

- What chief complaint will you manage on both an adult and pediatric emergency shift?
- When you’re running through differentials for hypotension or shock, what life threatening conditions are on the list?
- When you think of airways that keep you up at night, scenarios that could escalate to need a double set up, what is on your list?
It’s anaphylaxis. Whether you’re working in an urban tertiary centre or a remote rural clinic, you need to own this potentially fatal condition.
Within the last year, 2 major anaphylaxis organizations – the Canadian Society of Allergy and Clinical Immunology (CSACI) and the World Allergy Organization (WAO) – updated their anaphylaxis guidelines with the most up-to-date evidence, even proposing new, simpler diagnostic criteria.
There are 4 take home points from this post:
- The World Allergy Organization has developed new anaphylaxis diagnostic criteria.
- There is little to no evidence to support the routine administration of steroids in the acute phase of anaphylaxis, nor in the mitigation or prevention of biphasic reactions.
- Antihistamines should never come before, delay or replace the administration of epinephrine for anaphylaxis.
- In patients with high-risk features, extended observation (≥6h) is reasonable. In patients without high-risk features, early discharge may be appropriate (<2h).
Take Home Point 1: new Anaphylaxis Diagnostic Criteria
Previous diagnostic criteria (Figure 1a) were criticized for being too restrictive and ambiguous.
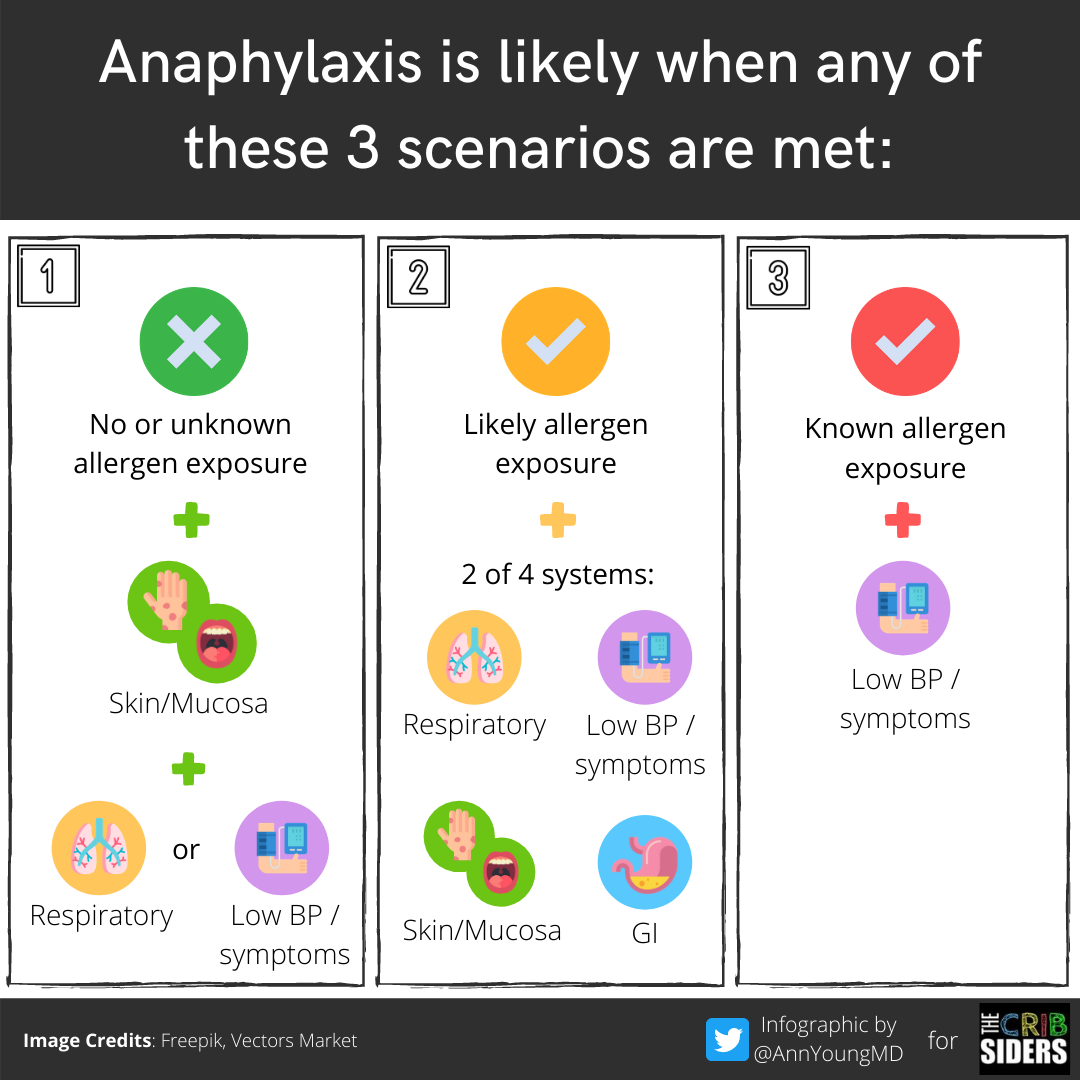
Figure 1a | old 2005 three-scenario diagnostic criteria. Brown J, Young AL, Chiu C, Berk J. “Dr. Julie Brown and Anaphylaxis; Or: How I Learned to Stop Worrying and Love Epinephrine”. The Cribsiders Pediatric Podcast. https:/www.thecribsiders.com. 9/30/20.
