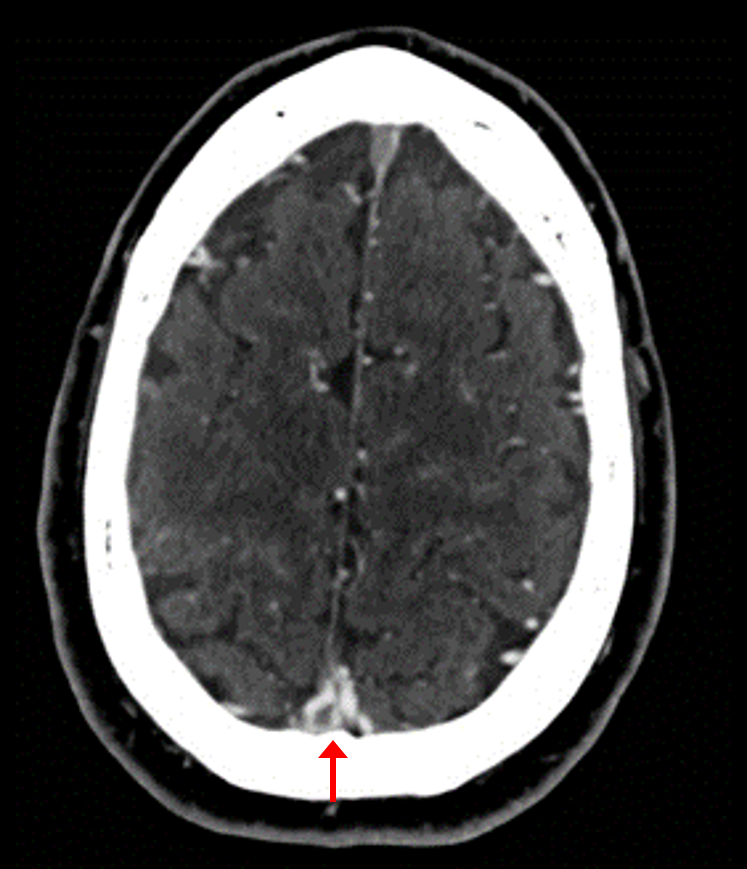
(Adapted from radiopaedia.org)
Diagnostic accuracy of NCCT and CECT
- Both miss up to approximately 20-30% of CVT
- Xu et al, 2018 (16)
- A meta-analysis consisting of 48 studies, more than 4500 cases
- Compared diagnostic accuracy of CT vs MRI at diagnosing CVT
- NCCT + CECT have a pooled sensitivity and specificity of 79% and 90%, respectively
- Xu et al, 2018 (16)
CT venogram
- Capable of detecting the heterogenous density of the thrombus, filling defects, sinus wall enhancement and increased collateral venous drainage
- When compared against digital subtraction angiography (DSA), this test has a sensitivity of 95% and a specificity of 91%.
- Combining a NCCT with CT venography, the accuracy of detecting a CVT is 90-100%, depending on the site of occlusion (11).
- CT venography is not as good for looking at thrombosis of cortical veins. Reported sensitivity varies significantly from 6-75% (17).
MRI + MR venogram
- When compared with CT, MRI without contrast has a pooled sensitivity of just 82% and a specificity of 92% (16).
- Contrast enhancement in a MR venogram provides better visualization of cerebral veins and abnormal flow.
- Comparing MR venogram against DSA, MR venogram has a sensitivity and specificity of 100 and 93%, respectively (12).
CT vs MR venogram
- Guidelines suggest that CT venography is at least equivalent to MR venography for diagnosing CVT (11, 12). However, the evidence is not considered high quality since the studies were observational and small, and thus were at high risk of bias.
