
Acute pancreatitis is one of the most common gastroenterology conditions we see in the emergency department with a prevalence of 110-140 cases per 100,000 population. (1) At The Ottawa Hospital alone, we saw over an average of 1 case per day over the last year. Unfortunately, a lot of what we do in the emergency department is still following the dogma of traditional teaching. New evidence has been arising in the recent years about how we could be improving the ED management of acute pancreatitis.
Recall the diagnostic criteria for acute pancreatitis (>2/3):
- Abdominal pain consistent with acute pancreatitis
- Elevated amylase or lipase more than 3 times upper limit of normal
- Characteristic findings of acute pancreatitis on imaging
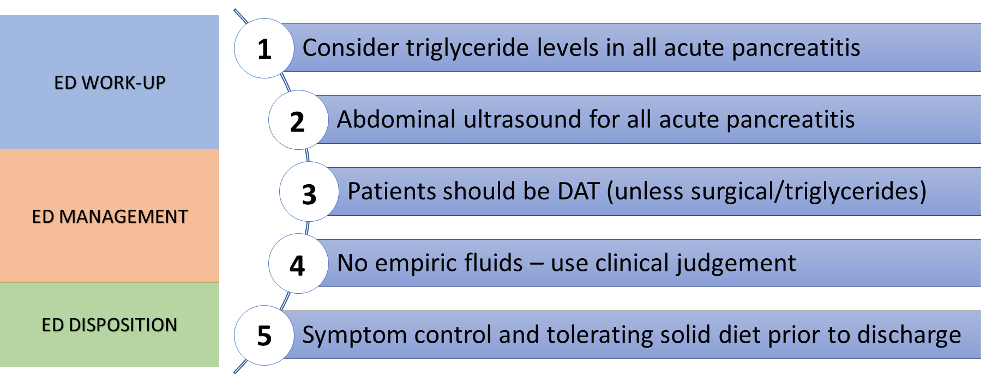
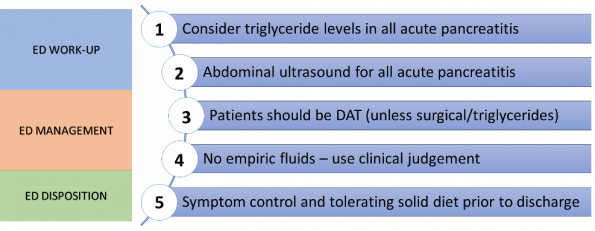
Take home #1: Consider ordering a triglyceride level in all diagnosis of acute pancreatitis.
In medical school, we were taught mnemonics for the differential of acute pancreatitis (e.g. I GET SMASHED) but not all of these will be clinically relevant. Pragmatically, we tend to think about acute biliary causes, chronic alcohol, and lump everything else together to be assessed on a case-by-case basis. However, hypertriglyceridemia should be the next consideration on your mental checklist for all of these patients for a few different reasons.
It’s much more common than you think!
- Multiple studies and reviews have found this was the 3rd most common single cause of acute pancreatitis after gallstones and chronic alcohol use with a rate of approximately 5% in North American populations (1 in 20 cases)
- In East Asian populations, this has been quoted to go up to as high as 20% in certain studies (2)
Hypertriglyceridemia induced acute pancreatitis patients are sicker!
- Multiple reviews have found that these patients have worse outcomes including increased mortality, organ failure, SIRS scores (3–5)
Hypertriglyceridemia induced acute pancreatitis needs different management!
- These patients need to be admitted to hospital and placed on NPO
- They need specific hypertriglyceridemia management including IV insulin +/- heparin, plasmapheresis that need specialist involvement.
Take home #2: A biliary ultrasound should be obtained in all patients with acute pancreatitis.
Although gallstones are still by far the most common cause of acute pancreatitis, not all patients will present the same. As emergency physicians, we try to be judicious for our investigations and imaging. When patients appear well, have no abdominal pain, or their liver enzymes are normal, we may not think an ultrasound to rule out gallbladder pathology is required for these patients. However, in the case of acute pancreatitis, the gallbladder should be imaged with ultrasound for all of these cases for several reasons.
Even when we don’t think it’s the gallbladder, it still might be the gallbladder!
- Biliary pathology is still by far the most common cause acute pancreatitis (up to 70% in literature) (1)
- Even in cases with initial diagnosis of idiopathic acute pancreatitis, the gallbladder ends up being the culprit in 28-80% of cases (2)
- If there is imaging evidence of microlithiasis and sludge without evidence of gallstones or obstruction, the gallbladder is still considered to be the culprit.