This led the WAO to update and clarify the previous diagnostic criteria in hopes of improving its utility. Anaphylaxis is likely when your patient has an acute onset of illness with any of the following 2 scenarios:
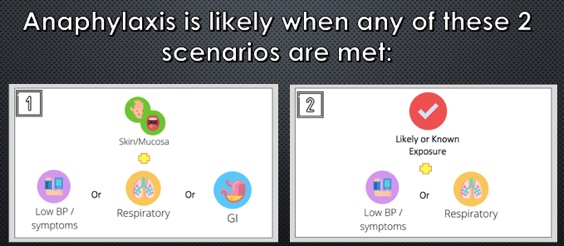
- Figure 1b1: typical skin features (i.e., diffuse urticaria, erythema, angioedema) + 1 organ system involved:
- cardiovascular: hypotension or symptoms of end organ dysfunction (e.g., syncope, hypotonia, incontinence).
- resp: hypoxemia, dyspnea, stridor, wheeze, bronchospasm.
- GI: repetitive vomiting, severe abdominal pain.
- Figure 1b2: exposure to a known or likely allergen with either:
- acute hypotension or signs of shock
- bronchospasm or laryngeal involvement
Take Home Point 2: There is little to no evidence to support the routine administration of steroids in the acute phase of anaphylaxis, nor in the mitigation or prevention of biphasic reactions
Steroids are given by doctors for 2 hypothetical benefits:
- to reduce the severity of the acute reaction
- to mitigate and/or prevent biphasic reactions
Given the maximum serum concentration for steroids occurs approximately 1-2h after administration, it is unlikely steroids would impact the acute phase of anaphylaxis.
Steroids gained popularity in the management of biphasic reactions in 2007, after a single-centre review of 103 patients showed fewer biphasic reactions in those who received corticosteroids. A subsequent Cochrane review and two follow-up systematic reviews failed to show any association between steroid treatment and biphasic reactions. This question was reviewed in the most recent 2020 update by the CSACI (Figure 2). After assessing 26 studies, no benefit from steroids was observed in the prevention or mitigation of biphasic anaphylaxis (OR 0.87, 95% CI, 0.74-1.02).