- CT venography:
- Quicker to obtain
- Has less motion artifacts
- Can be used in patients with contraindications for MRI (e.g. implanted magnetic devices or pacemaker)
- MR venography:
- Higher resolution
- Better for deep venous structures and cortical veins
- No radiation exposure
Angiography
- Not required for diagnosis of cerebral venous thrombosis (12)
- Only recommended when clinical suspicion for CVT is high yet CT or MR venography are inconclusive, or if endovascular procedures are planned
Diagnosis – Take home points:
- D-dimer and LP are not recommended
- CT venography is at least as accurate as MR venography
- Angiography only considered if CT and MR are inconclusive and clinical suspicion remains high
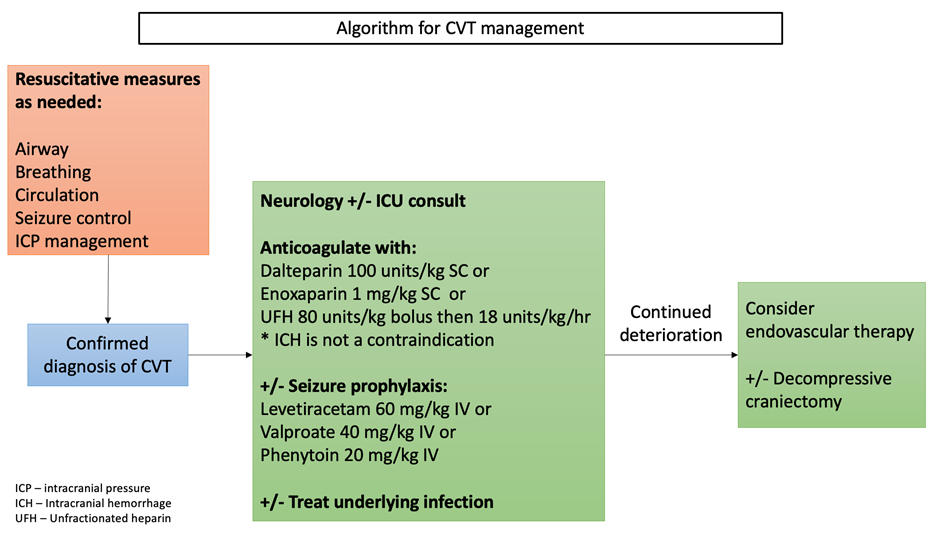
Management of Cerebral venous thrombosis
Management priorities are in resuscitating and stabilizing the patient along with treatment of life-threatening complications including respiratory failure, increased ICP and seizure. This is followed by antithrombotic therapy, treatment of the underlying cause and finally, supportive care.
1. Anticoagulation
- Improves mortality and long-term outcomes by restoring flow to the occluded vessel and preventing propagation of the thrombus (18, 19)
- Decreases the risk of disease recurrence
LMWH vs UFH
- Data is limited but it does favour LMWH (11, 12).
- However, since UFH has a shorter half-life and can be easily reversed with protamine sulfate, it is recommended to start with UFH in the critically ill patient who may require downstream procedures such as decompressive craniectomy.
- Misra et al. 2012 (20)
- An open-label study of 66 patients with CVT who were randomized to receive either dalteparin or UFH
- In-hospital mortality was 0 vs 19% for dalteparin and UFH groups, respectively
- UFH led to more hemorrhagic complications
- Less patients in the UFH group had full recovery after 3 months
- Limitations: no allocation concealment and patients in the UFH group were more severe at baseline
- Coutinho et al, 2010 (21)
- Case control study
- Compared LMWH against UFH in 421 patients
- Mortality rate and hemorrhagic complications were higher in the UFH group. However, the outcomes listed in this study were not statistically significant.
- Misra et al. 2012 (20)
- LMWH is also the treatment of choice for pregnant patients acutely and for the long-term as other agents, including warfarin and direct oral anticoagulants (DOACs) are contraindicated.
