
Patients with heart failure are often newly diagnosed in the Emergency Department, or are the presenting location for those with decompensated heart failure. This is why it is important for ER Physicians to remain updated on the latest AHA/ACC/HFSA guidelines for the management of heart failure. In this post, we are going to touch on:
- BNP has new class 1 indications for the assessment of ambulatory patients
- Considerations around diuresis strategies (agents, dosing, 2nd line diuretics)
- Importance of continuing goal directed medical therapy (GDMT) for admitted patients
- SGLT2 inhibitors, and their importance, considering increase prevalence across all classes of heart failure and subsequent increased complication rates.
1. BNP in Heart Failure (Class 1 Indications)
What is BNP?
- B type natriuretic peptide is a natriuretic hormone released from the heart, in particular the ventricles. The release of his hormone increases in heart failure as ventricular cells are recruited in response to high ventricular filling pressures. The assay ranges from 5-4000pg/ml (picogram from mililiter). It is classifically taught that a BNP > 500 is suggestive of heart failure and value below 100pg/ml have a very high negative predictive value for HF.
What is the difference between proBNP and BNP?
- Both vasoactive peptides, BNP has a shorter half life than NT-proBNP with is an inactive peptide that circulates longer. (20 mins vs 1-2 hours). BNP is cleared by plasma and nt proBNP is cleared by renal excretion.
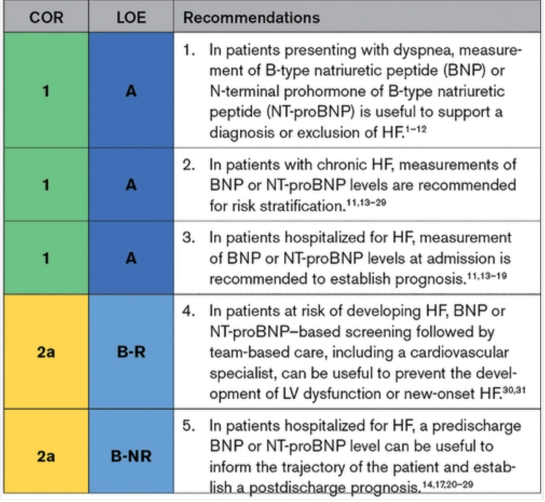
Patients with dyspnea measurement of BNP or NT-proBNP is useful for diagnosis/exclusion of heart failure
- This is a controversial topic as we now have increased use of point of care ultrasound which aids our clinical diagnosis of CHF exacerbation (click here for a useful guide on point-of-care echocardiography). Many of the studies from which this recommendation stems are from the early 2000s such as:
-
- Maisel et al. (2002)
- Kimmenade et al. (2006)
- Maisel (2004)
-
These studies suggested that BNP or NT pro BNP were useful in aiding in the diagnosis of CHFe. The last suggested that BNP may be more sensitive than physician gestalt in the severity of the CHF exacerbation. Ultimately, this may be another data point in your diagnostic toolbox, but is not independently useful.
In patients with Chronic heart failure, measurements of BNP or NT-proBNP levels are recommended for risk stratification.
- The PONTIAC trial (2013) was an RCT of 300 patients with aim to assess effectiveness of neurohumoral therapy for prevention of cardiac events in pts with T2DM with increased NT-proBNP. They found that there was a significant reduction in hospitalized or death due to cardiac disease in following 24 months in intervention group (HR 0.351, 95% CI: 0.127-0.975; p=0.044)
- A metaanalysis by Brunner-La Rocca et al. 2015 of 8 pro BNP trials aimed to assess which HF pts benefit from NT-pro BNP therapy. They included patients with HFpEF and HFrEF. They found:
- Lower mortality in HFrEF with guided treatment (HR: 0.78; 95% Ci 0.62-0.97; p=0.03)
- Other studies RCTs and meta-analysis that shows that BNP guided therapy (either BNP or NT-proBNP significantly reduce all cause mortality and HF related hospitalization
- Xing and al. 2015
- Troughton et al. 2014
- De vecchist et al. 2014
- Balion et al. 2014
- Savarese et al. 2013
- This is why cardiologists and internists find serial BNPs to be useful, the literature has shown time and time again that there is an obvious benefit in reducing harm in by recognizing risk of exacerbations prior to their onset and guiding patients’ GDMT in accordance.
Patients hospitalized with BNP or NT pro-BNP levels at admission is recommended to establish prognosis.
- Appears to have mixed evidence on inpatient management
- BNP/Pro-BNP guided therapy suggest that modifications to therapies were completed with the measurement of serial levels. These were used are markers of decongestion in the fluid overloaded CHFe patients.
