

The United Nations (UN) defines human trafficking (HT) as “the recruitment, transport, transfer, harbouring, or receipt of a person by such means as threat or use of force or other forms of coercion, abduction, fraud, or deception for the purpose of exploitation“. HT is often referred to as a modern form of slavery, and can take place in one’s home country, during migration, or in a foreign state. HT has 3 core elements:
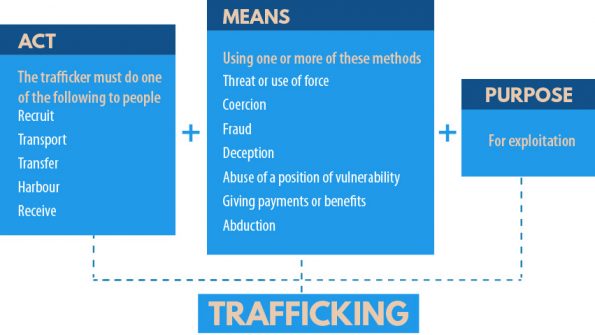
Figure 1 | The three core elements of HT. The purpose of HT is always exploitation. From the UN Office on Drugs and Crime.
HT is illegal in Canada, whether it occurs within or across Canadian borders. Both the Criminal Code (Section 279) and the Immigration and Refugee Protection Act (IRPA) have specific sections that address HT.
Types of Human Trafficking

Figure 2 | Types of HT. From the UN Office on Drugs and Crime.
Sex trafficking is the most common form encountered in healthcare settings. It includes all forms of facilitated and/or forced non-consensual sexual exploitation:
- Overt and hidden sex work (sexual services in settings like body houses, massage parlours, truck stops, etc.).
- Online audiovisual exploitation (webcam shows, sexting, message boards, pornography).
- Erotic dancing, stripping, sexual performances.
Sex trafficking is different from consensual sex work. Sex work by personal agency is a legitimate occupation and one’s choice to engage in this line of work is unique to that person. The distinction is choice and consent; sex trafficking is always exploitative.
Forced labour is another common form of human trafficking. Victims may be forced or coerced into working without pay or for a non-livable wage, often in fear of violence and in inhumane conditions. Common settings include factories, construction sites, the hospitality industry, and the agricultural sector.
Trafficking for organ trade more commonly occurs internationally. However, Canadians do travel to other countries, particularly lower-income and previously colonized countries, to receive organs from trafficked persons.
The scope of the problem
The hidden nature of trafficking renders it is impossible to precisely quantify. A host of barriers to seeking assistance from authorities results in under-reporting.
Barriers to reporting and seeking help
The dynamics of a trafficked person’s situation are nearly always complex. Barriers include:
- Fear of further abuse from their trafficker.
- Victims are often threatened and conditioned to conceal their situation. This becomes a very powerful deterrent to disclosure and seeking help.
- Fear of deportation.
- Fear of legal ramifications.
- Many victims of human trafficking are often involved in forced criminal activity.
- Lack of familiarity with the regional language.
- Lack of means to support leaving their current situation.
- Sense of shame, stigmatization, or humiliation about their situation.
- Lack of understanding of what trafficking is or do not identify as being trafficked.
- Often don’t see themselves as being victims or sometimes view their situation as only temporary.
- Fear of judgement or discrimination by health care providers and authorities.
Data reported through international organizations provide an incomplete view of the problem, however trends over the last 10-15 years are useful.
Global statistics:
- 40 million HT victims internationally (5.4 HT victims/1000 people).
- 71% of those trafficked are women or girls.
- 25% of those trafficked are under the age of 18.
Canadian statistics:
- 2468 police-reported HT incidents between 2009 – 2019, with a rising trend since.
- 33% of police-reported incidents involve the crossing of the Canadian border.
- 85% of police-reported incidents occur in major cities.
- 95% of trafficked persons are women or girls.
- 89% of trafficked persons are under the age of 35.
- 89% of victims know their trafficker.
- 65% of those accused of trafficking are men aged 18 – 34.
