

The role of the emergency department pelvic exam has come under debate for some time. Clinicians have raised concerns regarding whether or not it changes management, whether or not our findings are reliable, and of course the logistic barriers regarding space, time and chaperones. This topic could be approached from many angles, but this article will discuss three main objectives:
- Review the literature discussing the role of the pelvic exam in early pregnancy bleeding, suspected ectopic pregnancy and pelvic inflammatory disease
- Review PID diagnosis and treatment guidelines
- Review practical tips and tools to provide the best patient care around the time of pelvic exam
Pelvic Exam in Early Pregnancy Bleeding
Early pregnancy bleeding occurs in approximately a third of pregnancies. Half of these cases go on to result in pregnancy loss. A population based study in Ontario published in 2020 reported nearly 40% of pregnancies present at some point to an emergency department.1 An American study reported 1-2% of all ED visits were related to early pregnancy bleeding.2
Reading across emergency department literature, obstetrical guidelines and discussing general practice patterns with emergency physicians and obstetricians, there is general agreement that a pelvic exam is necessary in patients with:3
- Heavy vaginal bleeding
- Unstable vital signs
- Concern for vaginal or cervical trauma
- When another diagnostic entity is suspected which requires a pelvic exam (for example, PID)
These scenarios are excluded from the literature that debates the exam’s necessity. In patients with heavy bleeding or unstable vital signs, a speculum exam can facilitate the removal of blood clots or tissue at the cervical os, which can be both diagnostic and therapeutic. If seen, blood clots or tissue should be removed using ring forceps and sponges or gauze.
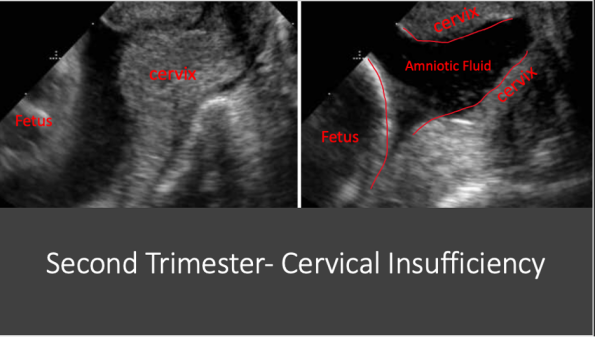
Cervical insufficiency should also be considered in early second trimester pregnancies. This is when the cervix opens prematurely in the absence of labour and can lead to miscarriage or preterm delivery. It is detected either via ultrasound or by seeing an open cervical os on exam. Second trimester patients should be worked up in the department because if cervical insufficiency is identified in an otherwise viable pregnancy, these patients need obstetrics consultation in the department for consideration of cervical cerclage.
More commonly, we are faced with a stable first trimester patient, with relatively small amounts of bleeding. The following studies have attempted to assess the necessity of the pelvic exam in this population
Isoardi, 2009: Review article concluded that the pelvic exam provides no further diagnostic information over ultrasound and beta-hcg testing, with the caveat this is based on low quality evidence.4
Brown, 2011: Prospective study of both pregnant and non pregnant patients, which found 94% of patients did not have management changes based on pelvic exam. This study suggested there may be a subset of the population that could have the pelvic exam omitted, and recommended further study.5
Johnstone, 2013: Randomized study of 135 patients with first trimester bleeding. This study assessed accuracy of diagnosis between patient assessment and ultrasound findings. Patients were randomized to receive a pelvic exam or not as part of their assessment. The study found the accuracy of diagnosis was poor both with and without the pelvic exam. The authors concluded that there is no need for a pelvic exam when ultrasound is readily available. Unfortunately, this study was not powered to detect it’s primary outcome. These results should be interpreted with caution.6
Linden, 2017: Prospective, open label, randomized equivalence trial published in 2017. It included 202 patients under 16 weeks gestation with confirmed intrauterine pregnancy presenting with either lower abdominal pain or vaginal bleeding. Patients were randomized to pelvic exam vs no pelvic exam. The primary outcome was a large composite outcome including need for emergent procedure, transfusion, admission, infection, unscheduled return visits, intervention within 30 days, or identification of alternate source of symptoms. Composite primary outcome occurred in 19.6% of the group without exam vs 22% in the control group (had pelvic). Statistically they could not claim equivalence (predetermined accepted CI -8 to 8), this study was also significantly underpowered.7
Bottom Line- Early Pregnancy Bleeding Pelvic Exams
I don’t think you’re ever wrong to offer the pelvic exam. At the end of the day, we don’t have the evidence to unify our practice pattern or refute guidelines. However, I do think we can improve our discussion with our patients regarding what the pelvic examination can and cannot offer. When discussing the pelvic exam with patients, I recommend we include the following points:
- Acknowledge the lack of evidence “A pelvic exam may or may not change our next steps”
- Discuss the therapeutic potential with your patient: “If there are blood clots or tissue at the cervix that we can see and remove, we may improve your symptoms”
- Approach the concept of alternate diagnoses. “Rarely, there are other causes of bleeding unrelated to your pregnancy, such as polyps or injury to the cervix or vagina. We can’t identify these without an exam”
Ultimately this will be a shared decision between you and your patient.
