
In this comprehensive guide, Dr. Tetyana Maniuk, a third-year FRCPC Ottawa Emergency Medicine resident summarizes the existing evidence on anorexia and eating disorders specific to the emergency department. Highlighting everything from signs and symptoms to watch out for, to associated complications, and a list of patient and parent resources, this is an invaluable post to reference for your next shift.
Eating Disorders in the Emergency Department
Are we equipped to take care of patients with eating disorders?
-
- Of 162 American emergency physicians interviewed, >90% were not aware of any guidelines to treat patients with eating disorders or local resources; 85% agreed further education is required.1
- A survey of 637 programs (internal medicine, pediatrics, family medicine, psychiatry, adolescent medicine) in 2014 found that only 42 offered a formal, scheduled rotation for eating disorder training.2
Why should we care?
- Because they are common
-
- New estimates endorse a prevalence of any eating disorder to affect 1 in 7 men and 1 in 5 women; 95% of the time this happens prior to age 25.3
- In fact, a study that screened 1,795 21–to-65-year-old adults who visited the emergency room for any concern found that almost 16% screened positive for an eating disorder.4
-
- Because they are a missed population
-
- Two thirds of patients with eating disorders will never be diagnosed
-
- Of those that do get diagnosed, there is often a significant delay to treatment.4
- Delay in treatment is an independent risk factor for increased mortality.
-
- Two thirds of patients with eating disorders will never be diagnosed
-
- Because they come to see us
-
- Patients with ED are 1.6x more likely to come to the emergency department compared to controls.5
-
Anorexia Nervosa (AN) Definition & Epidemiology
- Anorexia is a psychiatric disorder resulting in a state of severe malnutrition from starvation.6
- Approximately 1 in 100 women will be affected by anorexia in their life.6
- It has the highest mortality rate in any psychiatric disorder6
-
- 18x higher suicide risk
- Mortality rate nearing 6% per decade
-
- DSM5 criteria:
- Diagnosis is based on having 3/3 criteria:
-
- Food restriction that results in weight lower than what would be expected of the patients height / weight / age OR failure to gain weight
- Fear of gaining weight or being fat
- Presence of distortions (e.g., perceiving themselves as fat)
-
- Diagnosis is based on having 3/3 criteria:
- Furthermore, there are two subtypes:
-
-
-
- Restricting type (AN-R)
-
- Patient has not engaged in binge-purge behavior in the past three months
- Associated with better prognosis
-
- Binge – Purge type (AN-BP)
-
- Patient has engaged in binge-purging behaviors in the past three months
- Purging comes in many forms including vomiting, laxative abuse, diuretic abuse, or excessive exercise.
-
- Restricting type (AN-R)
-
-
- Note Cross-over exists7
-
-
-
-
- Restriction > purging crossover in 62%
- Binge-purge > restrictive in 43%
-
-
-
-
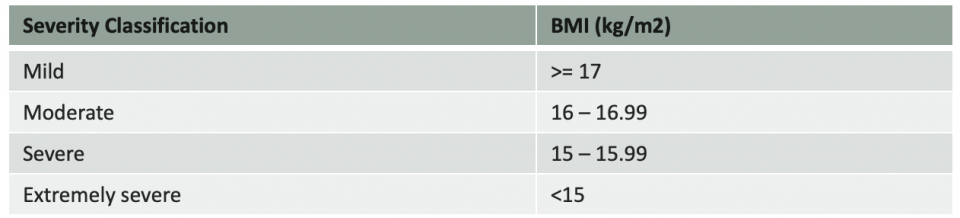
Table 1. Outline of the severity of anorexia nervosa based on BMI
Aetiology
- Twin based studies found a heritability of 50-60%6
-
- Multiple genetic loci implicated in AN
-
- Current model endorses genetic and environmental factors along with symptoms of a starvation syndrome to explain the occurrence of anorexia
Overall Signs & Symptoms
- Tend to present with GI concerns5
- They may not self-report history related to eating disorder because they often have a very distorted view of their eating disorders and often do not recognize there is a problem, or that the problem may be contributing to their chief concern
-
- Dr. Bissada endorses that low weight and hypokalemia should make you worry about AN.