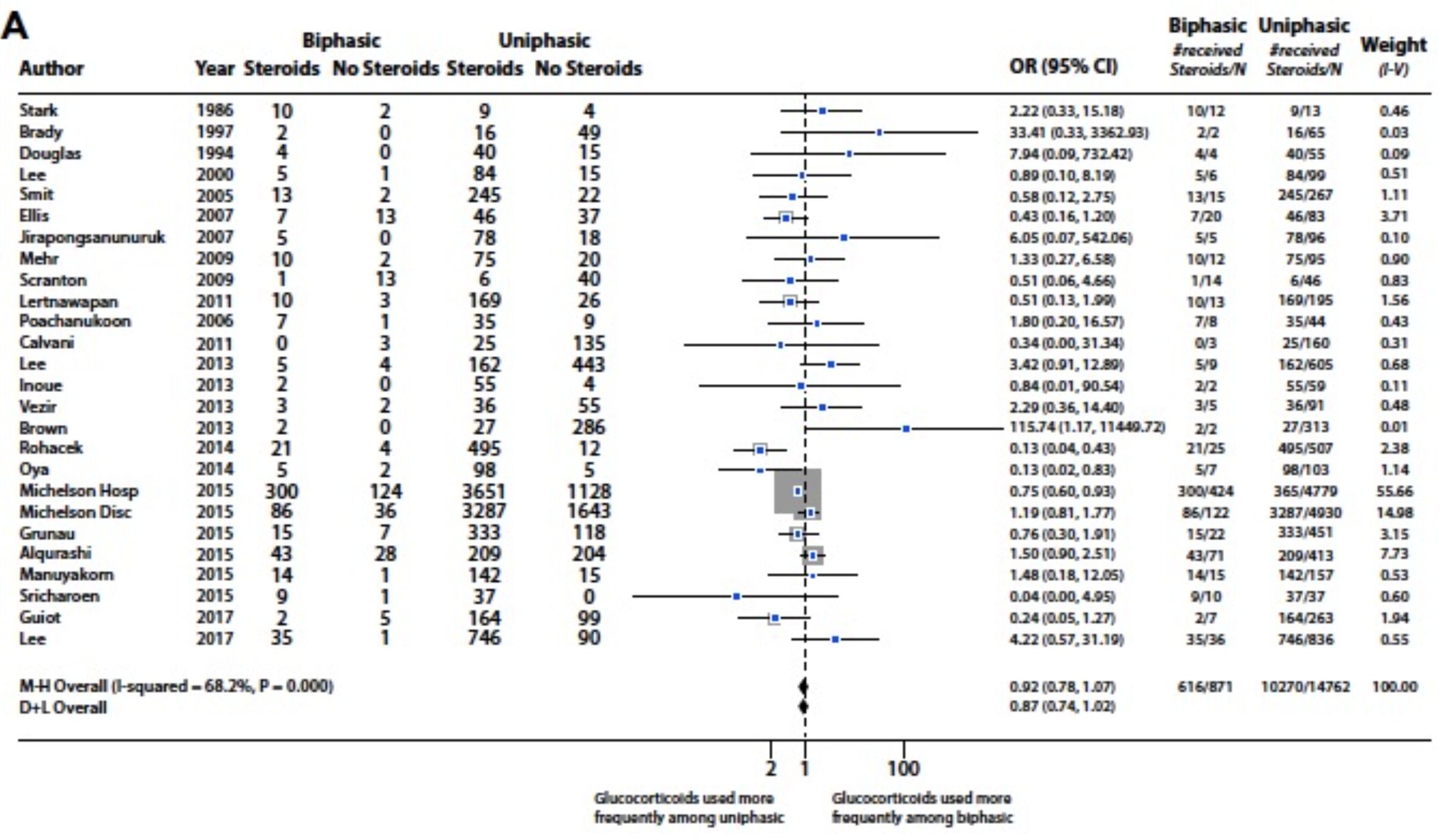
Figure 2 | can corticosteroids be used to prevent or mitigate biphasic reactions? From Shaker et. al (2020).
Take Home Point 3: antihistamines should never come before, delay, or replace the administration of epinephrine for anaphylaxis
The role of antihistamines in the management of anaphylaxis remains controversial. Two published reviews, including one 2010 Cochrane review, were unable to identify any suitable studies to assess the benefits or harms for their use in anaphylaxis. This too was explored in the most recent update by the CSACI. Their joint task force reviewed 26 articles to assess whether or not antihistamines had any impact on biphasic reactions (Figure 3).