If you are sending your patient home without a pelvic exam, I recommend they meet the following criteria:
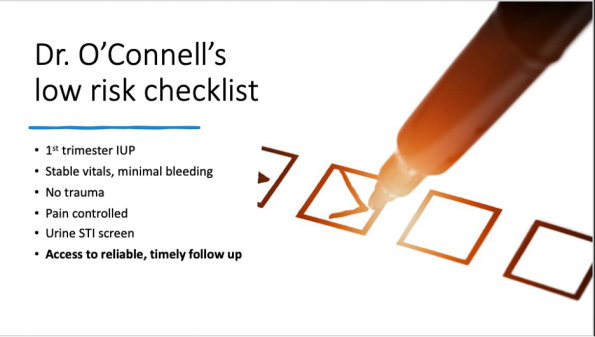
*Not validated
Consider doing an exam even in low risk patients who have had little to no recent medical or gynecologic care, as they are at higher risk of delayed diagnoses of polyps or malignancies.
Pelvic Exam for Ectopic Pregnancy
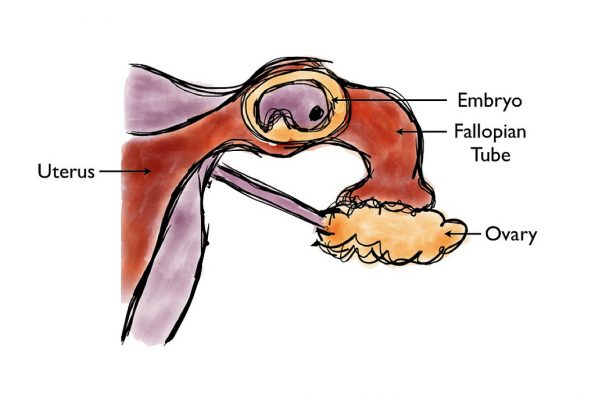
Ectopic pregnancies occur when a developing blastocyst implants to any surface other than the uterine endometrium. 98% of ectopics are tubal, meaning implantation occurred at the fallopian tube.8 Ectopic pregnancies are estimated to occur at a rate of 2-3%, but it’s been estimated that the prevalence of ectopics in the pregnant emergency department population could be as high as 7%.9-11 A ruptured ectopic can be a life threatening emergency. So, can the pelvic exam help us make this diagnosis? The JAMA Rational Clinical Examination series published a systematic review in 2013 to address this question. It included 14 studies, totaling 12,101 patients.12 Test characteristics for each exam finding are outlined in the following table:
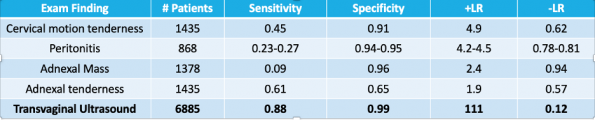
Adapted from JAMA Rational Clinical Exam
Bottom Line- Ectopic Pregnancy Pelvic Exam
A normal or abnormal pelvic exam does not change the need for a transvaginal ultrasound. A normal pelvic exam does not help you classify someone as low risk.
Diagnosis: Pelvic Inflammatory Disease (PID)
PID is an infection of the upper genital tract involving any combination of the endometrium, fallopian tubes, pelvic peritoneum and contiguous structures. Physical exam findings are key to diagnosis, so the importance of the physical exam is not up for debate. If PID is on your differential, the patient requires a pelvic exam (if they are agreeable). Any patient with a uterus/cervix/fallopian tubes and unexplained lower abdominal pain should have PID on their differential. The CDC estimates that up to 2/3 of cases go unrecognized!
