

You have just seen an 10 month old previously healthy well-appearing female with 2 day history of fever (Tmax 39.5). No focus of infection is obvious on history of examination. Vitals are normal when ibuprofen is on board. She is completely unimmunized. What is your approach to work up? Does this differ from a completely immunized child?
We all know that most well-appearing children >3 months of age with fever will have a virus – this is true of both unimmunized and immunized children. But what about those infants who aren’t “just a virus”? When we are stuck with no great explanation for fever on both our history and examination, the most likely serious bacterial infections that we could be missing are urinary tract infections, pneumonia, or “walking” bacteremia. Of these, the incidence of pneumonia and bacteremia have been greatly affected by vaccine availability and uptake in the last 35 years.
Vaccine Preventable Serious Bacterial Infections in Infants
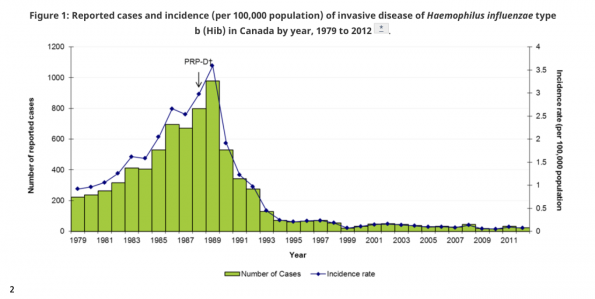
Heamophilus Influenzae is a gram negative coccobacillus that is either typeable (encapsulated) or non-typeable (non encapsulated). Encapsulated serotypes a to f are most likely to cause invasive disease, the most pathogenic of which is Heamophilus Influenza type b (Hib). Though some diseases like; epiglottitis, meningitis, cellulitis, and septic arthritis may be clinically apparent, there is a worry that occult bacteremia with Hib may harold these severe infections and the only presenting symptom of Hib pneumonia may be a fever1.
Thankfully, there has been a dramatic decline in the incidence of invasive disease caused by Hib since the late 80’s which has been maintained over time.
Streptococcus pneumoniae is a gram positive bacterium with 92 serotypes worldwide. Though strep pneumo is implicated in our run of the mill respiratory track infections, it is also a culprit in invasive pneumococcal disease manifesting as bacteremia or bacteremic pneumonococcal pneumonia. Similar to Hib, there is a point in the illness where the only manifestation of invasive disease may be fever.
Thankfully, due to the implementation of the pneumococcal conjugate vaccines (C-7, 2002-2006; C10 2009; C13 2010-now), the incidence of invasive pneumococcal disease has also drastically decreased.1
These trends provide significant comfort in clinicians treating infants without a source for their fever who are immunized, but…
How often do Vaccine Preventable Serious Bacterial Infections occur in Unimmunized Children?
The incidence of occult bacteremia in children aged 3-36 months in the pre-vaccine era was estimated at 3-11%. We all know that the rates of vaccine preventable diseases in the community have remained low in the population due to herd immunity*- in fact, in all comers it is estimated the rate of bacteremia in well looking children is <1%. To look at this specifically related to vaccination status, a study was published in the Journal of Pediatrics May 2021, entitled “Association of Bacteremia with Vaccination Status in Children Aged 2-36 Months”3:
Questions and Methods: The authors looked to determine the rate of bacteremia in under or unimmunized children based on state vaccine registry using a retrospective cohort design of children aged 2-36 months with blood cultures obtained in the ED
Findings: The rate of vaccine preventable bacteremia in 857 patients regardless of vaccination status was 0% (in their population, one child had a vaccine preventable pathogen, and they were fully immunized)
Limitations: The region in which the study was completed has a 96.3% vaccination rate which may limit generalizability to regions with lower rates of vaccination
Interpretation: The incidence of vaccine preventable bacteremia in areas of high vaccination rates is essentially non-existent but the study is not powered to detect an association with vaccination status
*the immunization rate for herd immunity for these pathogens is NOT well defined
Does our Approach Differ for Unmmunized Children?
Hot of the press! A study recently published in Pediatric Emergency Care in January 2023, entitled “Immunization Status and the Management of Febrile Children in the Pediatric Emergency Department: What are we doing?” looked at management patterns in ED providers for this population 4.
Questions and Methods: The authors looked at practice patterns differences of emergency physicians treating well-appearing febrile children using a retrospective cohort design of children aged 3-36 months based on caregiver report of immunization status
Findings: Under or unimmunized children were more likely to be investigated with bloodwork and more likely to be given antibiotics
Interpretation: There is a suspicion amongst care providers of serious bacterial infection, like what was seen in the pre-vaccine era
Should our Approach Differ for Unimmunized Children?
