
Onboarding and transition to independent practice are challenging (1–3). New attending physicians need knowledge to function in novel roles (4), (Yeung, Cheung et al, personal communication) However, this knowledge is often tacit. By improving our understanding of the characteristics of tacit knowledge, we can ease the integration of new physicians.
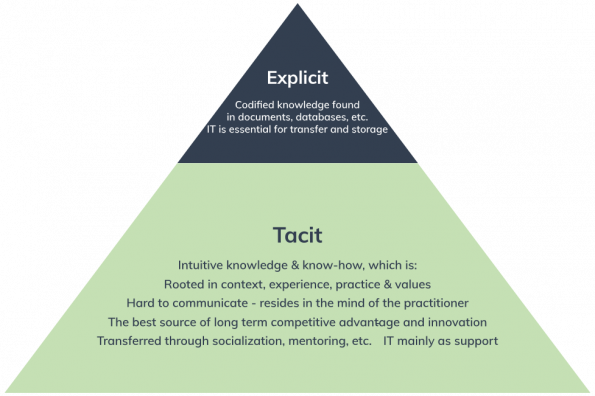
Image from: www.helpjuice.com
Objectives:
- List four important areas of tacit knowledge in Emergency Medicine practice
- Devise and implement strategies to integrate new physicians into a group practice
What did we do?
We conducted two studies to learn more.
Onboarding study
We offered a survey and interview to physicians who had onboarded at our academic department within three years. Most had simultaneously transitioned to practice. Six onboarding themes were developed: formal orientation and information, graduated responsibilities, mentorship, relationship building, workplace culture and structure, and strong emotions that overlaid all findings. Together with leadership, we developed and began to implement a new multifaceted onboarding program. Tacit knowledge formed a core aspect of several themes.
Tacit knowledge study:
Guided by constructivist grounded theory (5,6), we interviewed newly independent physicians about tacit knowledge acquired in early practice. We identified themes and generated two theories. For this Grand Rounds we will concentrate on the first theory.
What did we find?
Tacit knowledge is dynamic, nuanced, and difficult to transfer, but essential for independent practice. New attendings identified tacit knowledge in four main areas:
- Institutional processes
This includes processes within the department and the institution, local resources and norms of referral processes. Unwritten rules undermined the usefulness of written resources. New attendings needed skills to optimize practice efficiency. - Patient Interaction
New attendings needed skills in developing clinical gestalt, streamlining decision-making, diffusing difficult encounters, and managing expectations. - Managing learners
New attendings felt they lacked skills to diagnose learners, delegate tasks, and set expectations. They also needed to learn how to manage multiple learners and give feedback. - Group culture
New attendings encountered many tacit elements of group culture. These included tacit group practice standards, unspoken codes of conduct, and individual practice quirks. These elements collided with new attendings’ expectations. Their ensuing responses to these conflicts shaped their professional identity.
What can I do? How do we make the tacit more explicit?
For new attendings:
- Seek out near peers who have recently joined the same practice
- Discuss experiences tonormalize experiences and emotions. (Keep imposter syndrome at bay!)
- Seek out more established physicians as mentors to help navigate the system (10).
For senior attendings:
- Acknowledge the presence of (unavoidable) tacit group culture.
- Explicitly state clinical practice patterns and preferences to minimize conflict.
- Recognize that new attendings may need assistance and be willing to do so.
- Mentor a new attending.
For leaders:
- Acknowledge that tacit knowledge and group culture exist in (any) workplace.
- Support formal mentorship and coaching programs for new attendings.
- Offer conflict management workshops to foster growth, and increase collegiality and retention (11,12).


Great article on differentiating the types of learning and their association to your medical profession.