
Patient complaints are common in medicine. Emergency medicine (EM) in particular has some of the highest numbers of complaints, just behind obstetrics and surgery. Almost all of you reading this have probably been subject to some sort of complaint, and if it hasn’t happened yet, then it likely will. It is impossible to satisfy everyone, and when you encounter a vast and diverse population, a complaint become inevitable. Many of these complaints may seem frivolous to you, but there is massive overlap between situations that lead to complaints and patient safety. This post will mostly focus on complaints where peer review was critical of the care provided for various reasons, because this is how we can make meaningful changes to protect ourselves from complaints and improve patient care.
What is really important to keep in mind through this post is that patient concerns and College investigations reflect a very small proportion of actual patient safety incidents overall. The numbers you will see are really there to provide the common themes, but it’s safe to assume they astronomically underestimate all of these events.
The Patient Complaints Landscape
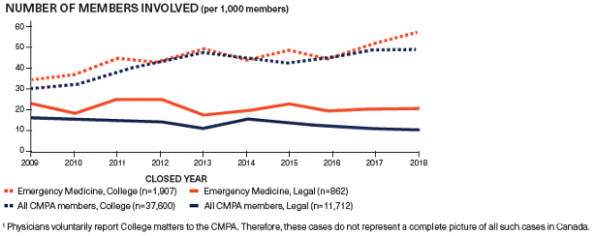
Complaints are on the rise across all specialties1. In 2016, the Canadian Medical Protective Association (CMPA) received 3,379 requests. In 2020, that number climbed to 4,045, an increase of 20%2. Another CMPA study found that 17% of physicians received a college complaint within 10 years of writing the now defunct MCCQE23.
Even more concerning, looking at cases closed between 2012-2016 against EM physicians where the CMPA was involved, less than 60% of the cases had a “favourable outcome” for the physician4. You’re probably wondering what a favourable vs unfavourable result is according to the CMPA. Dr. Lisa Calder of the CMPA defines the terms for us as follows:
“Unfavourable outcomes for members for civil legal actions include trials won by plaintiff, members convicted and trials settled in favour of a plaintiff. Unfavourable outcomes for members with college and hospital complaints include cases dismissed with concern, revoking of license, limitation on license, suspension of license and voluntary resignation/retirement.”
The COVID-19 pandemic has been difficult on everyone. It has also affected complaint numbers. Locally we have seen a rise of hospital complaints when comparing pre- and post-COVID data, with complaints rising approximately 20% between the year leading up to COVID and the first year of COVID5.
So, we know that complaints are on the rise in medicine as a whole, and EM is no different. EM also has some of the highest numbers of complaints of any specialty, and COVID did not help our cause. Now that we have discussed the landscape a little bit, let’s discuss the complaints process.
The Complaints Process
In order to discuss the hospital complaints process, we first need to review the basis for this process in Ontario: The Excellent Care for all act of 20106. This piece of Ontario legislation was developed in order to increase focus and accountability for delivering high quality patient care. It consists of the development of a quality committee in order to recommend improvement initiatives, translate best practice info, and develop annual QI plans. The legislation also mandates the establishment of a patient relations process with specific resolution timeline goals, the development of a patient declaration of values, yearly reviews, and ombudsman oversight. All Ontario hospitals must follow the mandated process for dealing with hospital complaints. Should a patient be unsatisfied with the hospital response, they may choose to bring their concerns to the office of the ombudsman or submit a complaint to the College.
We can’t discuss College complaints without first introducing the CMPA. they are a not-for-profit defence association that provides medico-legal advise and assistance, patient compensation, resources for risk management and also write opinions for medico-legal public policy7. In the case of a complaint the CMPA will advise on how to proceed through each step of your complaint process. Should you require, they may also provide you with legal counsel.
The College complaints process is long. In Ontario, The College of Physicians and Surgeons of Ontario (CPSO) estimates that a complaint investigation takes between 3 and 10 months, followed by a 2-3 month decision period. Together, people subject to a complaint can be looking at a 6-12 month process. If you do receive a complaint, you will be notified either through email, mail or phone. The College often supplies the complaint letter, though they may just enumerate the complaints listed within it. Physicians who receive a complaint should contact the CMPA PRIOR to opening the patient chart, especially if the record belongs to the hospital or another institution.