- Some studies showed positive endpoints with the use of BNP/pro BNP guided therapy
- RCT by Berger et al. (2010)
- BATTLESCARRED RCT (2009)
- Some studies showed negative endpoints
- PRIMA II RCT (2017)
- Some showed no difference
- GUIDE-IT RCT (2017)
- It was also found that 30 day readmission was associated with elevated BNP. For example those with BNP > 1000 had a 3 fold increase in readmission rate as per a retrospective chart review published in JAMA 2014.
- GUIDE-IT RCT (2017)
Barriers to use in the ED:
- BNP/Pro BNP is simply supporting data, not a confirmatory test. It has never been clear that BNP can outperform physician judgement, but the guidelines emphasize its use in prognostication and avoidance of adverse events.
- It has high sensitivity, low specifity and therefore can be elevated in other conditions:
- Renal failure, AOS, cardiomyopathy may increase values
- BNP will be lower in obese patients
BOTTOM LINE
- Continue to consider its’ use in diagnostic uncertainty keeping in mind that CHF is a clinical diagnosis.
- Consider ordering in patient’s you will refer to internal medicine and Cardiology as there is a definite role in prognostication and prediction of adverse outcomes.
2. Diuretics: Decongestion Strategy
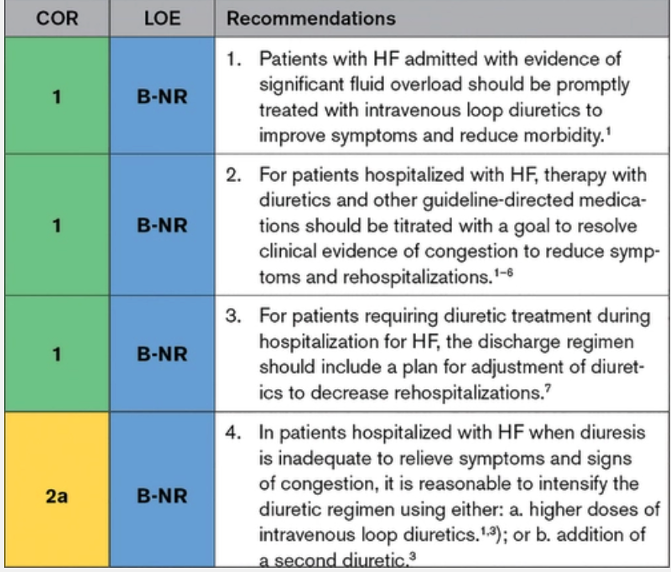
- Intravenous loop diuretics like furosemide provide the most rapid and effective treatment for signs and symptoms of congestion leading to hospitalization for HF
- Failing to successfully accomplish decongestion prior to discharge leads to higher rates of re-hospitalization and mortality
- Our goals in the ED:
- Administration of furosemide early
- REALITY–AHF was a prospective multicenter observational study. This study noted that patients who receive furosemide within 60 mins (37.3%) after presentation had a lower hospital mortality than those who receive it after 60 minutes (62.7%). This is for the pulmonary vasodilatory effects of furosemide which occur within the first 10 minutes of administration. This study had some flaws, in that association rather causality was demonstrated in this study. The patients who receive furosemide early had obvious signs of volume overload.
- Starting dose of furosemide
- 2x the home diuretics dose mg to mg administered IV
- Can start with 40mg IV if furosemide naïve
- The DOSE trial (2011) Was a RCT with 2×2 factorial design comparing high and low dose IV loop furosemide and bolus vs continuous infusion. It showed that there was greater relief of dyspnea with higher doses of furosemide.
- Take note that if your patient your patient may have an worsening renal function in the setting of volume overload but Furosemide will not cause an AKI. What will cause the renal injury is if the fluid assessment is inaccurate, and diuresis is given for a patient that in fact volume deplete.
- Those with cardiorenal syndrome actually warrant more furosemide than our mildly congested patient.
- Added therapies?
- This was not specifically mentioned in the guidelines
- ADVOR was a multicenter parallel-group, double blind randomized control trial published in NEJM 2022. It compared 519 patients with ADHF to acetazolamide vs placebo. Once randomized the oral diuretic was stopped, patients were placed on IV form of oral diuretic from home at double dose + 500mg IV of acetazolamide x 3 days (or to clinical decongestion) vs placebo.
- Primary outcome – successful decongeston at 3 days (defined by asence of clinical signs of volume overload other than trace peripheral edema. Assessed by cardiologist with decongestion score)
- Primary outcome of decongestion within 72 hours: 42.2% Acetazolamide group and 30.5% placebo group; RR 1.45 [95% CI1.17-1.82 P<0.001]
- Limitations
- The Lasix dose in the ACTZ was higher than the placebo group (80mg IV vs 60mg IV)
- Cardiology perspective
- Local cardiology perspective – acetazolamide has no role in the ED, increase furosemide doses rather than adding second line agent.