-
- Findings on history7
-
-
- Ages 16-25, particularly females though rising incidence in males
- Perfectionist
- High achiever, particularly competitive athletes
- History of sexual abuse
- Depression or anxiety
- Substance abuse
- Purging behaviors
- Excessive dieting
- Eating rituals (e.g., taking a long time to eat, cutting food up into small pieces, using excessive seasoning)
-
-
Emergent Department Signs & Symptoms
Emergency Department Presenting Symptoms
- Tend to be GI related
-
- Bloating
- Constipation
- Abdominal pain NYD
-
- Weight loss
- Amenorrhea
- Fatigue
- Suicidality
Emergency Department Presenting Signs7
- Hypotension, bradycardia
- Lanugo hair
- Cachexia
- Acrocyanosis
- Low weight
- Nonspecific skin changes
-
- Carotene pigment
- Hair loss
- Dry skin
- Delayed wound healing
-
- Induced vomiting signs
-
- Parotid hypertrophy
- Poor dental hygiene, erosion of dental enamel
- Russel’s sign (calluses on knuckles)
-
Note: Later in the article we will discuss specific laboratory abnormalities.
Screening for Eating Disorders
- Similar to the CAGE questionnaire, SCOFF is a 5-question questionnaire screening for AN and bulimia in particular, but it does not screen well for other eating disorders listed in the DSM-5.
- A recent meta-analysis endorse a sensitivity of 86% and a specificity of 83% when screening for any eating disorder however does have higher sensitivity and specificity if used to only screen for anorexia nervosa or bulimia.8
Scoff questionnaire
- Do you make yourself sick because your feel uncomfortably full?
- Do you worry you have lost control over how much you eat?
- Have you recently lost 14 pounds in a 3-month period?
- Do you believe yourself to be fat when others say you are thin?
- Would you say the food dominated your life?
1 point for each question. A score 2 or more is significant.
- If used, can consider administering it in a written format if possible as studies show increased disclosure when patients answer in a written way.9
Local experts do not recommend use of the SCOFF questionnaire.
How to Interview Patients
- Motivational interviewing has the most robust supportive data.
- Ensure to frame questions around the chief concern and ask without judgement
-
- “Sometimes suffering from constipation can change how you eat, has that happened to you?”
- “Changing how you eat can sometimes result in a change in weight, has that happened to you?
- “How do you feel about your weight loss?”
- “Have you done anything to keep losing weight?”
-
- Provide empathetic and validating support to the patient
- It may help to bring print outs of laboratory or radiological evidence of disease to show patients
- Patients have strong distortions and denial about their disorder, and it may help to bring objective evidence of ailment
- Always assess risk for suicide, as it is the cause of mortality in 20% of these patients
Electrolyte Abnormalities
Hypophosphatemia
- Often cited as the most important component of refeeding syndrome, but this may be due to bias and hypokalemia and hypomagnesemia may be just as important.21
- Phosphate is integral to creation of ATP.
-
- If stores are deplete due to use and intracellular shift, this can result in muscle weakening which importantly can affect the heart and diaphragm.
- Also has a role in conduction and can precipitate cardiac dysrhythmias.
-
- Phosphorus is also integral to production of 2,3 DPG and depletion will cause decreased production of 2,3 DPG and therefore a left shift on the HGB-O2 affinity curve leading to reduced O2 release.21
Hypokalemia
- From stimulation of Na+/K+ ATPase by insulin.21
- As we know, hypokalemia can result in aberrant electrical impulses and muscle weakness.
Refeeding Syndrome
- No concrete definition.
- ASPEN (2020) guidelines21 define refeeding syndrome as:
-
- “[Refeeding syndrome], conceptually, as a measurable reduction in levels of 1 or any combination of phosphorus, potassium, and/or magnesium, or the manifestation of thiamin deficiency, developing shortly (hours to days) after initiation of calorie provision to an individual who has been exposed to a substantial period of undernourishment.”
-
- Populations that are affected include AN, malabsorption disorders, patients with poor oral intake (such as those with dementia).
- The body uses energy in multiple phases throughout the day, including postprandial, post-absorptive and fasting states.21
-
- As the fasting state increases, energy reserves are depleted with increased use of electrolytes and vitamins.
- This is exacerbated by self-induced purging, or conditions that have chronic diarrhea or vomiting.
- If glucose is re-introduced after a period of prolonged fasting, there is an overproduction of insulin.