Once you do gain access to the patient chart it is critical that you never alter the patient record. You can have a conversation with the CMPA about whether it is appropriate to add information, though this may impact your credibility. You should also confirm what the College wants from you and observe their stated timelines8.
Next, you need to craft a response with CMPA guidance. The response should be respectful in tone, factual and objective. You should avoid defensiveness or anger. The letter should also consider the key issues in the complaints and reflect on mitigation strategies for the future as needed. From here the College will conduct their investigation, which may involve interviewing witnesses and seeking expert opinion. Once concluded, they will come to a decision. They will decide whether this complaints requires any action at all, a caution, a recommendation of remedial action, or to be sent to the disciplinary committee.
Patient Complaints: Where do they originate?
There are a variety of reasons a patient may choose to lodge a complaint against a physician. About 54% of College complaints involve cases where patient harm occurred9. Focusing in on cases where patients were harmed, a CMPA report of cases closed between 2012 and 2016 revealed that 72% of cases involved deficiencies in decision making. The majority of those involved inadequate assessments or incomplete investigations.
A further 22% of cases involved inadequate situational awareness as a contributing factor: inadequate monitoring, poor test follow-up, premature discharge, and failure to adequately read the medical chart. 26% of cases also involved an element of communication breakdown, either between physician and patient, inter-physician, physician to other provider or in respect to documentation10. What makes communication breakdown so critical is that not only is it the most easily modifiable target, it also does not simply affect patient perceptions of the interaction. Poor communication in the cases we just discussed led to negative effects on physician decision making 63% of the time and contributed to a lack of physician situational awareness 29% of the time. The other major reason to care about communication is that College complaint cases with communication issues ended in an 84% unfavourable outcome rate.
Handovers in particular are a major problem in emergency medicine. There are studies showing significant omissions or even incorrect data being handed over leading to longer handovers, increased length of stay, sub optimal care and negative impacts on the physicians themselves11,12. This was previously discussed in more detail in another EMOttawa Blog post on checklists in the ED. Kwok et al., published a QI report on introducing a handover tool that we will discuss briefly later, where they noted upwards of 1/4 of active patients and 1/2 of referred patient weren’t being handed over prior to their handover framework intervention13.
To summarize, the main drivers of complaint are as follows:
-
-
- Clinical Decision Making
- Inadequate assessments, investigations and treatment leading to misdiagnosis, a missed diagnosis or delay in diagnosis.
- Situational Awareness
- Inadequate monitoring of the patient’s condition, inadequate follow-up management, not appreciating the severity of a patient’s status, and premature discharge from the ED
- Communication Breakdown
- Poor handovers and coordination of care, not fully considering the patient’s or family’s concerns, issues with consent, and inadequate discharge instructions
- Clinical Decision Making
-
Avoiding Patient Complaints
Now let’s talk about strategies and best practices to reduce complaints. You probably noticed that the majority of the cases include clinical decision making as a factor in the complaint. Unfortunately, this is not an area that is easy to target for improvement. We are all human. We all have finite knowledge and will make errors. But as mentioned earlier, communication errors are associated with diagnostic errors and loss of situational awareness. By targeting our communication errors we can reduce our personal risk of patient complaint and improve patient safety.
In terms of physician-to-physician communication, let us focus on handover specifically. It has been established that handover is an area of communication where breakdowns occur and can cause patient harm. Luckily Kwok et al. have created a handover framework to correct these issues resulting in nearly a doubling in adequate handovers at our centre13. The ED-VITALS framework is an excellent way to improve patient safety and has been fairly well adopted by our department. I would encourage everyone who does not consistently employ structured handover notes to strongly consider using this framework on every handover in order to reduce your complaint risk and improve patient safety in the process.