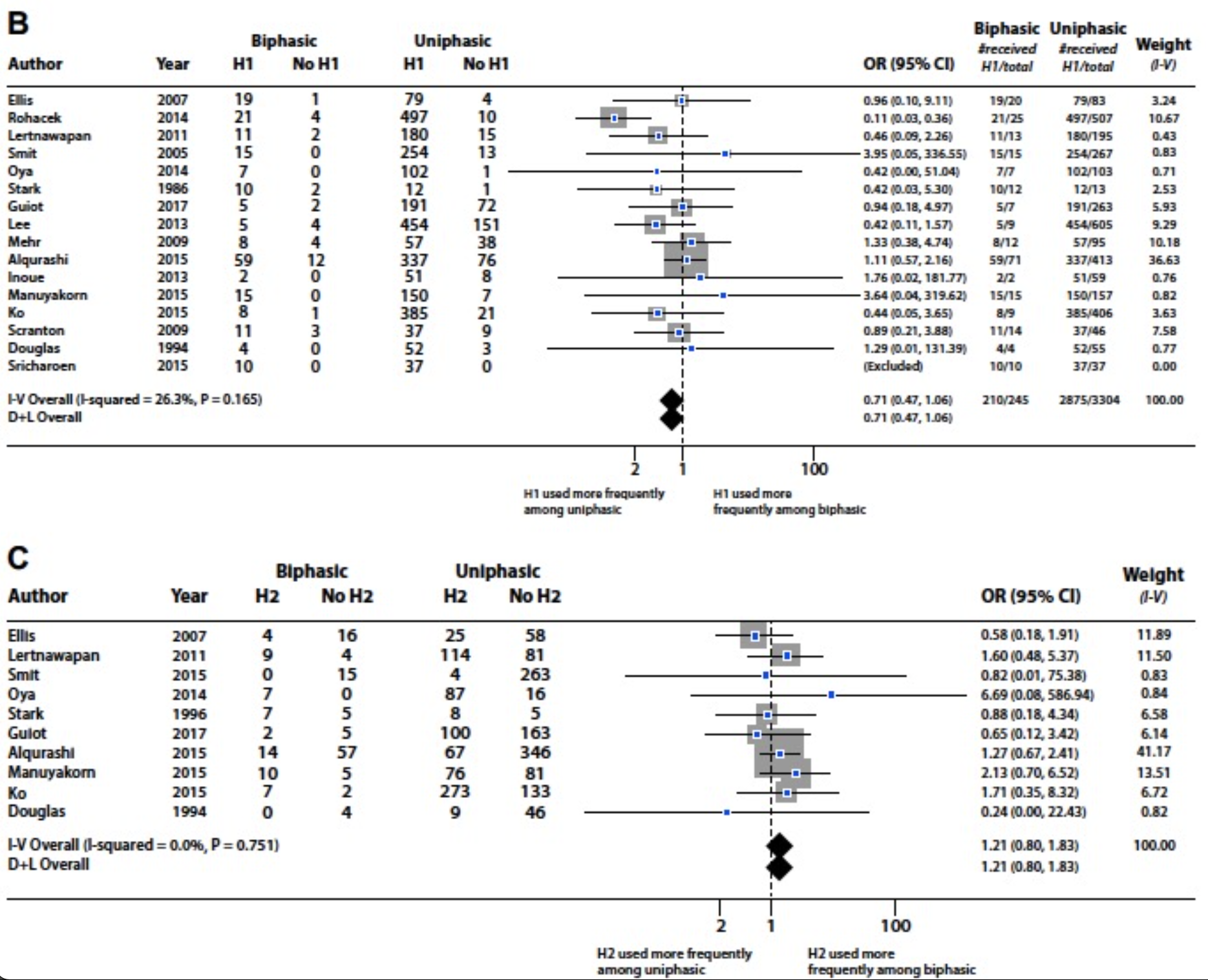
Figure 3 | can antihistamine be used to prevent or mitigate biphasic reactions? From Shaker et al. (2020).
Similar to glucocorticoid use in anaphylaxis, H1 antihistamines – like diphenhydramine – did not provide a benefit in the reduction of biphasic reactions (OR, 0.71; 95% CI, 0.47-1.06), nor did H2 antihistamines like ranitidine (H2 antihistamines: OR, 1.21; 95% CI, 0.80- 1.83).
Take Home Point 4: in patients with high-risk features, extended observation (≥6h) is reasonable. Those without high-risk features may appropriately be discharged early (<2h).
When it comes to monitoring, evidence is lacking to clearly define the optimal duration of observation. There is no clear consensus on how long someone presenting with anaphylaxis to the emergency department should be observed for.
In an ideal world, the solution to reduce morbidity and mortality from biphasic reactions would be to have all patient on monitors for an extended period of direct observation. Clearly this is not feasible nor cost-effective.
In 2019, a meta-analysis by Kim et al. attempted to establish a practical observation time to detect biphasic reactions. In this study, they had a pooled negative predictive value (NPV) after symptom resolution of 95% at 1h, 96% at 4h, 97% after 6h, with the greatest NPV being 99% at 48h (Figure 4).