- Insulin drives phosphorus and potassium into the cells through phosphorylation of glucose > glycolysis and stimulation of ATPase.
- This causes a rapid fall in phosphorus, potassium and magnesium
-
- It is not clear the pathophysiology of magnesium depletion in refeeding syndrome.21
-
-
Patients at risk of refeeding syndrome
- No good screening test exists to predict which patients will have refeeding syndrome.
- However, the population at risk appears to be prolonged malnourishment especially if there is also presence of electrolyte abnormalities.21 Below is a list of high-risk disorders for refeeding syndrome:
-
- AN
- Patients who are incapable of feeding themselves (e.g., dementia, mental health disorders)
- ETOH and substance use disorders
- Chronic malabsorptive conditions (such as bariatric surgery, celiac disease) with acute electrolyte loss conditions (such as gastroenteritis)
- Patients in areas of famine, refugees, migration
- Child abuse
- Acute weight loss (for example in body builders preparing for a competition)
- Critically ill patients
- Malignancy
-
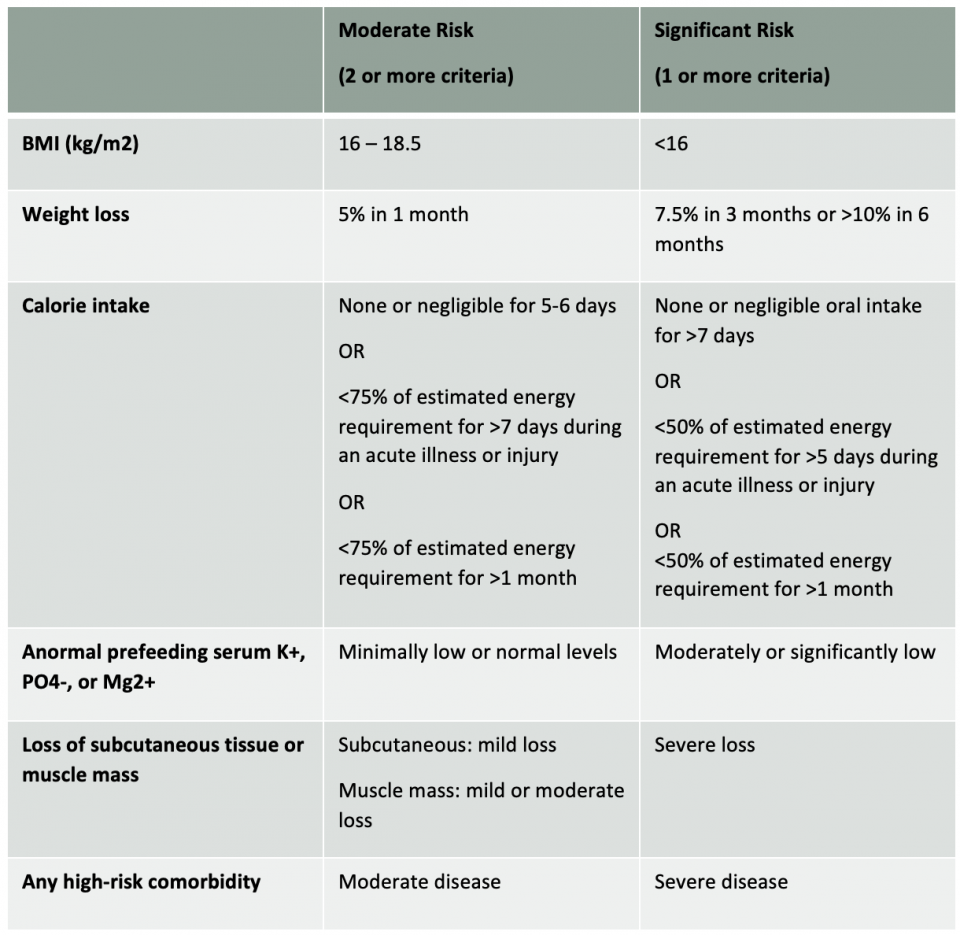
Table 2. Stratifying adult patients at moderate and severe risk of refeeding syndrome. Table taken and adapted for clarity from ASPEN 2020 guidelines.21
How to prevent refeeding syndrome
- Varied and multiple guidelines
- Most guidelines endorse starting to refeed at 5-10 kcal/kg/day > using lower end for more severe cases.21
- Some studies support aggressive refeeding in AN with 1100 – 1600 calories / day immediately.22
-
- For those who are critically ill, more cautious refeeding is suggested.