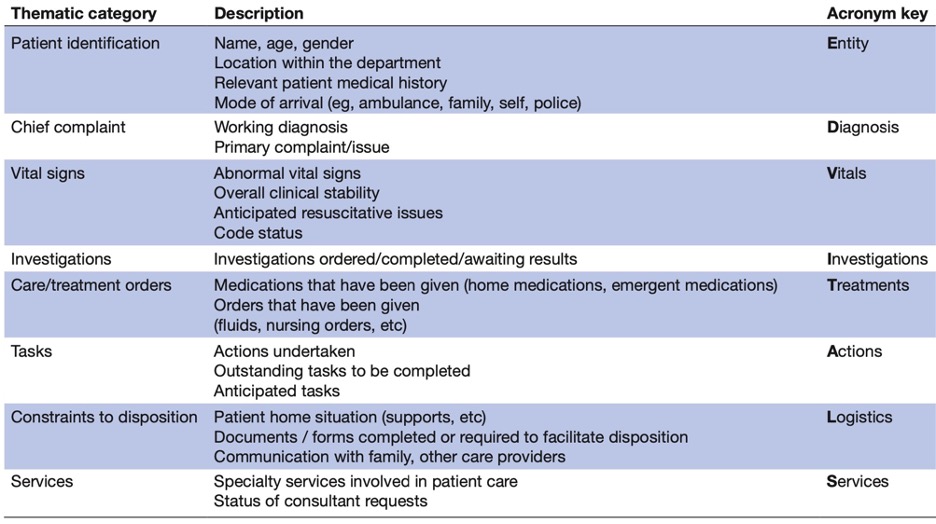
It is particularly important to pay attention to the often omitted parts of the framework, i.e. the “Logistics” component, as these disposition constraints greatly affect the patient’s perceptions of our care.
There is a lot to unpack with our interactions with patients. Let’s focus on discussing abnormal results, disclosing adverse vents, discharge instructions, consent, documentation and sensitivity.
Abnormal and Incidental Findings
Generally speaking, we are good at discussing important abnormal results. It may also be important to discuss any “abnormal” results (i.e. outside the reference range) that we do not find particularly concerning. This is particularly important if the patient receives a copy of their results (i.e. EMR). Reassurance that you’ve seen those “red” results and feel they are not an issue is important to some patients. It is also critical that you address incidental findings with patients and recommend a plan for follow-up14. This may be something as simple as “We found a little spot in your thyroid that doesn’t look dangerous. I would recommend you follow-up with your GP and get an US of the thyroid in around 6 months time.”
Disclosing Error
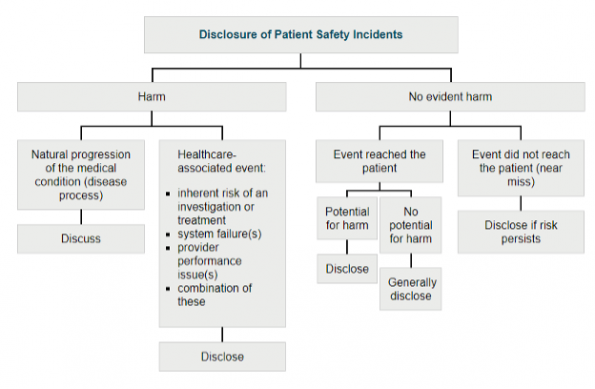
As you can see from the graph from the CMPA below,15 you need to disclose all patient safety incidents where harm occurs or where the event reached the patient, especially if there was potential for harm. If a non-harmful event reached the patient, even if there was no potential for harm it may still be advisable to disclose the error, as this can promote better physician-patient trust. You also need to disclose if the risk of this incident is ongoing. An example of an event without harm where the event did not reach the patient, but where the risk still persists would be the following: two middle age male patients with the name “Jim Smith” in the ED at the same time. Let’s say a medication was ordered on the wrong one, but was caught by your wonderful nurse prior to it being brought to the patient and no harm occurs. In this case it is fairly reasonable to foresee the potential of this recurring and it would be prudent to inform the patient.
This is a good time to add an important note about apologizing. An apology in the form of an expression of regret is really important for the emotional healing process. An example of this is “I’m sorry this happened to you”. Further apology depends on what exactly happened in the incident. I would suggest consulting the CMPA website for further info or to speak to a physician advisor if you have concerns about an incident. This type of apology will not put you in any legal jeopardy. In Ontario, and many other provinces in Canada, an expression of regret is not an admission of fault legally. In Ontario this is due to the Apology Act of 200916.