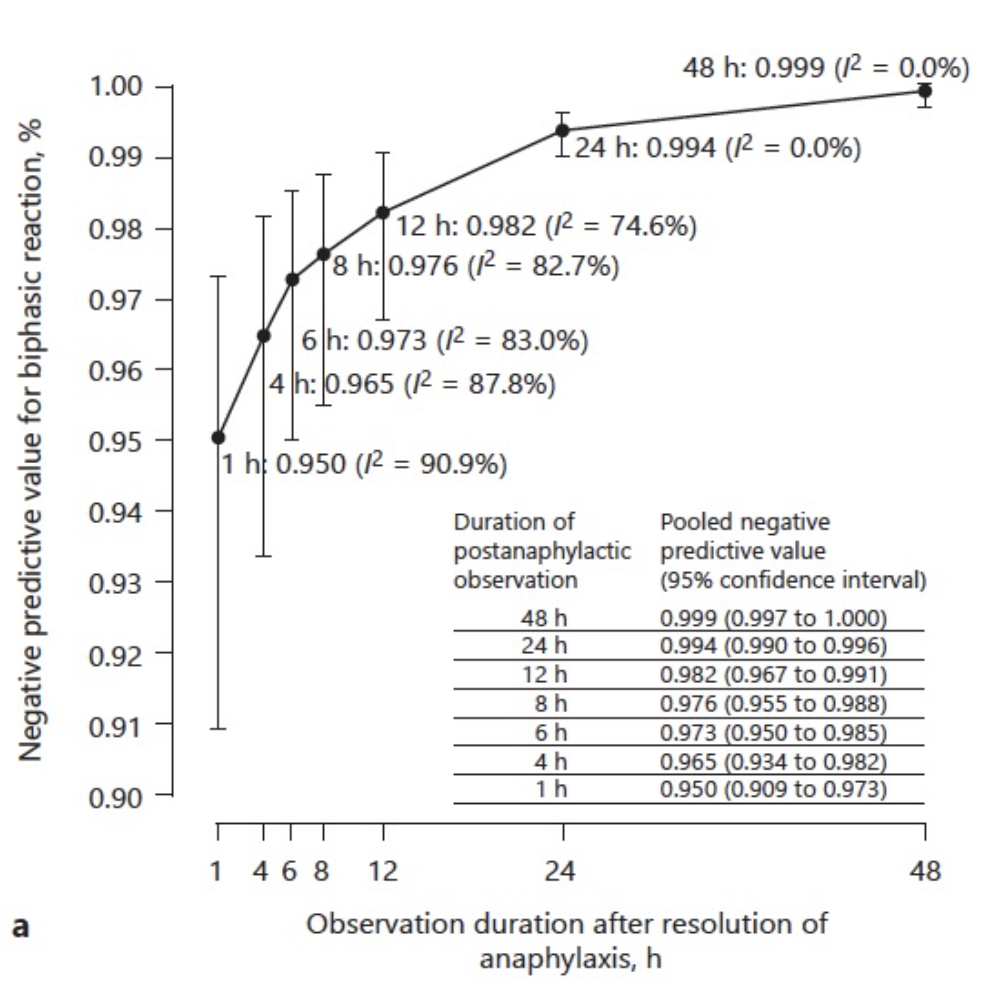
Figure 4 | NPV of observing a biphasic reaction in the ED, from Kim et al. (2019).
Each extension of observation time beyond 1h, the NPV for observing a biphasic reaction in the ED increased by only ~1%. Therefore, an extended observation time for low-risk patients is unlikely to mitigate the risk of biphasic reactions and a patient’s observation time can be guided by appropriate risk stratification.
In the most recent 2020 update, and after reviewing over 30 studies, the CSACI found that biphasic reactions were most often associated with:
- repeated (>1) epinephrine doses (OR 4.82; 95% CI, 2.70-8.58).
- severe anaphylaxis symptoms (OR 2.11; 95% CI, 1.23-3.61).
In patients who had multiple epinephrine doses, the number needed to observe to detect one biphasic reaction before discharge was 13, and 41 in patients with severe anaphylactic symptoms (Figure 5).
In the latter group, this is 246h or 10 days-worth of occupancy in a monitored bed to detect one biphasic reaction. Given that we work in a time where overcrowding, bed availability, and flow are so crucial to our functioning in the ED, an over-excessive observation time to capture one of these biphasic reactions is impractical.