-
- Likely we will not see acute refeeding syndrome as the chief presentation, but we should be cognizant of its prevention.
- Consider an 80 kg adult:
-
- 80kg x 10 kcal/kg= 800 kcal over 24 hours, which leads to ~33 kcal / hour
- One litre of D5NS has 200 kcal. Now imagine that as a bolus.
-
- Thus: unless hypoglycemic, do not give dextrose if patient is being admitted. Especially: do not give glucose if patient has underlying electrolyte abnormalities.
- Check potassium, phosphorus and magnesium
-
- Replete them to aim for a normal range.
- Do not supplement prophylactically if already normal.
- Consider administration of thiamine 100 – 500 mg IV.21
-
- Consider an 80 kg adult:
Gastrointestinal Complications
- A very common concern (>90%), especially in patients with AN-R15
Dysphagia
- Due to lack of use (as well as GERD and frequent vomiting in binge-purge subtype), atrophied and weakened pharyngeal muscles can lead to dysphagia and aspiration.15,16
-
- If this is noted, a speech language pathologist assessment should be considered.
-
- Conflicting evidence if patients with anorexia have increased risk of developing achalasia.16
Acute gastric dilation
- Patients at the end of a severe binging/overeating episode are most at risk for acute gastric dilatation.16
-
- If there is severe gastric dilation that compresses gastric venous return, gastric necrosis can develop and then lead to perforation. Mortality is 80%.
-
- Thought to be secondary to delayed gastric emptying and motility.
-
- If stable, conservative management can be trialed with gastric decompression and supportive management.
- Surgical treatment can be considered if medical management fails.
-
- Complications can include gastric necrosis.
- Rare complications reported are acute pancreatitis, acute cardiac output impairment, SMA syndrome, acute renal failure, leg ischemia, duodenal ileum.
-
-
Gastroparesis
- Unknown when in the course of disease this develops or when it resolves with treatment.16
-
- Thought to be the bodies mechanism to extract as much nutrients as possible for the little food it does receive.16
- Normal gastric emptying is approximately 60 min, in patients with AN it is ~2.5 hrs.
-
- Due to symptoms, creates a negative feedback loop for patients preventing them from eating.16,17
-
- Patient with delayed gastric emptying reported more feelings of early satiety, nausea, sadness and anxiety.
-
- Can consider a trial of metoclopramide 2.5 mg PO or domperidone 10 mg 30 min before meals; of course caution should be used regarding QT prolonging effects of these medications and an ECG should be performed and binge/purge behavior evaluated.16
SMA syndrome
- Can present in severe AN due to loss of retroperitoneal fat pad that normally separates the SMA and aorta from duodenum resulting in a mechanical small bowel obstruction.16
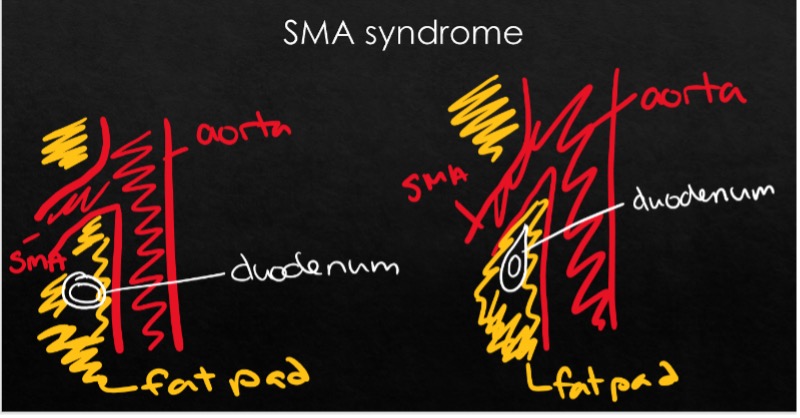
Figure 1. Visual representation of normal calibre of fat pad separating the SMA and aorta (left) and decreased fat pad causing squishing of the SMA and aorta in states of malnutrition (right).