Discharge Instructions
Discharge instructions are a critical part of the patient interaction and leave a final impression with each patient. Your instructions should include signs and symptoms that should prompt further medical care, specific advice regarding their condition, who to follow up with and when, and they are always welcome to return if needed17. You should also ensure that the patient understood your instructions and that you document everything you discussed. Copies of the chart should be sent to the GP as well as any specialist you instruct the patient to follow up with. Handouts are a nice supplement but do not replace verbal instructions.
Consent
Decades ago, the Supreme Court of Canada ruled that patients should be told what the doctor intends to do, what the significant material risks are, as well as anything else that a reasonable person in that patient’s condition would want to be told. This is in essence informed consent. Briefly, the components of consent are that it must be voluntary, the patient needs to be capable and that they must be properly informed18. Generally, providers get into trouble when either no attempt at consent was made (which can lead to allegations of battery), or the informed component of the consent was lacking. It’s critical to discuss the diagnosis, proposed treatment, alternatives and risks, success rate and consequences fo refusal of treatment.
Documentation
We won’t really discuss standard history and physical note documentation here, as most of us have at least a reasonable understanding of what to document for an ED visit. In brief, you must list the patients presenting complaint, pertinent positives and negatives, past medical history, exam, important investigation findings, impression and plan. I want to instead draw your attention to documentation of procedures. Proper documentation is critical from a medico-legal point of view.
You need the following components in your procedure note:
-
-
- Type of Procedure
- Who performed it
- Indication
- Consent with the listed aspects discussed
- The procedure itself
- Complications
- Follow-up care plan
-
Just jotting down a couple of vague lines within your note is insufficient documentation and leaves you open to significant risk.
EMR templates are a double-edged sword for procedure notes. They can really help save time, and can sometimes be a forcing function to help you remember to fill out specific aspects of the note. This comes at a risk of transcribing errors into the chart especially if you employ smart phrases that pre-populate normal findings, ultimately possibly patient’s at risk19. Similarly, inaccurate information can potentially harm the validity of your notes medico-legally, though I am not currently aware of a case where a judgement on this has been made. Use them at your own risk and I strongly encourage you to consider avoiding pre-populated exam templates.
Sensitivity
Physicians are expected to deliver patient-centred care. The patient comes in because they have a concern. Even if we know that is concern is not something worrying to us, it doesn’t change their feelings about it. We need to acknowledge their concerns and address them properly. One way to do this is validate their decision to come to the emergency department. Some people do this by thanking patients for coming in that day. Empathy and understanding are powerful tools that we must use with our patients. Part of patient-centred care in Canada is also embracing the multicultural aspect of our country. It is critical to deliver culturally appropriate care for our patients20. This is a key patient safety issue. Now more than ever it is our responsibility to gain understanding of other people’s culture as part of our role as physicians.
Coping with a Patient Complaint
I want to leave you with a short discussion on the emotional effects of a complaint on the physician. College complaints are lengthy and cause significant emotional symptoms, such as anxiety, self-doubt, anger, helplessness, and lack of trust in patients. People also describe rumination on the case, social withdrawal, substance abuse, and work disruption, as well as physical symptoms like insomnia, and exhaustion. It is extremely understandable to struggle in these situations. If you find yourself in this situation there are things you can do, to manage the stress of a complaint including self-care (i.e. regular exercise or mindfulness). There are also cognitive strategies you can employ to help manage these stressful times.
-
-
- “Best Friend Strategy” – treat yourself the way you would treat a best friend in your situation
- Set limits on the amount of time you spend on a complaint
- Reflect on the event as an opportunity to grow as part of your growth mindset
- Acknowledge your biases
- Review your knowledge base.
-
You can also seek out personal support through a “failure friend”21 or get professional support. Most universities and hospitals have faculty and staff wellness programs that you can reach out to for ongoing support.
Here are a few resources that you can refer to if you need:
-
-
- Ontario Medical Association Physician Health Program: 1-800-851-6606
- CMPA – Managing Stress
-
Summary
-
-
- Complaints are on the rise in medicine and the ED is a common site of complaint;
- College complaints can be long and arduous, but the CMPA is there to help;
- Clinical care issues are the most common reason for complaint but communication breakdowns are key;
- Poor communication leads to poor perceptions of care, poor decision and loss of situational awareness;
- Handover frameworks reduce omissions and false information propagation;
- Clear discharge instructions are key to patient safety and satisfaction;
- EMR pre-populated templates increase speed at expense of accuracy and potential for harm;
- Empathetic and culturally-appropriate care is good patient care.