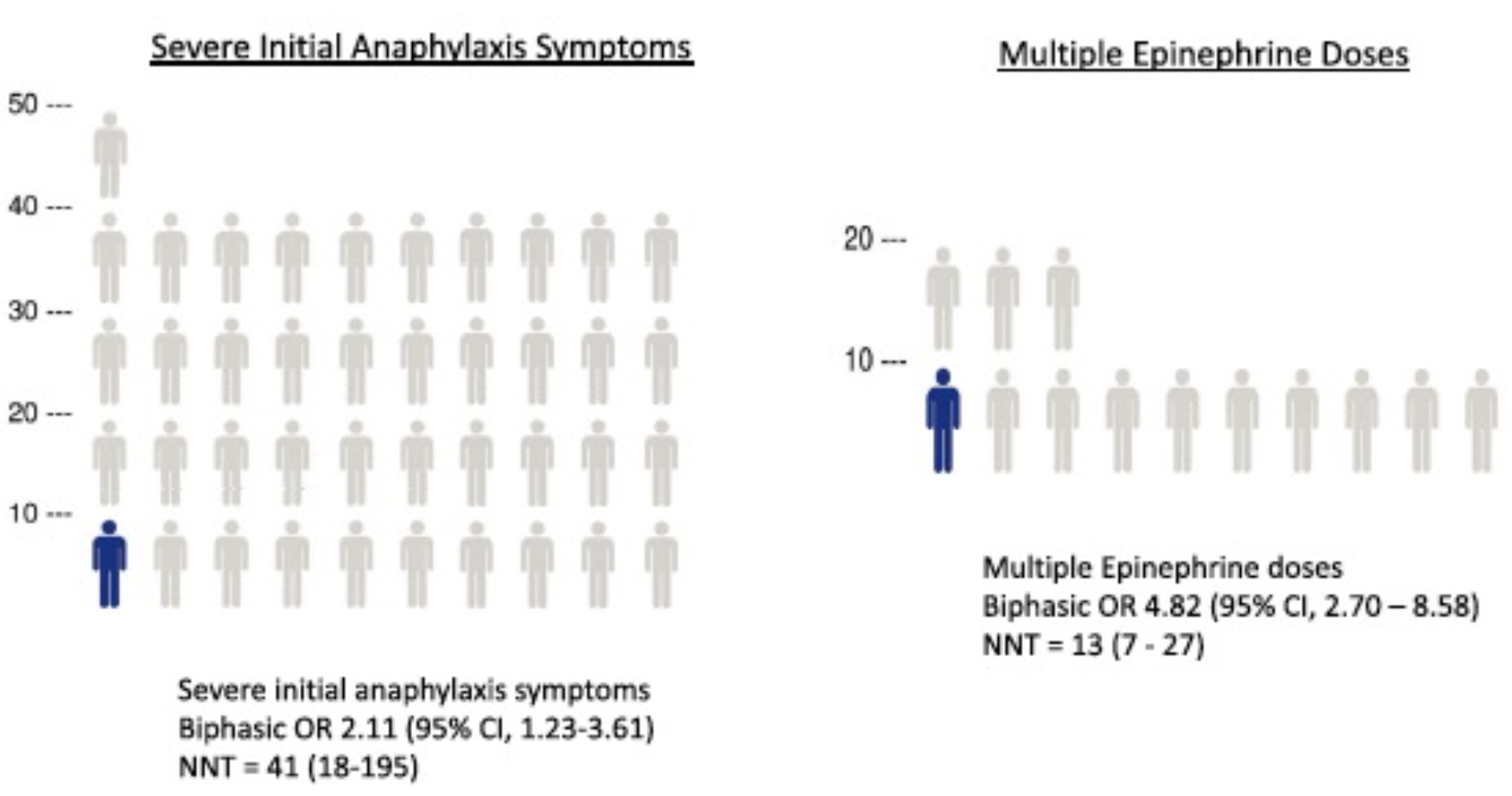
Figure 5 | number needed to treat to observe one biphasic reaction, from Shaker et al. (2020.
Up to 6h or longer of observation is reasonable:
- patients with high-risk features for biphasic reactions (multiple epinephrine doses or severe anaphylaxis); and/or
- risk factors for mortality such as lacking access to epinephrine, poor self-management skills, or lack of access to emergency medical services.
Patients without high-risk features, discharging after a 1h asymptomatic period may be reasonable, but insufficient evidence exists to establish this as policy.
Summary
At this time, there is no evidence to support the routine use of steroids. Antihistamines are an adjunct and should never come before, replace or delay epinephrine administration. Look for high-risk features, if they are present, then observing that patient for 6 hours or longer may be appropriate. But in those without, early discharge after an asymptomatic period may be appropriate.