- There is now growing evidence for consideration of elective cholecystectomy in patients with idiopathic pancreatitis as this prevents recurrent episodes! (6)
Surgical management is important for this patient population to prevent poor outcomes and recurrence!
- There is an underlying surgical pathology for these patients that needs to be performed
- Studies show a 25-30% recurrence rate for patients who do not receive a cholecystectomy (7)
Take home #3: Patients with idiopathic acute pancreatitis can immediately be on diet as tolerated.
Historically, the teaching was for patients with acute pancreatitis to be nil per os (NPO) due to concern of food increasing pancreatic stimulation and worsening disease process. But current evidence has shown that NPO status can lead to GI mucosal atrophy, bacterial overgrowth, and higher rates of sepsis and infection. But how do we achieve this in the ED and how quickly can we allow patients to eat?
- Early enteral nutrition was long ago established as preferable over parenteral nutrition in a Cochrane review in 2010 (8)
- Reviews have shown that enteral nutrition early on in patient’s course of admission was found to have significantly better outcomes in terms of rates of complications and length of stay (9)
- Recent studies have shown that immediate oral nutrition is much superior to step-wise progression of diet in terms of length of hospital stay, symptoms (nausea, vomiting, pain), and decreased rate of complications and ICU admission (10)
Take home #4: There is no role for empiric IV fluids, use clinical judgement for fluid resuscitation
Acute pancreatitis at its core is due to pathophysiology of large amounts of inflammation that can theoretically lead to third spacing and decreased intravascular volume. Therefore, historically, recommendations were for massive amounts of empiric fluid resuscitation to counteract this. Over the years, multiple studies have shown the downsides of empiric large volume resuscitation in acute pancreatitis leading to volume overload, respiratory symptoms, and increased complications (11,12)
The WATERFALL trial recently published in NEJM has been the most up to date data on fluid resuscitation in acute pancreatitis (13).
- This was a multi-centered, randomized, open label study that included 4 countries which ended up enrolling 249 patients with mild/moderate acute pancreatitis
- They randomized patients to receiving one of two groups:
- Aggressive fluid resuscitation (20 cc/kg bolus + 3 cc/kg/hr)
- Moderate fluid resuscitation (1.5 cc/kg/hr +/- 10 cc/kg bolus if hypovolemic)
- Their primary outcome was development of severe acute pancreatitis with secondary outcomes examining organ failure, rates of ICU admission, length of hospital stay, SIRS scores
- They had a safety outcome looking at rates of fluid overload and complications secondary to this
- They found that there was no difference in their primary and secondary outcomes
- However, they found there was a significantly higher rate of fluid overload in the aggressive fluid resuscitation (20.5%) compared to the moderate fluid resuscitation group (6.3%)
This might sound obvious but when you do the math for an “average” 70kg patient, the “moderate fluid resuscitation” is only approximately 105 cc/kg which is just below maintenance for body weight. This really adds to the evidence that we are really only giving patients the fluids that they cannot replace themselves. Therefore, give these patients a bolus if they look dry, if not, put them on maintenance if they cannot tolerate fluids themselves (see take home #3)!
Take home #5: Be cautious with discharge unless patients have well controlled symptoms and are able to tolerate a solid oral diet
Traditionally, 5-10 years ago, almost all patients with acute pancreatitis were being admitted to hospital. As evidence increased for earlier oral intake, decreased need for aggressive IV fluids and antibiotics, we are starting to discharge more and more of these patients from the ED. Although there have been multiple risk stratification systems proposed for acute pancreatitis such as the Ranson criteria or BISAP score, there is no clear-cut guidance for discharge from the ED.
If we delved into the inpatient literature, there have been certain risk factors that are repeated implicated in studies for worse outcomes and higher rates of readmission to hospital (14–17):
- Intolerance of a solid oral diet
- Severe gastrointestinal symptoms including vomiting
- Severe abdominal pain
- Higher morphine equivalent doses of opioid analgesics (another marker of abdominal pain)
This tells us that the presence of these factors should really give us pause before we discharge the patient. These should not be patients that we quickly discharge from the ED as soon as they are able to tolerate some oral rehydration after ondansetron, they have a true intra-abdominal disease process for which we should be mindful! While you are awaiting a trial of oral intake, it can be helpful to obtain a delta lipase to understand which direction the patient is trending (ie: pancreatic enzymes going up or down), as this may influence your disposition.
References
- Mederos MA, Reber HA, Girgis MD. Acute Pancreatitis: A Review. JAMA. 2021 Jan 26;325(4):382–90.
- Del Vecchio Blanco G, Gesuale C, Varanese M, Monteleone G, Paoluzi OA. Idiopathic acute pancreatitis: a review on etiology and diagnostic work-up. Clin J Gastroenterol. 2019 Dec 1;12(6):511–24.