-
References
-
- CMPA MEDICAL-LEGAL RISK OVERVIEW Emergency Medicine. May 2019
- College complaints on the rise: Better communication can help. https://www.cmpa-acpm.ca/en/advice-publications/browse-articles/2018/college-complaints-on-the-rise-better-communication-can-help. Accessed June 15, 2021.
- Tamblyn R, Abrahamowicz M, Dauphinee D, et al. Physician Scores on a National Clinical Skills Examination as Predictors of Complaints to Medical Regulatory Authorities. JAMA. 2007;298(9):993. doi:10.1001/jama.298.9.993.
- CMPA Brief Report: Emergency Medicine – Ontario and Canada, June 2018
- TOH Patient Relations Stats presentation. Emergency Medicine Program / Service Line. May 2021
- Government of Ontario, Ministry of Health and Long-Term Care. Excellent Care For All – Health Care Professionals – MOHLTC. https://www.health.gov.on.ca/en/pro/programs/ecfa/legislation/act.aspx. Accessed June 15, 2021.
- About the CMPA. CMPA. https://www.cmpa-acpm.ca/en/about. Accessed June 15, 2021.
- What to do if you’re notified of a College complaint. https://www.cmpa-acpm.ca/en/advice-publications/browse-articles/2018/what-to-do-if-you-re-notified-of-a-college-complaint. Accessed June 15, 2021.
- CMPA brief report: Emergency Medicine – Ontario and Canada, June 2018
- CMPA Brief Report: Communication issues in the emergency department, May 2018
- Ye K, McD Taylor D, Knott JC, Dent A, MacBean CE. Handover in the emergency department: Deficiencies and adverse effects. Emergency Medicine Australasia. 2007;19(5):433-441. doi:10.1111/j.1742-6723.2007.00984.x.
- Maughan BC, Lei L, Cydulka RK. ED handoffs: observed practices and communication errors. The American Journal of Emergency Medicine. 2011;29(5):502-511. doi:10.1016/j.ajem.2009.12.004.
- Kwok ES, Clapham G, White S, Austin M, Calder LA. Development and implementation of a standardised emergency department intershift handover tool to improve physician communication. BMJ Open Quality. 2020;9(1). doi:10.1136/bmjoq-2019-000780.
- Physician-patient: Test result follow-up: Good Practice Guidance. https://www.cmpa-acpm.ca/en/education-events/good-practices/physician-patient/test-results-follow-up. Accessed June 15, 2021.
- Physician-patient: disclosure: CMPA Good Practices Guidance. https://www.cmpa-acpm.ca/en/education-events/good-practices/physician-patient/disclosure-of-patient-safety-incidents. Accessed June 15, 2021.
- Apology Act, 2009. Ontario.ca. https://www.ontario.ca/laws/statute/09a03. Published November 19, 2018. Accessed June 15, 2021.
- Informed discharge. CMPA Good Practices Guide – What patients need to know. https://www.cmpa-acpm.ca/serve/docs/ela/goodpracticesguide/pages/communication/Informed_Discharge/what_patients_need_to_know-e.html. Accessed June 15, 2021.
- Informed consent. CMPA Good Practices Guide – Informed consent. https://www.cmpa-acpm.ca/serve/docs/ela/goodpracticesguide/pages/communication/Informed_Consent/informed_consent-e.html. Accessed June 15, 2021.
- Cultural safety. CMPA Good Practices Guide – Respecting difference and diversity. https://www.cmpa-acpm.ca/serve/docs/ela/goodpracticesguide/pages/professionalism/Cultural_safety/respecting_difference_and_diversity-e.html. Accessed June 15, 2021.
- Medical Records Documentation. CPSO. https://www.cpso.on.ca/Physicians/Policies-Guidance/Policies/Medical-Records-Documentation#endnote09. Accessed June 15, 2021.
- Gray S, A FeminEM in NYC – Reflections from #FIX18 Part One • St Emlyn’s. Fail Better with a Failure Friend. FemInEM. https://feminem.org/2017/12/05/fail-better-failure-friend/. Published August 27, 2019. Accessed June 15, 2021.


Excellent overview and outline of key takeaways . Congratulations!