References
- Hemlan, A. (NYGH), & Carr, D. (UHN). (2016). Episode 78 Anaphylaxis and Anaphylactic Shock – Live from The EM Cases Course – Emergency Medicine C. https://emergencymedicincom/anaphylaxis-anaphylactic-shock/.
- Cardona, V., Ansotegui, I. J., Ebisawa, M., El-Gamal, Y., Fernandez Rivas, M., Fineman, S., Geller, M., Gonzalez-Estrada, A., Greenberger, P. A., Sanchez Borges, M., Senna, G., Sheikh, A., Tanno, L. K., Thong, B. Y., Turner, P. J., & Worm, M. (2020). World allergy organization anaphylaxis guidance 2020. World Allergy Organization Journal, 13(10), 100472. https://doi.org/10.1016/j.waojou.2020.100472
- @AnnYoungMD, & FreePic, V. M. (n.d.). Anaphylaxis: All You Need to Know – The Curbsiders.
- FreePic, V. M. (n.d.). Anaphylaxis: All You Need to Know – The Curbsiders.
- Pumphrey RS. (2000). Lessons for management of anaphylaxis from a study of fatal reactions. Clin Exp Allergy;30:1144-50.
- Charmandari E, Johnston A, Brook CG, Hindmarsh PC. Bioavailability of oral hydrocortisone in patients with congenital adrenal hyperplasia due to 21-hydroxylase deficiency. J Endocrinol 2001;169:65-70.
- Ellis AK, Day JH. (2007). Incidence and characteristics of biphasic anaphylaxis: a prospective evaluation of 103 patients. Ann Allergy Asthma Immunol;98:64-9.
- Choo, K. J. L., Simons, E., & Sheikh, A. (2010). Glucocorticoids for the treatment of anaphylaxis: Cochrane systematic review. Allergy: European Journal of Allergy and Clinical Immunology, 65(10), 1205–1211. https://doi.org/10.1111/j.1398-9995.2010.02424.
- Lee S, Bellolio MF, Hess EP, Erwin P, Murad MH, Campbell RL. (2015) Time of onset and predictors of biphasic anaphylactic reactions: a systematic review and metaanalysis. J Allergy Clin Immunol Pract;3:402-8.
- Alqurashi, W., & Ellis, A. K. (2017). Do Corticosteroids Prevent Biphasic Anaphylaxis? Journal of Allergy and Clinical Immunology: In Practice, 5(5), 1194–1205. https://doi.org/10.1016/j.jaip.2017.05.022.
- Shaker, M. S., Wallace, D. V., Golden, D. B. K., Oppenheimer, J., Bernstein, J. A., Campbell, R. L., Dinakar, C., Ellis, A., Greenhawt, M., Khan, D. A., Lang, D. M., Lang, E. S., Lieberman, J. A., Portnoy, J., Rank, M. A., Stukus, D. R., Wang, J., Riblet, N., Bobrownicki, A. M. P., … Wickham, A. (2020). Anaphylaxis—a 2020 practice parameter update, systematic review, and Grading of Recommendations, Assessment, Development and Evaluation (GRADE) analysis. Journal of Allergy and Clinical Immunology, 145(4), 1082–1123. https://doi.org/10.1016/j.jaci.2020.01.017.
- Sheikh A, Ten Broek V, Brown SG, Simons FE. H1-antihistamines for the treatment of anaphylaxis: Cochrane systematic review. Allergy. 2007 Aug;62(8):830-7. doi: 10.1111/j.1398-9995.2007.01435.x. PMID: 17620060.
- Choo, K. J., Simons, F. E., & Sheikh, A. (2012). Glucocorticoids for the treatment of anaphylaxis. The Cochrane database of systematic reviews, 2012(4), CD007596. https://doi.org/10.1002/14651858.CD007596.pub3.
- Kim TH, Yoon SH, Hong H, Kang HR, Cho SH, Lee SY. (2019). Duration of Observation for Detecting a Biphasic Reaction in Anaphylaxis: A Meta-Analysis. Int Arch Allergy Immunol. 2019;179(1):31-36. doi: 10.1159/000496092.. PMID: 30763927.
- Brown J, Young AL, Chiu C, Berk J. (2020). “Dr. Julie Brown and Anaphylaxis; Or: How I Learned to Stop Worrying and Love Epinephrine”. The Cribsiders Pediatric Podcast. https:/www.thecribsiders.com.


Trackbacks/Pingbacks