Two separate expert recommendations have been published advising clinicians to obtain bloodwork to guide decision making. Quite like our guidance around febrile infants less than 3 months of age, these experts recommend utilizing a WBC threshold of 15, ANC >10, band >1.5 or procalcitonin >0.5 to send blood cultures and empirically treat while awaiting results in unimmunized well-looking children. They also both refer to a study which showed that a WBC> 20 is an independent predictor of occult pneumonia regardless of clinical signs and suggest that clinicians obtain a CXR. The proposed algorithm from Finkel et al, 20215:
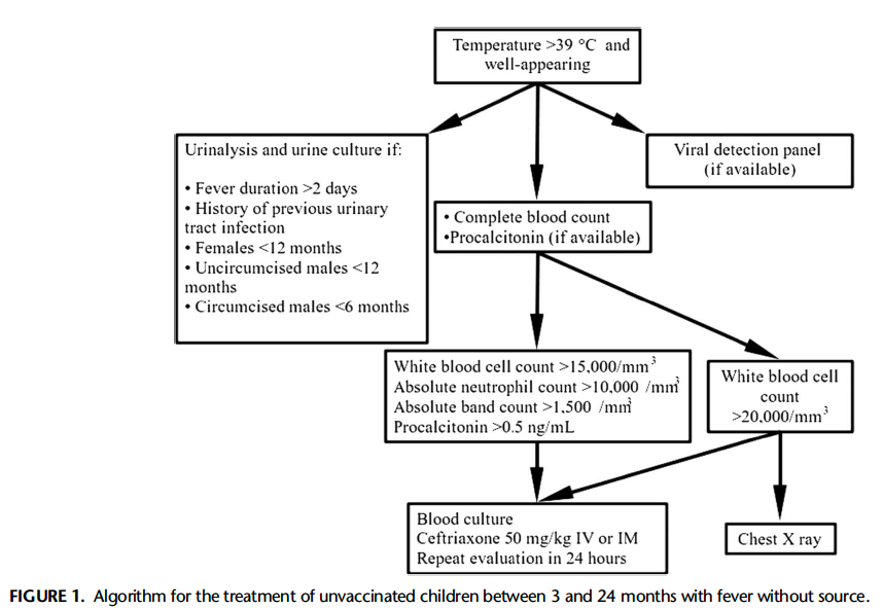
It is important to note that many experts feel that this is an over-conservative approach, given the rate of bacteremia in well-appearing children.
Vaccination Rates in the COVID-19 Era
 Unfortunately, the situation is not getting any clearer. We are seeing many more children who are unvaccinated or under vaccinated presenting to the ED. In July of 2022, WHO and UNICEF released data demonstrating the largest sustained decline in childhood vaccinations in 30 years. They estimated that in 2021, 25 million infants worldwide under the age of 1 did not receive basic vaccinations—this was the highest number since 2009. Further, the number of completely unvaccinated children increased by 5 million between 2019 and 2021 worldwide6.
Unfortunately, the situation is not getting any clearer. We are seeing many more children who are unvaccinated or under vaccinated presenting to the ED. In July of 2022, WHO and UNICEF released data demonstrating the largest sustained decline in childhood vaccinations in 30 years. They estimated that in 2021, 25 million infants worldwide under the age of 1 did not receive basic vaccinations—this was the highest number since 2009. Further, the number of completely unvaccinated children increased by 5 million between 2019 and 2021 worldwide6.
When it comes to a high-income nation like Canada, the situation is also concerning. Studies in Alberta and Quebec mirror this trend showing sustained decrease in rate of vaccination related to the pandemic7,8. Reasons behind this are numerous: diversion of resources to mitigating outbreaks, social distancing measures, and increasing vaccine hesitancy amongst parents9.
Conclusions
Though rates of vaccine preventable serious bacterial infections are low, it is imperative that the ED physician remains vigilant to the possibility of vaccine preventable diseases and their complications particularly in the era of vaccine hesitancy, decreased access to primary care and pandemic related decrease in immunization rates.
References
- Canada Public Health Immunization Information. https://www.canada.ca/en/public-health/services/immunization-vaccines.html.
- Canada Public Health Hib Graph. https://www.canada.ca/en/public-health/services/immunization/vaccine-preventable-diseases/haemophilus-influenzae-disease/health-professionals.html#figure-1.
- Dunnick J, Taft M, Tisherman RT, Nowalk AJ, Hickey RW, Wilson PM. Association of Bacteremia with Vaccination Status in Children Aged 2 to 36 Months. Journal of Pediatrics. 2021;232:207-213.e2. doi:10.1016/j.jpeds.2021.01.005
- Curtis M, Kanis J, Wagers B, et al. Immunization Status and the Management of Febrile Children in the Pediatric Emergency Department What Are We Doing? Pediatric Emergency Care •. 2023;39(1). www.pec-online.com
- Finkel L, Ospina-Jimenez C, Byers M, Eilbert W. Fever Without Source in Unvaccinated Children Aged 3 to 24 Months What Workup Is Recommended?; 2021. www.pec-online.com
- WHO and UNICEF sound alarm over vaccination backslide. https://www.who.int/news/item/15-07-2022-covid-19-pandemic-fuels-largest-continued-backslide-in-vaccinations-in-three-decades.
- Macdonald SE, Paudel YR, Kiely M, et al. Impact of the COVID-19 pandemic on vaccine coverage for early childhood vaccines in Alberta, Canada: A population-based retrospective cohort study. BMJ Open. 2022;12(1). doi:10.1136/bmjopen-2021-055968
- Kiely M, Mansour T, Brousseau N, et al. COVID-19 pandemic impact on childhood vaccination coverage in Quebec, Canada. Hum Vaccin Immunother. 2022;18(1). doi:10.1080/21645515.2021.2007707
- Maltezou HC, Medic S, Cassimos DC, Effraimidou E, Poland GA. Decreasing routine vaccination rates in children in the COVID-19 era. Vaccine. 2022;40(18):2525-2527. doi:10.1016/j.vaccine.2022.03.033