Trafficked persons in the ED
Lederer et al. interviewed 107 survivors of sex trafficking in the United States to explore health care access and symptoms experienced both during and after trafficking.They found that during their time of captivity:
- 88% sought treatment within the healthcare system but were neither identified as being trafficked nor offered assistance.
- 63% were seen in the ED.
- Within the ED, only 43% were asked something about their personal and social history and only 65% were assessed alone without their trafficker, which is critical to the identification process.
Identification of potential trafficked persons in the ED
Identification within the ED can be difficult for a number of reasons:
- There are no definitive signs or symptoms that reliably identify trafficked persons.
- There are no widely-employed screening tools.
However, there are risk factors for human trafficking, health consequences of being trafficked, and red flag features that you can ascertain during your assessment. It is the constellation of ALL of these together that should raise your suspicion.
Risk factors for HT
The origins of HT are very complex and influenced by economic, social, and cultural factors. Traffickers often exploit the desire to migrate due to poverty, political unrest, gender-based violence, or social instability.
The risk factors that predispose victims to all forms of trafficking can really be broken down into three main categories:
- Socioeconomic vulnerabilities:
- Poverty.
- Lack of formal education.
- Limited English proficiency.
- Food and housing insecurity.
- Limited support systems.
- Low income.
- Low self-esteem.
- History of violence or trauma:
- Early childhood abuse, trauma, or neglect.
- Prior physical, sexual, emotional, or domestic abuse.
- Past history of mental health disorder(s).
- Personal or family history of substance misuse or addiction.
- For children, exposure to the juvenile corrections system or foster care.
- Marginalized populations:
- Homeless youth.
- Members of the 2SLGBTQ+ community.
- Individuals with disabilities.
- Radicalized minorities, particularly Black and Indigenous women.
- Transient foreign migrant workers.
- Migrants or refugees displaced from conflict zones.
History and Physical Examination Features
Those being trafficked suffer a wide spectrum of both physical and psychological health consequences as a result of exposure to violence, restricted movement, and deprivation. Patients may present to the ED with a variety of complaints including:
- Sexual / reproductive health: recurrent or untreated STIs, requesting STI or pregnancy testing, PID, unintended pregnancy, spontaneous abortions, or requesting elective abortions (which may or may not be forced).
- Workplace related injuries due to dangerous working conditions, poor training or equipment, inadequate PPE, or exposure to chemical or physical dangers.
- Substance misuse or withdrawal.
- Mental health concerns.
- Traumatic injuries secondary to physical violence.
- Advanced disease states due to delay in seeking medical care.
A complete and thorough physical exam is important in order to identify any injuries. Documentation of physical findings should be objective, clear, and comprehensive.
- Injuries related to trauma or physical assault.
- Occupational injuries in the case of labour trafficking.
- Signs suggestive of neglect such as dehydration, malnutrition, and poor dentition.
- Tattoos or branding: victims are often coerced into getting tattooed as a way to signify that they belong to a certain trafficker. Such tattoos may include bar codes, crowns, and roses with initials and even currency, which may be money bags, coins, dollar bills, or currency symbols. Common tattoo locations linked to trafficking include the neck, arms, and above the groin area.

Figure 3 | Examples of tattoos that may be found on trafficked persons.
Red flags – history:
- History may be inconsistent.
- The story may change with repeated questioning.
- You illicit a history that sounds ‘scripted’.
- Injuries or physical exam may not match the reported mechanism.
Red flags – patient / situation:
- Patient may be inappropriately dressed or not dressed for the elements.
- Patient may be unsure of their location or report that they have moved recently.
- Discrepancy between suspected and reported age.
- Patient may lack access to identification, particularly if that documentation is being carried by another individual who is escorting them to the ED.
- The presence of a controlling person at the bedside:
- They may report that they are a family member, partner, or employer.
- This individual may dominate the conversation, answer questions on behalf of the patient, or may attempt to act as a translator.
- You may get a sense that the patient is unable to express themselves with that individual around.
What now? Ask more questions!
Once you start to suspect your patient may be trafficked based on your assessment, it is important to ask more questions with some key principles in mind.
