Did you know that your patients could be upset with you and your care AFTER you see them? You’re wondering how could this happen, I was friendly, polite and approachable when I saw them. It turns out, in this new world of electronic medical records (EMR) with all notes available to patients to read this is happening more frequently than you think. How often? Approximately 10% of patients found something in their chart offensive or judgemental according to this excellent study by Fernandez et al. via Journal of General Internal Medicine.
On a personal note I became aware of this issue when we went to an EMR in 2019. I was always blessed with illegible writing, considering I could barely read my own notes I was not too concerned about patients reading my notes. We also didn’t make our notes available to them directly, meaning unless they went to health records they didn’t see our note. I know, I know. Not good excuses but I’ve realized I have to change my ways.
Now I suggest you read the article yourself, but as a summary from this article here are some things you and I can do to make sure our patients remain happy with our care long after they leave the Emergency Department (ED).
Avoid
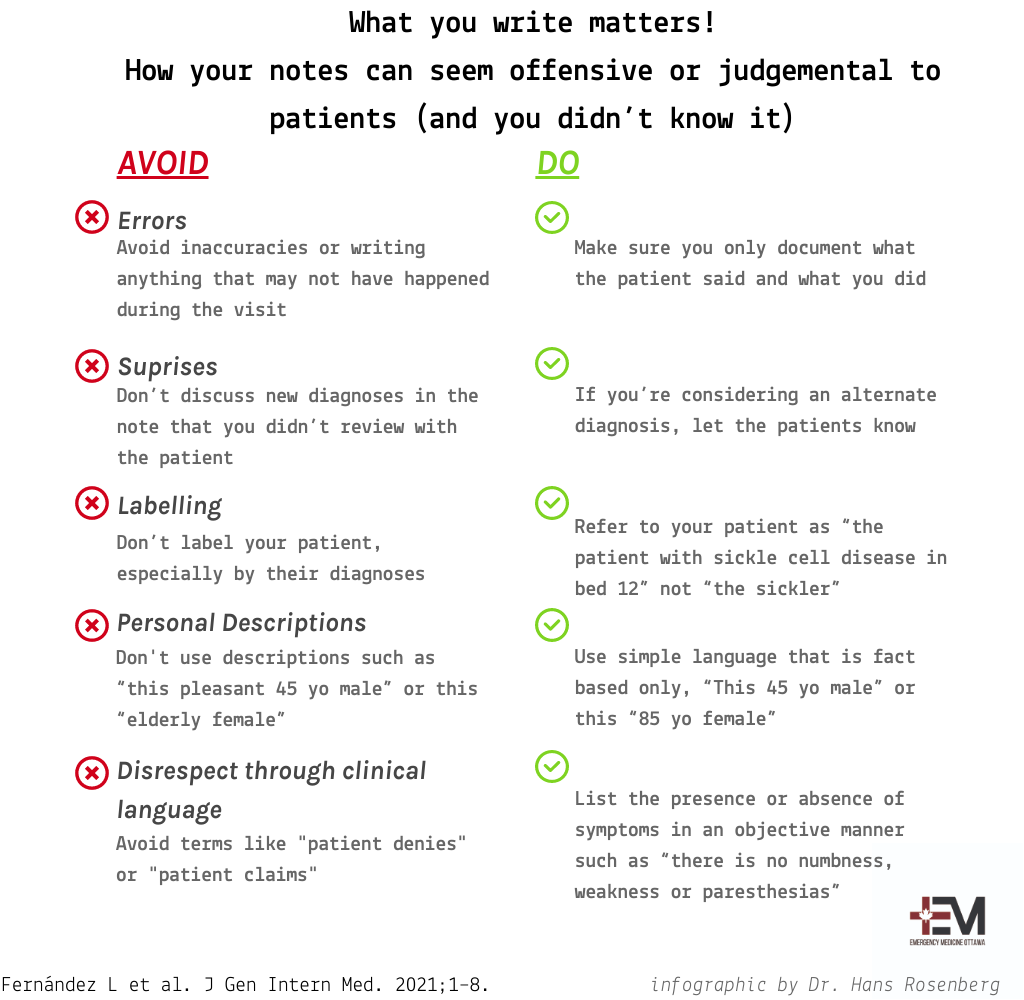
Errors: this seems intuitive but whether it’s a complete accident or intentional (hopefully this is never the case) do your best to avoid inaccuracies or writing anything that may not have happened during the visit.
Do
Do you have a standard template for your cardiorespiratory exam? You may use it as a quick way to document the encounter. But it might include something in the exam that you didn’t do. Patients are aware of what we do during our encounters and what we ask. Make sure you only document what the patient said and what you did. Are you someone who documents at the end of your shift? This is a time of high risk to add/omit something that happened as you don’t recall the details. Writing the history right away and leaving the physical exam/impression and plan until the end may help avoid these errors.
Avoid
Surprises: don’t discuss new diagnoses in the note that you didn’t review with the patient.
Do
Here’s a common scenario, you see a patient for chest pain. You believe it’s more related to stress or anxiety. You work them up for ACS and the work-up is negative. Wonderful! But on your note, you write that you believe the underlying cause is anxiety, yet you didn’t discuss it with your patient. If you’re considering an alternate diagnosis, let the patients know. It might be the first step in them heading towards solving their mental health issues.
Avoid
Labelling: don’t label your patient, especially by their diagnoses.
Do
Refer to your patient as “the patient with sickle cell disease in bed 12” not “the sickler”. The patient in bed 8 is not “an obese diabetic” they are “a patient with obesity/high BMI and diabetes”.
Avoid
Personal Descriptions: don’t use descriptions such as “this pleasant 45 yo male” or this “elderly female”. This doesn’t add anything to the patient’s course and can indicate that at this visit they are “pleasant”, yet at others they are not or it can set them up for bias based on their age.
Do
Use simple language that is fact based only, “This 45 yo male” or this “85 yo female”.
Avoid
Disrespect through clinical language: using clinical language which can seem to disregard or question a patient’s concerns. Avoid using terms like “patient claims” or “patient denies numbness or paresthesias”.
Do
List the presence or absence of symptoms in an objective manner such as “there is no numbness, weakness or paresthesias”
Each one of these uses of language in our notes can seem minor, but when you put them together in the patient note they might feel like you are offending or judging them. Take a look at a few or your most recent charts, do they contain a number of the above statements? Mine surely did. Some small changes might make a huge difference in how our patients interpret what we say and ensure that trust and respect is maintained in the clinician-patient relationship.
What are your tips to ensure that we write our notes using language that patients can understand, is accurate and does not cause them any undue feeling of being offended/judged? Let us know in the comments!