- Diagnosed with CT abdomen with contrast
- Aortomesenteric angle <25 degrees
- Aortomesenteric distance <8mm
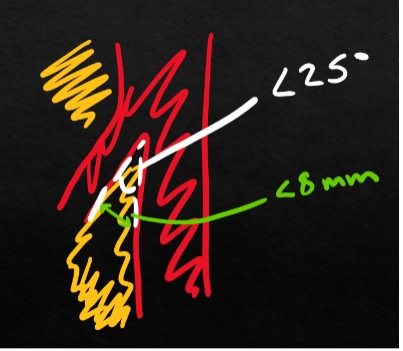
Figure 2. Visual representation of diagnostic criteria of SMA syndrome on CT scan.
- In most cases this resolves with supportive management (NG decompression, admission, monitoring) and eventual refeeding. Due to high resolution rates with refeeding, surgery is rarely indicated.16
Constipation
- Multifactorial due to diet, dehydration, gastroparesis and pelvic floor dysfunction due to muscle atrophy.17
- Rarely, rectal prolapse has also been reported
- Should only prescribe osmotic laxative such as peg lax as stimulants have potential for abuse.
Cardiovascular Complications
Vital signs
- Almost half of patients with AN will have bradycardia10
- This is thought to be secondary to increased vagal tone.
- Bradycardia is so common that a heart rate (HR) >70 should be considered tachycardic and patients should be evaluated for cause of increased sympathetic tone.11
- Their HR can rise to 120-150 with seemingly minor exertion such as standing up.
-
- This is debated whether it’s from orthostatic hypotension or as physiological response of decreased stroke volume and left ventricle atrophy.
- This can differentiate bradycardia in AN versus bradycardia in an individual who is very athletic (as a patient who is very athletic will not show this increase in HR with minimal exertion.
-
- Majority will also have hypotension and hypothermia7
-
- Up to 85% of patients show resting hypotension12
-
Cardiac function
- 87% of patients with AN suffer from cardiovascular complications.12
- In states of chronic and severe malnutrition, there is cardiomyocyte atrophy – specifically there appears early loss of left ventricular mass.11-13
-
- The proposed mechanism of change is due to increased vagal tone to decreased energy consumption > this leads to changes in contractility and decreased preload and subsequent cardiac atrophy.
-
- However, studies do not consistently find decreased ejection fraction and most studies do find that ejection fraction is normal in patients with non-acute presentations of AN despite common findings of decreased cardiac output.13
-
- There have been new research supporting decreased diastolic function.13
-
- Regardless, it would be wise to be judicious in fluid use due to demonstrated cardiac remodeling, atrophy and decreased cardiac output in this population in the emergency room.
Mitral valve prolapse11
- While in the general population the prevalence of MVP is 0.6 – 2.4%, the prevalence of MVP in the patient with AN is 33-66%.
-
- This is likely due to the aforementioned cardiac atrophy causing prolapse of the mitral valve and other not yet known multifactorial factors.
-
- Physical exam may reveal mid-systolic click and decrescendo systolic murmur.
- Can be the cause of syncope, dyspnea and palpitations in this population.
-
- Consider an outpatient ECHO if there are any concerns.
-
Pericardial effusion11
- Is more common in this population with an approximate 33% occurrence rate.11
- It tends to be asymptomatic and resolves with refeeding, however tamponade has been rarely reported.
- The pathophysiology is not yet known.
- It is not yet elucidated which patients are at risk for developing a pericardial effusion.
Dysrhythmias12
- Most often, patients with AN with sinus bradycardia. The bradycardia gets worse with longer duration of disease and lower BMI. At the extremes, junctional escape rhythms can develop.
- Due to left ventricular atrophy, right axis deviation can be seen on ECG .
-
- The ECG may show low voltage due to atrophy or pericardial effusion.
-
- QT prolongation has been historically thought as the cause of sudden death in patients with severe starvation.
-
- This is likely not true in AN14
- A study of 906 patients admitted for ED found that only 11 patients had QTC >500 ms and all of these patients had other reasons for prolonged QTC (such as hypokalemia or QT prolonging medications).
- This is likely not true in AN14
- More modern theory endorses that it is QT dispersion that causes fatal dysrhythmiass.
-
- QT dispersion is measured based on the maximum variability within one lead of longest and shortest QT interval.