- Interview your patient alone. This can be tricky, especially if there is a controlling individual at the bedside who refuses to leave. Try citing hospital policy, ordering a urine sample and walking your patient to the bathroom, or ordering imaging and escorting your patient to radiology.
- Privacy. Ensure as best as possible that you are in a private setting before proceeding with sensitive questions.
- Consent. Obtain consent and re-iterate policies and limits of confidentiality.
- Translation. Use a certified translator if a language barrier is present.
- Use direct, open-ended questions and be supportive of the patient’s right to not disclose.
- Remain cognizant of both verbal and non-verbal responses to questions.
While disclosure, rescue, and rehabilitation are the ideal outcomes of your encounter, the primary goal is to establish trust, facilitate empowerment, and provide a safer judgment-free space. Trafficked persons endure significant physical and psychological trauma, often manifesting in distrust of the healthcare system. Using a trauma-informed and patient-centered approach, we can create a safe clinical environment sensitive to their needs.
Trauma-informed care
- Approach that emphasizes that one’s behaviours are informed by traumatic experiences in their past.
- This model emerged ~20 years ago in the area of substance dependence and mental health, and has since evolved and been widely adopted by those working in intimate partner violence (IPV) and HT.
Wilson et al. consolidated the central tenants of IPV-specific trauma-informed practice into 6 core principles They can be applied to our approach to HT in the ED.
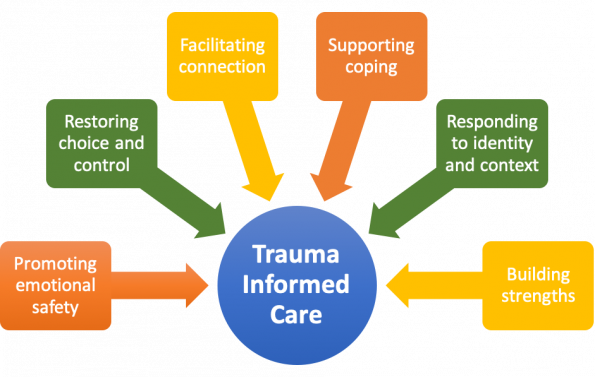
Figure 4 | The six principles of trauma-informed care, as defined by Wilson et al. (2015).
Patient-centred care
- Emphasizes the patient being central to the decision making process throughout all stages of care.
- A common feature of the trafficked experience is unpredictability and lack of control over one’s body / actions. Encourage your patient to participate in care decisions in the ED and take ownership in those decisions.
- Aims to prevent re-traumatization throughout the care process.
Screening questions
When it comes to the specific questions to ask, a number of screening tools have been developed to detect HT, but they take time and none have been validated in the ED.
Kaltiso et al. recently published a study of a novel HT screening tool in an urban adult ED. They developed an 11-item screening tool based on the review of existing tools and feedback from providers. Adult patients were screened based on high-risk chief complaints, ‘red flag’ risk factors, or provider impression. Healthcare providers including physicians, nurses, and nurse practitioners were trained to administer the questionnaire. A screen was considered positive if the patient answered yes to any one of the questions. Those who screened positive underwent a longer semi-structured interview with a social worker to further evaluate risk and determine the patient’s likely trafficking status.
In total, just under 27,000 ED patients were screened, 189 of which screened positive. 37 of those patients were confirmed to have a likely active sex trafficking status. Eight of these patients elected to go to a community partner safe house. Limitations of the study include:
- Questions were not specific for HT; many positive screens turned out to be cases of IPV.
- 61 of the patients screening positive had an unknown trafficking status, mostly due to incomplete documentation.
- While the screening tool was designed to assess both sex and labour trafficking, no patients endorsed labour trafficking.
- Potential unconscious bias; since trafficking primarily affects women, clinicians may have preferentially screened female patients.
While more research is required prior to widespread adoption of this tool, it does provide some insight into the types of questions we can be asking to screen our patients for human trafficking.
