

We are back with Part-2 of our blog series on Palliative Care in the ED. If you haven’t already check-out Part 1 HERE. In this series, we will delve into the subject further by exploring the following topics:
-
- Screening Tools: The Old and the New
- Education and Integration of Palliative Care Medicine in the ED
“I Screen, You Screen!” : Screening tools for the identification of patients requiring palliative referral
When you think of your regular run of the mill ED shift, many of them have chronic diseases as identified in Part 1. So who requires palliative care? Are we to screen every single person? The answer, is no. What we propose is to consider further prompting/screening by hand-picking patients that tickle your “spidey senses”. This next section will focus on some simple tools that can be used on shift to help streamline and consolidate the decision to refer to palliative care services.
Surprise Question (SQ) and Double-Surprise Question (DSQ)
Many of you may have already heard of the “Surprise Question”:
Would I be surprised if my patient died in the next 12 months?
The SQ was developed by Dr. Joanne Lynn in 2005 to help identify patients who might benefit from PC services. However, in 2017 Dr. James Downar, an intensivist, and PC specialist at The Ottawa Hospital conducted a systematic review to assess the SQ’s efficacy. He found that it performed rather poorly, with a sensitivity (Sn) and specificity (Sp) of 67% and 80%, respectively. Pushing the point further, he found that it performed particularly poorly among patients with non-malignant illnesses.7
Ouchi and colleagues also evaluated the SQ in 2018 and 2019. They narrowed the scope of the question, in an effort to improve the Sn and Sp.
-
- In 2018, they had individuals ask the same question, with a12-month timeline but adjusted the age group to ≥65 years. This adjustment yielded a Sn of 77% and Sp of 56%.15
- In 2019, they the question was changed to address a 1 month timeline. Unfortunately, no notable improvements were made; the Sn and Sp were 43% and 82%, respectively.16
- Overall, they concluded that the Surprise Question doesn’t perform well and isn’t much better than baseline physician gestalt.
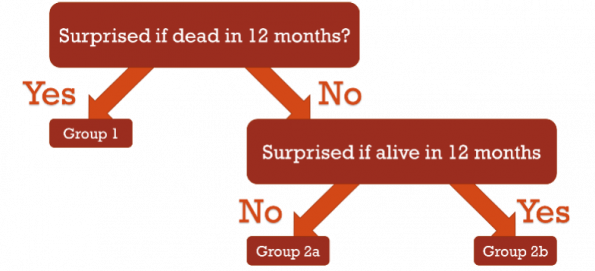 A Dutch team, led by Ermers in 2021, put a new spin on the question by first positing the SQ, followed by its inverse; “Would I be surprised if my patient was alive in the next 12 months?”. They created the Double Surprise Question,8 in an effort to create a 3-tier stratification of patients, allowing for greater prognostication. If the clinician answered ‘yes’ to the SQ, they would be included in Group 1. If they answered ‘no’, the clinician would then pose the inverse question and, depending on the answer, they would be split into either Group 2a or 2b (see the flow chart to the R side).
A Dutch team, led by Ermers in 2021, put a new spin on the question by first positing the SQ, followed by its inverse; “Would I be surprised if my patient was alive in the next 12 months?”. They created the Double Surprise Question,8 in an effort to create a 3-tier stratification of patients, allowing for greater prognostication. If the clinician answered ‘yes’ to the SQ, they would be included in Group 1. If they answered ‘no’, the clinician would then pose the inverse question and, depending on the answer, they would be split into either Group 2a or 2b (see the flow chart to the R side).
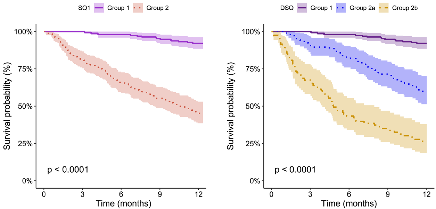 How did the Double Surprise Question fair? Did positing that second question have an effect?
How did the Double Surprise Question fair? Did positing that second question have an effect?
-
- Specificity: Sp (67.7% →6%) and positive predictive value (PPV) (54.8% → 73.5%) were improved.