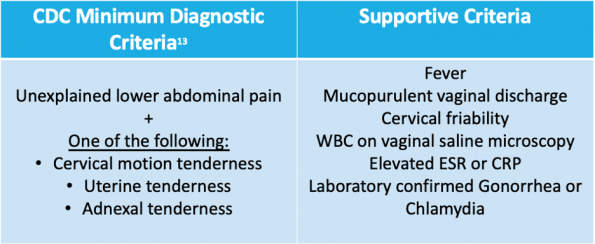
PHAC Diagnostic Criteria:The PHAC guidelines list their minimal diagnostic criteria as lower abdominal pain, CMT and adnexal tenderness, but they don’t provide any information regarding how many of these exam findings should be present.14
PID Risk Factors13
- Multiple sexual partners: 4 or more sexual partners in last 6 months increases PID risk by a factor of 3
- Age: Highest frequency in those with female anatomy ages 15-25
- Previous STI or PID
- Inconsistent use of barrier protection
- Recent instrumentation (IUD insertion in last 3 weeks, saline sonohystogram)
PID: A Diagnostic Challenge
Unfortunately, there is no single historical, physical or laboratory finding that is both sensitive and specific for PID. The diagnosis is difficult, as only 1/3 of cases will have fever, causative organisms include both those are sexually transmitted and some that are not, and negative swabs do not rule out PID. Untreated cases have a high risk of future complications, including but not limited to tubo-ovarian abscess, chronic pelvic pain, ectopic pregnancy and infertility.13,15 While cervical pathogens such as gonorrhea and chlamydia make up 50-85% of cases, many other organisms that can lead to infection of the upper genital tract. These include enteric and respiratory pathogens, as well as endogenous organisms such as those frequently responsible for bacterial vaginosis.16
There is also variety in the interpretation of physical exam findings, as demonstrated by a 2001 study by Close and colleagues.17 In this study of 186 patients, attendings and senior residents who decided a pelvic was needed as part of their assessment had another physician repeat the exam. Agreement of findings between the two physicians was assessed. Reliability < 50% deemed poor prior the start of the study. Agreement on exam findings ranged from 71-84% overall, but in positive exam findings, agreement was only 17-33%, with lowest agreement of 17% occurring for the detection of cervical motion tenderness.
PID and Infertility
A large prospective study in the early 90s identified the risk of tubal factor infertility in patients with PID was just over 10%. The risk of TFI increases with the number of episodes of PID, with infertility rates of nearly 40% after 3 episodes. The risk increased further if you were over 25 years old at age of first infection.15
PID is reported to be the leading PREVENTABLE cause of infertility.
PID: Updates in Outpatient Treatment
Now that we have made diagnosis, how are we going to treat it?
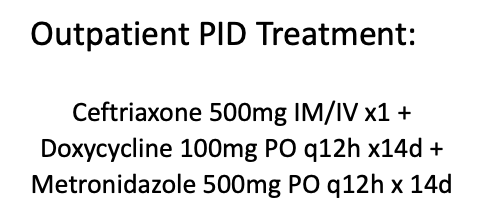
1) Ceftriaxone 500mg IM or IV
- Recent CDC guideline updates recommend increasing ceftriaxone dosing for gonorrhea from 250mg to 500mg based on resistance patterns and the amount of time serum concentrations stay above the MIC (minimum inhibitory concentration).18
- 500mg was the lowest dose that was 100% effective at eradicating gonorrhea in individuals up to 100kg.
- Increase dose to 1g for patients over 150kg.
2) Doxycycline 100mg PO q12h x 14 days
- Doxycycline has been recommended over azithromycin for PID for several years now as per the CDC, PHAC and our local guidelines in Ottawa, ON.13,14
- If you are choosing to use azithromycin (if patient cannot tolerate doxycycline or will not adhere to 2 weeks of treatment), single dose is no longer recommended. You may choose from the following two azithromycin options:
- Azithromycin 1g PO qweekly x 2 doses
- Azithromycin 500mg PO x1 followed by 250mg PO daily x 6 days
3) Metronidazole 500mg q12h x 14 days
- The decision of adding metronidazole has often been left up to the provider. It’s been debated in PID treatment because anaerobes are often detected in the lower genital tract, but their exact role in PID and sequelae of infection are not well known.
- Recently, there was a randomized placebo-controlled trial that compared ceftriaxone + doxy + metronidazole with ceftriaxone and doxy alone.19 This study enrolled 233 patients diagnosed with acute PID. The primary outcome was clinical improvement at 3 days following enrolment, which was similar between groups at 96 vs 90% (p=0.13). Secondary outcomes included presence of anaerobic organisms in the endometrium and clinical cure at 30 days. Pelvic organ tenderness on abdominal and pelvic exam was still present at 30 days in only 9% of patients in the metronidazole group, compared to 20% of patients in the placebo group. There were also decreased rates of bacterial vaginosis in the metronidazole arm at 30 days. This study’s secondary outcome is one of the main contributors to the body of evidence that has lead to the CDC’s recommendation of adding metronidazole to all cases. Although it was not a primary outcome, the potential for improved symptoms at 30 days makes metronidazole a worthwhile addition.