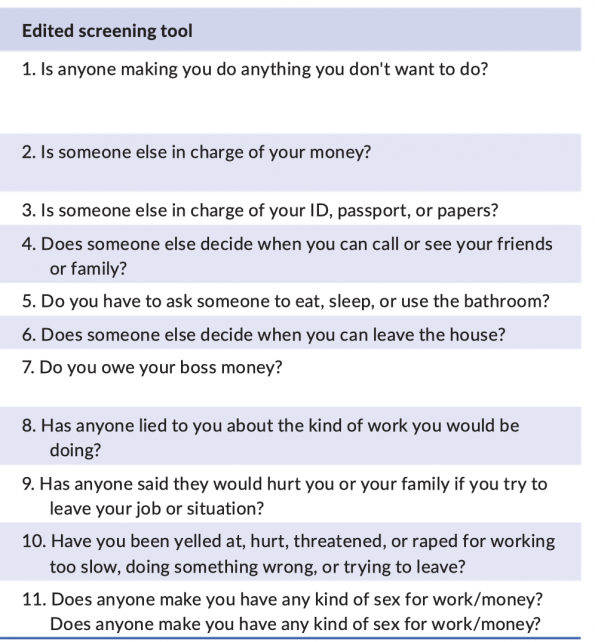
Figure 5 | 11-item screening tool for HT in adult EDs, as per Kaltiso et al. (2021).
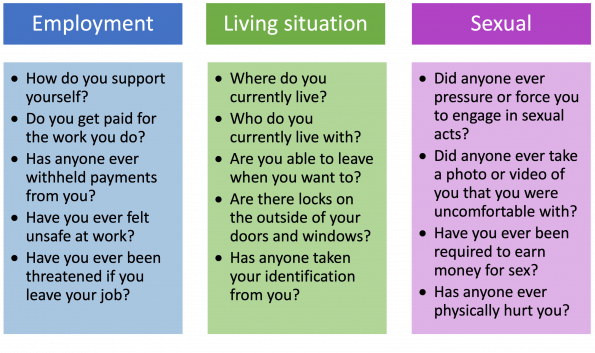
Figure 6 | Selected screening questions for HT in the ED.
Caring for trafficked persons in the ED – How can we help?
Interviews of HT survivors confirm they are often no prepared to leave their trafficker at the time they present to the ED. Our goals in the ED are to:
- Identify the patient’s medical, personal, and safety needs and ensure these are met.
- Consider social admission/referral to inpatient services, if permitted by the patient.
- Consider indications for mandatory reporting.
- Mobilize resources as approved by the patient.
Mandatory Reporting
In Canada, there are no mandatory reporting laws for HT. Do NOT contact the authorities without the patient’s consent. In Ontario, there are 2 notable exceptions:
- If a minor is involved (i.e., less than 16 years old) then we would be mandated to report to Children’s Aid Society (CAS). We strongly suggest consideration of CAS involvement for all patients under 18, however.
- If there is a gun shot wound, then you are mandated to report to the police.
Mandatory reporting laws do vary by jurisdiction so please ensure you are following your local policies.
Mobilizing Resources
Local resources vary depending on your location of practice. Engage your social work colleagues to assist in accessing these services. Personnel working at sexual assault and IPV programs are often trained to also care for trafficking victims, such as The Ottawa Hospital’s Sexual Assault and Partner Abuse Care Program (SAPACP). Assessments focus on addressing physical concerns, safety planning, harm reduction as well as personalized referrals to community resources. They can also arrange direct follow up with these patients
Ontario EDs each have an agreement with one of 37 sexual assault and IPV programs in the province. Information how to access your local program may be found HERE or by calling the 24/7 provincial Navigation Line: 1-855-NAV-SADV (628-7239).
Ottawa-specific resources:
- Ottawa Victim Services
- VoiceFound: a survivor-led Canadian charity that works to creat safe communities that recognize and stop abuse.
- The Clinic (though VoiceFound): provides healthcare and support for those who are at risk of, are experiencing, or have experienced HT
- YouTurn: community based counselling for youth and their families who are involved in HT.
References