Anticoagulation in the patient with existing intracranial hemorrhage is safe
- Einhaupl et al, 1991 (19) & de Bruijn et al, 1999 (18)
- 2 RCTs, anticoagulation vs placebo
-
-
- 43% of patients had an ICH at baseline
- 3 in the placebo group developed new ICH, none in the heparin group
-
- Other observational studies and case series supported this finding
Long-term anticoagulation
- Warfarin (11, 12)
-
- Better for renal failure patients
- Duration of treatment
- 3-6 months for provoked CVT
- 6-12 months for unprovoked CVT
- Dabigatran
- Does not require regular INR monitoring or lifestyle changes
- Ferro et al, 2019 (RE-SPECT CVT) (22)
- Open label, multicenter RCT, 120 patients with acute CVT
- Compared dabigatran with warfarin
- Duration: 24 weeks, after treatment with heparin for 5-15d
- Exclusions: CNS infection, active cancer or major trauma
- Recanalization occurred in 60% of the dabigatran group and 67.3% of the warfarin group
- One patient in the dabigatran group and 2 patients in the warfarin group had hemorrhagic complications
- Limitations: small sample size, not powered to detect differences in VTE recurrence
- Life-long anticoagulation is required for patients with underlying thrombophilia
2. Endovascular therapy
- Not recommended unless patients worsen despite anticoagulation with heparin
- Siddiqui et al, Stroke, 2015 (23)
- Systematic review of 42 studies
- 185 patients treated with thrombectomy
- Results:
- Good outcome in 84% of patients
- Mortality 12%
- Worsened bleeding 10%
- Limitation: none of the studies were RCTs
- Coutinho et al, JAMA Neurology, 2020 (TO-ACT) (24)
- Open label, multicenter RCT (N = 67)
- Patients with severe CVT: altered, coma, ICH, thrombosis of deep veins
- Compared endovascular therapy vs medical management only
- Results: no significant difference in mortality or neurological outcome at 12 months
- Study was prematurely terminated due to futility
- Limitation: small sample size, was underpowered to detect small differences between the 2 treatment groups
- Siddiqui et al, Stroke, 2015 (23)
3. Treatment of underlying cause and supportive care
Seizure
- Seizure prophylaxis is recommended for patients who have had at least 1 seizure (12).
- Levetiracetam and valproate have fewer interactions with vitamin K antagonists such as warfarin. Acutely, phenytoin is still a good choice.
ICP management
- General ED management +/- decompressive craniectomy
- Evidence not sufficient to support the use of acetazolamide, ventricular drain placement, therapeutic lumbar puncture or steroids (11, 12).
Infection
- CVT secondary to infections such as meningitis, sinusitis and mastoiditis should be treated with conventional antibiotics (11)
Management – Take home points:
- Give LMWH or UFH despite evidence of intracranial hemorrhage
- Warfarin or Dabigatran for long term therapy
- Endovascular therapy is not standard of care
- Give seizure prophylaxis if patient presents with a seizure
- Treat the underlying cause (e.g. infection)
- No to acetazolamide, LP and steroids
References:
- Borhani Haghighi A, Edgell RC, Cruz-Flores S, et al. Mortality of cerebral venous-sinus thrombosis in a large national sample. Stroke. 2012;43(1):262-264.
- Ferro JM, Canhão P, Stam J, et al. Delay in the diagnosis of cerebral vein and dural sinus thrombosis: influence on outcome. Stroke. 2009;40(9):3133-3138.
- Klein DE, Libman R, Kirsch C, Arora R. Cerebral venous thrombosis: A typical presentation of COVID-19 in the young. J Stroke Cerebrovasc Dis. 2020;29(8):104989.
- Cavalcanti DD, Raz E, Shapiro M, et al. Cerebral Venous Thrombosis Associated with COVID-19. AJNR Am J Neuroradiol. 2020;41(8):1370-1376.
- Capecchi M, Abbattista M, Martinelli I. Cerebral venous sinus thrombosis. J Thromb Haemost. 2018;16(10):1918-1931.
- Ghoneim A, Straiton J, Pollard C, Macdonald K, Jampana R. Imaging of cerebral venous thrombosis. Clin Radiol. 2020;75(4):254-264.
- Thorell SE, Parry-Jones AR, Punter M, Hurford R, Thachil J. Cerebral venous thrombosis-a primer for the haematologist. Blood Rev. 2015;29(1):45-50.
- Gotoh M, Ohmoto T, Kuyama H. Experimental study of venous circulatory disturbance by dural sinus occlusion. Acta Neurochir (Wien). 1993;124(2-4):120-126.