- Metronidazole is recommended here in Ottawa by our local ID specialists.
Some patients will require admission to hospital for PID, including but not limited to:
- Severe illness, nausea and vomiting, oral temperature >38.5
- No clinical response to oral outpatient therapy
- Unable to follow or tolerate outpatient regimen
- Presence of tubo-ovarian abscess
- Pregnancy
- Unable to exclude other surgical emergency (ex appendicitis)
A few more notes on PID
- You can give ceftriaxone IV! Both IM and IV routes achieve the appropriate MIC for gonorrhea.
- Mycoplasma genitalium is an organism that has recently been recognized as a possible PID, cervicitis and urethritis pathogen. It is not part of our usual testing for PID and won’t grow on our usual swabs. However, it is something to consider in patients who are returning to the ED with unresolving infections. You can test for mycoplasma by sending PCR swabs to the Ontario public health lab with approval from the microbiologist on call. Treatment of choice for M. genitalium is moxifloxacin.
- Cervical, vaginal (self-collected or provider collected) and urine samples are all appropriate for gonorrhea and chlamydia testing.
- You do NOT need to remove an IUD if your patient has PID. Removal may be required if they do not respond to usual first line therapy.
Bottom Line- PID
Increase your suspicion for PID! Any patient of reproductive age with a uterus and unexplained acute lower abdominal or pelvic pain should be screened for G/C, undergo pelvic exam if agreeable and considered for diagnosis and treatment of PID, even if physical exam findings are equivocal.
Optimize your Pelvic Exam
Adolescence
Teenagers who have never been sexually active with insertive intercourse should not have a speculum exam. However, remember that these patients are still at risk of PID as sexually transmitted infections can spread via other forms of sexual contact. If you’re asking your teenage patient if they are sexually active and they say no, you need to clarify what exactly they mean. This is a great population to take advantage of urine NAT testing or self swab for gonorrhea and chlamydia. Also consider throat swabs for G+C in teenage patients with persistent or non resolving pharyngitis.
LGBTQ+
Any patient with a vagina, cervix, uterus, fallopian tubes or ovaries is at risk of gynecologic pathology. For transgender patients, ask where they are in their transition. Are they on hormones? Have they had surgery? If so, which ones? In Canada, there are only a few clinics doing bottom surgery. Many patients transitioning will have pelvic organs from their sex assigned at birth. For patients on hormone therapy, remember that testosteronized vaginas get smaller, so use a smaller speculum or even a pediatric speculum in these cases. Consider using the neutral phrase “genital exam” rather than pelvic exam, and mirror the language that patients use for their own anatomy.
Unstable Patients
Patients with significant vaginal bleeding will often be in monitored stretchers that don’t break in half. In these cases, try flipping the speculum upside down and inserting it with the handle up. This way the handle is not getting caught on the bed.
Expand your Resources
Patients who have had multiple children or have higher BMI can have vaginal walls that obstruct your view of the cervix. In these cases, there are several tricks to optimize your view. One option is to cut the end off a condom and place it over the speculum. Another option is to use tongue depressors to hold the lateral walls of the vagina out of your view once your speculum is inserted.
Trauma Informed Approach
For some patients, the pelvic exam is a lot different than an abdominal or cardiac exam. Patients with a history of sexual assault and trauma can have a complex relationship with the pelvic exam. So how can we approach this?
- Ensure you are providing a detailed explanation of the exam prior to starting it. Then, explain each step again as your do the exam. Remind your patient that they can tell you to STOP at any point.
- If your patient needs an exam for both forensic and medical purposes, ensure all required tasks are done at the same time. You can avoid repeating the exam.
- Transgender populations are at higher risk for sexual assault and these assaults can be of a more violent nature. The exam in this scenario should take extra care to assess for vaginal or cervical lacerations, as well as rectal trauma.
- Remember, nearly 1 in 3 women have a lifetime history of sexual assault. The first part of your trauma informed approach is to screen for this on history before every exam, and assume that this could be your patient’s reality. In addition to screening for prior assault, ask your patient if they have had a poor experience with a pelvic exam in the past, or if a provider has had to switch to a smaller speculum on previous exams.
References
Author
![]()