- Believed to be a marker of ventricular excitability
-
-
- Few studies provide concrete evidence of the cause of sudden cardiac death in this population. A pilot study published in 2020 by Farasat et al., implanted a cardiac monitor and tracked 11 patients with severe AN for 10 months. It was found that two participants demonstrated sinus pauses and SVT.24
Neurologic Complications
- Loss of gray and white matter leads to (sometimes irreversible) cognitive impairment.
-
- Starvation has also been noted to cause depression, hyper focus on food and eating, and anxiety.18
-
- Thalamic changes lead to an increased prevalence of hypothermia.
- Loss of protective subcutaneous tissue damages peripheral nerves leading to neuropraxia.19
Hematologic Complications
- Leukopenia (50%), anemia (10%), and thrombocytopenia (10%) can be seen in anorexia.15
-
- This is believed to be from gelatinous marrow transformation where fat is replaced by mucopolysaccharides in bone marrow.
-
- Patients can have significant neutropenia, but despite neutropenia patients with anorexia do not generally appear to be at increased risk of opportunistic infections.15
Endocrine Complications
Hypothalamic amenorrhea
- Afflicts almost all females with AN.
- Does not mean they are not ovulating > always ensure to do a pregnancy test.
- Rx: Do not prescribe OCP. The only warranted treatment is refeeding.
-
- New data showing some evidence for transdermal estrogen but this should be left to the specialist physician involved in the patients care.10
- Bisphosphonates are generally not recommended to women of reproductive age due to potential teratogenic effects.20
-
Pseudo-Bartter Syndrome7
- Result of chronic dehydration and hypokalemia resulting in contraction alkalosis à activation of renin -angiotensin-aldosterone system à causes increase in circulating aldosterone.
- Increased aldosterone causes increased sodium and water retention.
- Thus, bolusing even 1L of fluids can cause significant edema to develop (can be up to 10-15lbs!)
-
- This can occur acutely in the emergency room or within days of discharge.
- This can result in patients associating the emergency room with weight gain, and may make them fear seeking further medical attention
-
- As a result, if a patient has moderate to severe anorexia or significant binge/purge behaviours be judicious with your fluids.
- Pseudo-Bartter syndrome takes weeks to correct but it does correct with refeeding.
Renal Complications
- Can develop CKD from chronic dehydration and hypokalemic nephropathy though is uncommon.
Skeletal Complications
Osteoporosis and Osteopenia
- AN causes profound alterations in the hypothalamic-pituitary axis and predisposes patients to osteoporosis and bony injuries.
- Due to its propensity to appear in adolescence, most patients never reach peak bone mineral density (BMD).
- Having AN for as little as 6-12 months results in significant bone mineral density loss.
-
- 2.5% loss per year of anorexia.20
-
- In adults, osteopenia is present in 92% of this population, osteoporosis in 40%.20
- Males with AN have worse bone density loss than females.
- BMD loss due to AN primarily affects trabecular bone
-
- Thus, hip or low back pain (even if atraumatic) should be evaluated with imaging in a patient with a history of, or active, AN.
-
- While alone it is not sufficient to increase bone mass, patients with AN should have optimized Ca and vit D supplementation.20
Prognosis
- There is strong evidence for better outcomes with earlier interventions therefore giving patients resources to start treatment is of outmost importance.15
-
-
- 30-60% recover completely
- 20% residual symptoms
- 20% do not show any response to treatment
-
Inpatient vs. Outpatient Management
Table 3. Table taken from Queensland admission algorithm for patients with eating disorders.