- Yoshikawa T, Abe O, Tsuchiya K, et al. Diffusion-weighted magnetic resonance imaging of dural sinus thrombosis. Neuroradiology. 2002;44(6):481-488.
- Tanislav C, Siekmann R, Sieweke N, et al. Cerebral vein thrombosis: clinical manifestation and diagnosis. BMC Neurol. 2011;11:69. Published 2011 Jun 10.
- Saposnik G, Barinagarrementeria F, Brown RD Jr, et al. Diagnosis and management of cerebral venous thrombosis: a statement for healthcare professionals from the American Heart Association/American Stroke Association. Stroke. 2011;42(4):1158-1192.
- Ferro JM, Bousser MG, Canhão P, et al. European Stroke Organization guideline for the diagnosis and treatment of cerebral venous thrombosis – endorsed by the European Academy of Neurology. Eur J Neurol. 2017;24(10):1203-1213.
- Dentali F, Squizzato A, Marchesi C, Bonzini M, Ferro JM, Ageno W. D-dimer testing in the diagnosis of cerebral vein thrombosis: a systematic review and a meta-analysis of the literature. J Thromb Haemost. 2012;10(4):582-589.
- Meng R, Wang X, Hussain M, et al. Evaluation of plasma D-dimer plus fibrinogen in predicting acute CVST. Int J Stroke. 2014;9(2):166-173.
- Tanislav C, Siekmann R, Sieweke N, et al. Cerebral vein thrombosis: clinical manifestation and diagnosis. BMC Neurol. 2011;11:69. Published 2011 Jun 10.
- Xu W, Gao L, Li T, Ramdoyal ND, Zhang J, Shao A. The Performance of CT versus MRI in the Differential Diagnosis of Cerebral Venous Thrombosis. Thromb Haemost. 2018;118(6):1067-1077.
- van Dam LF, van Walderveen MAA, Kroft LJM, et al. Current imaging modalities for diagnosing cerebral vein thrombosis – A critical review. Thromb Res. 2020;189:132-139.
- de Bruijn SF, Stam J. Randomized, placebo-controlled trial of anticoagulant treatment with low-molecular-weight heparin for cerebral sinus thrombosis. Stroke. 1999;30(3):484-488.
- Einhäupl KM, Villringer A, Meister W, et al. Heparin treatment in sinus venous thrombosis [published correction appears in Lancet 1991 Oct 12;338(8772):958]. Lancet. 1991;338(8767):597-600.
- Misra UK, Kalita J, Chandra S, Kumar B, Bansal V. Low molecular weight heparin versus unfractionated heparin in cerebral venous sinus thrombosis: a randomized controlled trial. Eur J Neurol. 2012;19(7):1030-1036.
- Coutinho JM, Ferro JM, Canhão P, et al. Unfractionated or low-molecular weight heparin for the treatment of cerebral venous thrombosis. Stroke. 2010;41(11):2575-2580.
- Ferro JM, Coutinho JM, Dentali F, et al. Safety and Efficacy of Dabigatran Etexilate vs Dose-Adjusted Warfarin in Patients With Cerebral Venous Thrombosis: A Randomized Clinical Trial [published online ahead of print, 2019 Sep 3]. JAMA Neurol. 2019;76(12):1457-1465.
- Siddiqui FM, Dandapat S, Banerjee C, et al. Mechanical thrombectomy in cerebral venous thrombosis: systematic review of 185 cases. Stroke. 2015;46(5):1263-1268.
- Coutinho JM, Zuurbier SM, Bousser MG, et al. Effect of Endovascular Treatment With Medical Management vs Standard Care on Severe Cerebral Venous Thrombosis: The TO-ACT Randomized Clinical Trial. JAMA Neurol. 2020;77(8):966-973.


Thanks, excellent topic 👏.
Excellent review on this topic. I had a case of a young 21F on OCPs who presented with persistent headache, neck pain, parasthesias of both upper extremities associated with nausea, vomiting, and syncopal episodes who ended up having CVST of the cortical, sagittal, and transverse sinuses extending into the R IJ. I did not realize CVST could cause neck pain and parasthesias, but this article does a great job of describing symptomatology based on which cerebral venous sinuses are thrombosed.