- Sensitivity: Unfortunately, the cost was a drop in Sn (87.3% → 7%) and negative predictive value (NPV) (92.1% → 80.7%).
- The paper also only assessed patients with oncologic disease. Ergo, the DSQ is an average question to identify those with cancer who are likely to survive, but not for those you suspect may die and may not be applicable in non-malignant populations.
General Recommendation: Use caution when using the SQ or DSQ in the ED, and consider only referring those in Group 2b, so long as clinical metrics align.
P-CaRES
The Palliative Care and Rapid Emergency Screening tool (P-CaRES), was developed by Bowman et al.9
- A tool designed specifically to help the Emergency physician identify patients who might benefit from PC referral in the ED.
- It comprises a two-stage screening process:
- Step 1: Identification of a life-limiting illness (see Figure 1).
- Step 2: Identify unmet PC needs (see Figure 2). These include ≥2 ED visits in 6 months, uncontrolled symptoms, functional decline, goals of care (GOC) uncertainty or caregiver burnout, and the Surprise Question.
- 541 ED providers were asked to apply the tool across 3-5 clinical vignettes and were able to identify patients who would benefit from PC services with 89% accuracy as verified by PC consultants.
- Not only does the tool boast a Sn of 93% but >80% of the participating clinicians reported ease of use, usefulness, and of benefit to patient care.
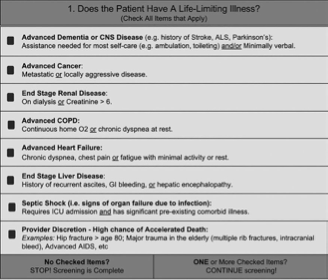
Figure 1: Identification of an individual with a life-limiting illness.
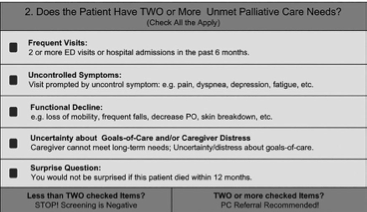
Figure 2: Identification of unmet PC needs.
Support-ED
Support-ED is a helpful screening tool currently being developed under the Primary Palliative Care for Emergency Medicine initiative spearheaded by New York University ED physician and researcher, Corita Grudzen. Support-ED is a novel, EMR based (Epic in this case), PC screening tool that is modelled after the P-CaRES criteria. It comprises automated notifications based on algorithmic data collected from several metrics in the patient’s chart , and inputed by healthcare professionals as outlined in the paper by Tan et al.10 These automated notifications are triggered immediately for nurses at triage and within a 1-hour time delay for physicians, allowing plenty of time for an initial assessment.
Notifications are based on the three following EMR criteria:
-
- Does the patient have an active eMOLST (DNR)?
- Has the patient previously been referred/enrolled with hospice services?
- Does the patient have a serious life-limiting illness (based on algorithmic criteria)?
- E.g., diminished function based on ECOG score, GFR < 15, pCO2 > 70 mmHg, or HCO3- < 10 mEq/L
If any of these alerts are triggered, the physician is asked two follow up questions:
-
- Do you think this patient may die during THIS hospitalization?
- Do they have any one of the following?
- Worsening functional status
- Uncontrolled symptoms due to life-limiting illness?
- Unclear goals of care?
If the answer is yes to any of the above questions, the physician/nurse is prompted to contact social work and/or palliative care services. Although Support-ED is still under development, the prospect of automated triggers based on complex algorithms does potentially alleviate some of the inertia inherent to checklists. To play devil’s advocate, EMR pop-ups also are often overlooked, however, if simplified and triggered in the right context, they could prove extremely useful with buy-in by both social work and available palliative services at respective hospital sites.
Take-Home Points
-
- The SQ performs poorly; the DSQ improves on prognostication;
- P-CaRES is a validated PC screening tool easily and effectively employed by the ED physician;
- Support-ED has the potential to be an effective ED tool for EPs using EMRs; regional/local validation is pending.