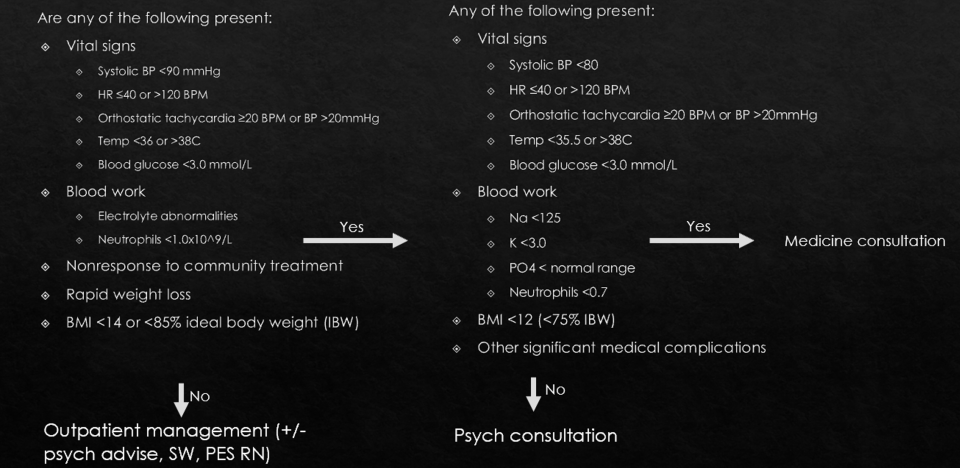
Above is an example of the criteria developed by Queensland, Australia where there was stakeholder buy-in between the in-patient eating disorder unit, psychiatry, medicine and emergency medicine. For more details of their admission algorithm for patients with eating disorders, please follow the following link.
Outpatient Resources for Patients with Eating Disorders
Outpatient resources
- National Eating Disorders
- Includes a call/chat/text option for acute crisis.
- ROAR (Reach Out and Recover)
- Allows patients to document their symptoms and the website generated a report to be printed for health care provider.
- NEDIC (National Eating Disorder Information Centre)
- Top-bar Get Help > ollow prompts to obtain local groups and individual therapists who have listed themselves as specializing in eating disorders.
- CCI – Disordered eating
- Provides multiples worksheets for patients and information sheets
- For example:
- Unhealthy exercise
- Vomiting and your health
- Normal eating vs disordered eating
- For example:
- Provides multiples worksheets for patients and information sheets
Caregiver Resources
- PLEO (Parents’ Lifeline of Eastern Ontario)
- Fee for service.
- Support for parents with children < 25 years of age who suffer from an eating disorder.
- Parent’s helpline available.
- Can also refer parents with their consent and they will get a call themselves.
- F.E.A.S.T
- Online support group forum.
- Feed Your Instinct (FYI)
- Website for parents who are concerned their child may have an eating disorders and provides education and fantastic tool kits to help with management.
Ottawa Specific Resources
- TOH Eating Disorders Clinic
- For concerning outpatient cases, can send referral for triage to day-hospital or inpatient management.
- EPIC > Psychiatry > Eating Disorders Clinical at The Ottawa Hospital
- Hopewell **
- Support groups, forums, information sessions
- Self-referral
- Ottawa CBT **
- Self-referral
- Blossom Counselling Centre
- Sliding scale
- Self-referral
- Firestone CBT
- Self-referral
**Highly recommended by local expert specializing in eating disorders.
References
- Ma C, Gonzales-Pacheco D, Cerami J, Coakley KE. Emergency medicine physicians’ knowledge and perceptions of training, education, and resources in eating disorders. J Eat Disord [Internet]. 2021 Jan 6 [cited 2021 Jan 20];9. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7789763/
- Mahr F, Farahmand P, Bixler EO, Domen RE, Moser EM, Nadeem T, et al. A national survey of eating disorder training. Int J Eat Disord. 2015 May;48(4):443–5.
- Ward ZJ, Rodriguez P, Wright DR, Austin SB, Long MW. Estimation of Eating Disorders Prevalence by Age and Associations With Mortality in a Simulated Nationally Representative US Cohort. JAMA Netw Open. 2019 Oct 9;2(10):e1912925.
- Dooley-Hash S, Adams M, Walton MA, Blow FC, Cunningham RM. The prevalence and correlates of eating disorders in adult emergency department patients. Int J Eat Disord. 2019 Nov;52(11):1281–90.
- Dooley-Hash S, Lipson SK, Walton MA, Cunningham RM. Increased emergency department use by adolescents and young adults with eating disorders. Int J Eat Disord. 2013 May;46(4):308–15.
- Mitchell JE, Peterson CB. Anorexia Nervosa. N Engl J Med. 2020 Apr 2;382(14):1343–51.
- Trent SA, Moreira ME, Colwell CB, Mehler PS. ED management of patients with eating disorders. The American Journal of Emergency Medicine. 2013 May 1;31(5):859–65.