- Adiamah A, Psaltis E, Crook M, Lobo DN. A systematic review of the epidemiology, pathophysiology and current management of hyperlipidaemic pancreatitis. Clinical Nutrition. 2018 Dec;37(6):1810–22.
- Wang Q, Wang G, Qiu Z, He X, Liu C. Elevated Serum Triglycerides in the Prognostic Assessment of Acute Pancreatitis: A Systematic Review and Meta-Analysis of Observational Studies. Journal of Clinical Gastroenterology. 2017 Aug;51(7):586–93.
- Rawla P, Sunkara T, Thandra KC, Gaduputi V. Hypertriglyceridemia-induced pancreatitis: updated review of current treatment and preventive strategies. Clin J Gastroenterol. 2018 Dec 1;11(6):441–8.
- Räty S, Pulkkinen J, Nordback I, Sand J, Victorzon M, Grönroos J, et al. Can Laparoscopic Cholecystectomy Prevent Recurrent Idiopathic Acute Pancreatitis?: A Prospective Randomized Multicenter Trial. Ann Surg. 2015 Nov;262(5):736–41.
- Hernandez V, Pascual I, Almela P, Añon R, Herreros B, Sanchiz V, et al. Recurrence of acute gallstone pancreatitis and relationship with cholecystectomy or endoscopic sphincterotomy. Am J Gastroenterol. 2004 Dec;99(12):2417–23.
- Al-Omran M, AlBalawi ZH, Tashkandi MF, Al-Ansary LA. Enteral versus parenteral nutrition for acute pancreatitis. Cochrane Upper GI and Pancreatic Diseases Group, editor. Cochrane Database of Systematic Reviews [Internet]. 2010 Jan 20 [cited 2023 Jan 25]; Available from: https://doi.wiley.com/10.1002/14651858.CD002837.pub2
- Feng P, He C, Liao G, Chen Y. Early enteral nutrition versus delayed enteral nutrition in acute pancreatitis: A PRISMA-compliant systematic review and meta-analysis. Medicine. 2017 Nov;96(46):e8648.
- Ramírez-Maldonado E, López Gordo S, Pueyo EM, Sánchez-García A, Mayol S, González S, et al. Immediate Oral Refeeding in Patients With Mild and Moderate Acute Pancreatitis: A Multicenter, Randomized Controlled Trial (PADI trial). Annals of Surgery. 2021 Aug;274(2):255–63.
- Li L, Jin T, Wen S, Shi N, Zhang R, Zhu P, et al. Early Rapid Fluid Therapy Is Associated with Increased Rate of Noninvasive Positive-Pressure Ventilation in Hemoconcentrated Patients with Severe Acute Pancreatitis. Dig Dis Sci. 2020 Sep;65(9):2700–11.
- Gad MM, Simons-Linares CR. Is aggressive intravenous fluid resuscitation beneficial in acute pancreatitis? A meta-analysis of randomized control trials and cohort studies. WJG. 2020 Mar 14;26(10):1098–106.
- de-Madaria E, Link to external sitethis link will open in a new window, Buxbaum JL, Maisonneuve P, Link to external site this link will open in a new window, Paredes AGG de, et al. Aggressive or Moderate Fluid Resuscitation in Acute Pancreatitis. The New England Journal of Medicine. 2022 Sep 15;387(11):989–1.
- Whitlock TL, Tignor A, Webster EM, Repas K, Conwell D, Banks PA, et al. A Scoring System to Predict Readmission of Patients With Acute Pancreatitis to the Hospital Within Thirty Days of Discharge. Clinical Gastroenterology and Hepatology. 2011 Feb;9(2):175–80.
- Whitlock TL, Repas K, Tignor A, Conwell D, Singh V, Banks PA, et al. Early Readmission in Acute Pancreatitis: Incidence and Risk Factors. Official journal of the American College of Gastroenterology | ACG. 2010 Nov;105(11):2492.
- Buxbaum J, Quezada M, Chong B, Gupta N, Yu CY, Lane C, et al. The Pancreatitis Activity Scoring System predicts clinical outcomes in acute pancreatitis: findings from a prospective cohort study. Am J Gastroenterol. 2018 May;113(5):755–64.
- Wu BU, Batech M, Quezada M, Lew D, Fujikawa K, Kung J, et al. Dynamic Measurement of Disease Activity in Acute Pancreatitis: The Pancreatitis Activity Scoring System. Am J Gastroenterol. 2017 Jul;112(7):1144–52.

Trackbacks/Pingbacks