
Below is based on studies of each class of drug used in isolation and in healthy individuals:
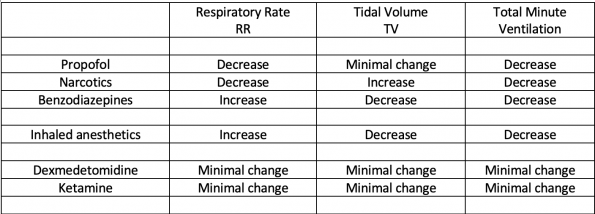
Propofol: Decrease RR, minimal effect on TV (patients use diaphragm less, and accessory muscles more for net effect of minimal change in TV); can induce apnea at common doses used
Narcotics: Decrease RR, partial compensatory increase TV; can induce apnea at common doses used
Benzodiazepines: Decrease TV, partial compensatory increase in RR; unlikely to cause apnea (very similar to inhaled anesthetics)
Dexmedetomidine: Minimal effects on respiration
Ketamine: Minimal effects on respiration
Inhaled anesthetics: Decrease TV, partial compensatory increase RR; will not significantly blunt respiratory drive except when very high doses such as when close to isoelectric EEG (isoelectric EEG usually occurs at 1.5-2 MAC, eg in 40yo pt, where 1MAC=1.1 ET% isoflurane, this is at about 1.7-2.2 ET% isoflurane)