- Kutz AM, Marsh AG, Gunderson CG, Maguen S, Masheb RM. Eating Disorder Screening: a Systematic Review and Meta-analysis of Diagnostic Test Characteristics of the SCOFF. J Gen Intern Med. 2020 Mar;35(3):885–93.
- Perry L, Morgan J, Reid F, Brunton J, O’Brien A, Luck A, et al. Screening for symptoms of eating disorders: reliability of the SCOFF screening tool with written compared to oral delivery. Int J Eat Disord. 2002 Dec;32(4):466–72.
- Voderholzer U, Haas V, Correll CU, Körner T. Medical management of eating disorders: an update. Current Opinion in Psychiatry. 2020 Nov;33(6):542–53.
- Spaulding-Barclay MA, Stern J, Mehler PS. Cardiac changes in anorexia nervosa. Cardiology in the Young. 2016 Apr;26(4):623–8.
- Giovinazzo S, Sukkar SG, Rosa GM, Zappi A, Bezante GP, Balbi M, et al. Anorexia nervosa and heart disease: a systematic review. Eat Weight Disord. 2019 Apr 1;24(2):199–207.
- Smythe J, Colebourn C, Prisco L, Petrinic T, Leeson P. Cardiac abnormalities identified with echocardiography in anorexia nervosa: systematic review and meta-analysis. The British Journal of Psychiatry. undefined/ed;1–10.
- Krantz MJ, Blalock DV, Tanganyika K, Farasat M, McBride J, Mehler PS. Is QTc-Interval Prolongation an Inherent Feature of Eating Disorders? A Cohort Study. The American Journal of Medicine. 2020 Sep 1;133(9):1088-1094.e1.
- Cass K, McGuire C, Bjork I, Sobotka N, Walsh K, Mehler PS. Medical Complications of Anorexia Nervosa. Psychosomatics. 2020 Nov 1;61(6):625–31.
- Norris ML, Harrison ME, Isserlin L, Robinson A, Feder S, Sampson M. Gastrointestinal complications associated with anorexia nervosa: A systematic review. International Journal of Eating Disorders. 2016;49(3):216–37.
- Santonicola A, Gagliardi M, Guarino MPL, Siniscalchi M, Ciacci C, Iovino P. Eating Disorders and Gastrointestinal Diseases. Nutrients [Internet]. 2019 Dec 12 [cited 2021 Feb 1];11(12). Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6950592/
- Calugi S, Miniati M, Milanese C, Sartirana M, El Ghoch M, Dalle Grave R. The Starvation Symptom Inventory: Development and Psychometric Properties. Nutrients. 2017 Sep 1;9(9).
- Sevinç TT, Kalaci A, Doğramaci Y, Yanat AN. Bilateral superficial peroneal nerve entrapment secondary to anorexia nervosa: a case report. J Brachial Plex Peripher Nerve Inj. 2008 Apr 27;3:12.
- Robinson L, Micali N, Misra M. Eating Disorders and Bone Metabolism in Women. Curr Opin Pediatr. 2017 Aug;29(4):488–96.
- Silva JSV da, Seres DS, Sabino K, Adams SC, Berdahl GJ, Citty SW, et al. ASPEN Consensus Recommendations for Refeeding Syndrome. Nutrition in Clinical Practice. 2020;35(2):178–95.
- Garber AK, Cheng J, Accurso EC, Adams SH, Buckelew SM, Kapphahn CJ, et al. Short-term Outcomes of the Study of Refeeding to Optimize Inpatient Gains for Patients With Anorexia Nervosa: A Multicenter Randomized Clinical Trial. JAMA Pediatrics. 2021 Jan 1;175(1):19–27.
- Queensland Eating Disorder Service. A guide to admission and inpatient treatment for people with eating disorders in Queensland [Internet]. Queensland Eating Disorder Service; 2020 [cited 2020 Feb 2]. Available from: https://metronorth.health.qld.gov.au/rbwh/wp-content/uploads/sites/2/2017/07/guide-to-admission-and-inpatient-treatment-eating-disorder.pdf
- Farasat M, Watters A, Bendelow T, Schuller J, Mehler P, Krantz M. Long‐term cardiac arrhythmia and chronotropic evaluation in patients with severe anorexia nervosa (LACE‐AN): A pilot study. Journal of Cardiovascular Electrophysiology. 2020. 31(2), 432-439. doi: 10.1111/jce.14338