Palliative care-Education and Integration in the ED
In 2019, Baylis et al conducted a survey of all the RCPSC-EM and CCFP-EM programs across Canada and found that only 38.5% had a structures PC and end of life (EOL) curriculum.11 Of those that did have an integrated program, 100% were based on 4 hours of lectures/seminars and a single PC rotation was mandatory in only 1 of 26 programs, 4 offered a selective, and 13 offered electives. The lectures focused largely on goals of care, breaking bad news, and ethics/legal issues and placed the least emphasis on grief and bereavement, death trajectories, and prognostication.
if we want to engender a true ED-PC culture in our hospitals, dedicated PC rotations, simulation sessions, and an accessible area of focused competence (AFC) or fellowship for EM residents is necessary. To expand on the last aspect, the American Board of Emergency Medicine (ABEM) has had a subspecialty in PC available to EM physicians since 2006, whereas the Royal College of Physicians and Surgeons Canada currently only have a 2-year program target at specialists in internal medicine, neurology, or anesthesiology. Alternatively, there is a 1-year program targeted at family medicine specialists. This acts as a barrier for entry of EM residents with a special interest in PC as they have little hope of true accreditation in the field. Without specialists, the field has a small opportunity for growth.
In the US, Dr. Grudzen’s PRIM-ER initiative is seeking to ensure that more EM providers are educated in the field.12 Her initiative comprises 4 facets and are driven by patient and QI centered outcomes:
-
- Multidisciplinary primary palliative care education for EPs, NPs, and PAs (two 1-hour lectures).
- Simulation-based workshops for EPs, NPs, and PAs (4-hour in-person workshop).
- Clinical decision support by the Support-ED screening tool.
- Provider audit and feedback through weekly individualized reports.
Qualitative analysis has been performed at 2 of 35 proposed sites in the US. Among the 79% and 92% uptake at sites 1 and 2, respectively, participants reported that both a strong QI presence and buy-in from hospital leadership resulted in the successful integration of this educational program.13 Results of patient-centered outcomes are currently unavailable due to ongoing data collection, however, their publication is anticipated to occur in the next 1-2 years.
Take-Home Points
-
- Resident ED-PC education exists but needs expansion;
- More ED-PC dual-certified staff required;
- PRIM-ER is a viable intervention for Canadian institutions to improve care for those at EOL.
Summary – Final Take Home Points
I hope that this 2-Part blogpost series has provided perspective to the reader as to the importance of ED-PC integration in the face of a growing elderly population. As ED physicians, we are often overburdened with the sheer volume and complexity of patient care on any given day but with further education and a culture shift that emphasizes the importance of preventing return ED visits and exceptional symptom control for this patient population, I believe that much of this could become second nature.
Just remember:
-
- There are currently inequities for Palliative Care services among patients at EOL with non-malignant disease;
- Symptom burden should be the main guide for care;
- Palliative Care involvement = fewer ED/ICU visits;
- P-CaRES and Support-ED are promising tools for future use in Canadian EDs;
- ED-PC education for residents and other EM providers needs advancement;
- An initiative like Grudzen’s PRIM-ER could bring us to the ED-PC integrated model we all need.
References
1. Statistics Canada. Leading causes of death, total population, by age group. Published November 26, 2020. https://www150.statcan.gc.ca/t1/tbl1/en/tv.action?pid=1310039401
2. Seow H, O’Leary E, Perez R, Tanuseputro P. Access to palliative care by disease trajectory: a population-based cohort of Ontario decedents. BMJ Open. 2018;8(4):e021147. doi:10.1136/bmjopen-2017-021147
3. Alicia Costante CL and CC. Access to Palliative Care in Canada. Healthc Q. 2019;21(4):10-12.
4. World Health Organization. Palliative Care. Published August 5, 2020. https://www.who.int/news-room/fact-sheets/detail/palliative-care
5. Canadian Society of Palliative Care Physicians. Palliative Care – Five Things Physicians and Patients Should Question. Choosing Wisely Canada. https://choosingwiselycanada.org/palliative-care/
6. Quinn KL, Stukel T, Stall NM, et al. Association between palliative care and healthcare outcomes among adults with terminal non-cancer illness: population based matched cohort study. BMJ. 2020;370:m2257. doi:10.1136/bmj.m2257
7. Downar J, Goldman R, Pinto R, Englesakis M, Adhikari NKJ. The “surprise question” for predicting death in seriously ill patients: a systematic review and meta-analysis. Can Med Assoc J. 2017;189(13):E484. doi:10.1503/cmaj.160775
8. Ermers DJ, Kuip EJ, Veldhoven C, et al. Timely identification of patients in need of palliative care using the Double Surprise Question: A prospective study on outpatients with cancer. Palliat Med. 2021;35(3):592-602. doi:10.1177/0269216320986720
9. Bowman J, George N, Barrett N, Anderson K, Dove-Maguire K, Baird J. Acceptability and Reliability of a Novel Palliative Care Screening Tool Among Emergency Department Providers. Acad Emerg Med. 2016;23(6):694-702. doi:10.1111/acem.12963
10. Tan A, Durbin M, Chung FR, et al. Design and implementation of a clinical decision support tool for primary palliative Care for Emergency Medicine (PRIM-ER). BMC Med Inform Decis Mak. 2020;20(1):13. doi:10.1186/s12911-020-1021-7
11. Baylis J, Harris DR, Chen C, et al. Palliative and end-of-life care education in Canadian emergency medicine residency programs: A national cross-sectional survey. CJEM. 2019;21(2):219-225. doi:10.1017/cem.2018.470
12. Grudzen CR, Brody AA, Chung FR, et al. Primary Palliative Care for Emergency Medicine (PRIM-ER): Protocol for a Pragmatic, Cluster-Randomised, Stepped Wedge Design to Test the Effectiveness of Primary Palliative Care Education, Training and Technical Support for Emergency Medicine. BMJ Open. 2019;9(7):e030099. doi:10.1136/bmjopen-2019-030099
13. Chung FR, Turecamo S, Cuthel AM, et al. Effectiveness and Reach of the Primary Palliative Care for Emergency Medicine (PRIM-ER) Pilot Study: a Qualitative Analysis. J Gen Intern Med. 2021;36(2):296-304. doi:10.1007/s11606-020-06302-2
14. Carter AJE, Arab M, Cameron C, et al. A national collaborative to spread and scale paramedics providing palliative care in Canada: Breaking down silos is essential to success. Prog Palliat Care. 2021;29(2):59-65. doi:10.1080/09699260.2020.1871173
15. Ouchi K, Jambaulikar G, George NR, Xu W, Obermeyer Z, Aaronson EL, Schuur JD, Schonberg MA, Tulsky JA, Block SD. The “Surprise Question” Asked of Emergency Physicians May Predict 12-Month Mortality among Older Emergency Department Patients. J Palliat Med. 2018 Feb;21(2):236-240. doi: 10.1089/jpm.2017.0192. Epub 2017 Aug 28. PMID: 28846475; PMCID: PMC6909689.
16. Ouchi K, Strout T, Haydar S, Baker O, Wang W, Bernacki R, Sudore R, Schuur JD, Schonberg MA, Block SD, Tulsky JA. Association of Emergency Clinicians’ Assessment of Mortality Risk With Actual 1-Month Mortality Among Older Adults Admitted to the Hospital. JAMA Netw Open. 2019 Sep 4;2(9):e1911139. doi: 10.1001/jamanetworkopen.2019.11139. Erratum in: JAMA Netw Open. 2020 Sep 1;3(9):e2020868. PMID: 31517962; PMCID: PMC6745053.



Good morning.
I work in the Emergency Department of the Central Hospital University Lisbon North, (FMUL), in which I’m performing my Master in Palliative Care.
The campaign of “Choosing Wisely” endorsed “timely engagement of palliative care services”, by using the TOOL (P- CaRES) is a very engaging question.
To widespread the adoption of this tool, in all emergency departments, for utterly the purposes it might be useful, it’s necessary the adequate translation and cultural adaptation.
My question is if there is any Portuguese translation (of Portugal, not Brazil), that can display the cultural reality of our European country?
I tried to contact Mrs. Naomi George, but i had no feedback at the time.
Could you please help me in this matter?
Did you gather to talk to her or her colleagues, in order to use the copyrights?
Thanks for your time!
Kind regards
Cristiana Rolão