- Administration of furosemide early
BOTTOM LINE
- Reach for furosemide early at 2x home dose in mg IV
- Give more!
- Renal injury is not directly caused by furosemide but rather an incorrect volume assessment
- Faster relief of dyspnea
- Acetazolamide is not quite useful in ED, but your admitted patients may receive this while in hospital
Continuation of Goal Directed Medical Therapy in admitted patients with mild BP drop or mild AKI
- Why is this relevant to Emergency Medicine? Well, in many centres EM physicians are writing holding orders or admissions orders. EM junior residents are also writing admission orders in larger academic centres.
- Continuation of oral GDMT during hospitalization for heat failure has been shown in registries to:
- Decrease risk of post-discharge death
- Lower readmission rates
- Initiation of oral GDMT during hospitalization for HF is associated with numerous clinical outcome benefits:
- Betablockers
- Particularly important for patients with HFpEF, there diastolic dysfunction requires a prolonged filling time which is facilitated by betablockers.
- In OPTIMIZE–HF (2007)– discontinuation of beta blockers was associated with a higher risk of mortality (at 60-90 days) (HR 0.46 (95% CI = 0.30-0.73, p 0.0006) and higher rate of rehospitalization (the other primary endpoint) – OR 0.71 (95% CI = 0.53-0.94) p=0.0175.
- When to hold betablockers
- Marked volume overload (Allow for higher inotropy permitting safer therapy with aggressive diuretics (ie. Patient with cardiorenal syndrome, flash pulmonary edema)
- Advanced degree atrioventricular block in the absence of pacemakers
- Bradycardia
- Hypotension (from patient’s baseline but recognize that many patients with HF live with a lower BP compared to general population)
- ACEI/ARB
- ACEI/ARB are excellent afterload reduction agents and our 2 main goals in heart failure is afterload reduction and diuresis.
- It was also noted in the guideline’s supporting literature that a ACEI/ARB are safe to continue despite rises of Cr (up to >20% decrease in GFR) was not associated with AKI
- The guidance heart failure registry (GWTG–HF, 2017) showed that withdrawal of ACEI/ARB was associated with higher rates of post-discharge mortality and readmission.
- When do I hold home ACEI/ARB?
- Hypotensive (from patient’s baseline)
- Angioedema
- AKI
- Spironolactone
- It was also shown that continuing this medication decreases 30 day mortality and re-hospitalization in the COACH–HF trial (2014)
- Betablockers
BOTTOM LINE
- GDMT at discharge is important for lower mortality and readmission rates
- Our role is to continue medications while in the ED, or at admission when there are no contraindications.
- The majority of our stable CHFe patients will be able to continue all their GDMT therapy and this will help with your end goal of afterload reduction and diuresis
SGLT2 Inhibitors are now recommended amongst all states of heart failure
- SGLT2 inhibitors are now recommended for use in all stages of heart failure. The prevalence of ED patients taking these medications will continue to increase.
- Sodium-glucose cotransporter 2 inhibitors optimized the management of heart failure by diuresis, blood pressure reduction, inflammation reduction and improved cardiac energy metabolism. The exact mechanism is not clearly understood.
- The complications of SGLT2 inhibitors are relevant to emergency medicine. Keep in mind that these patients scan present with:
- Infection
- UTI
- Urosepsis/pyelonephritis
- Fournier’s gangrene
- Hypotension
- AKI
- Diabetic ketoacidosis
- Infection
- Euglycemic DKA
- SGLT2 inhibitors increase the risk of DKA by 3 folds
- In several studies, SGLT2 inhibitors were associated with euglycemic DKA (plasma glucose < 250mg/dL)
- The absence of substantial hyperglycemia can certainly delay recognition.
- The important point to remember is the patient will continue to have ketones, acidosis, AG. You can rely on those additional diagnostic criteria for recognition:
- Typical DKA diagnosis
- pH < 7.3 or bicarb < 15
- Ketones
- Plasma glucose > 13 or 11 mmol/L (depending on where you look)
- Typically, euglycemia DKA will still be above this, but not always
- Typical DKA diagnosis
BOTTOM LINE
- Recommended to verify for ketones in a patients with SGLT2 inhibitor if nausea/vomiting
- Patient who are unwell (decreased oral intake, N/V, malaise) should withhold therapy to prevent DKA
- Should be discontinued if acidosis is confirmed
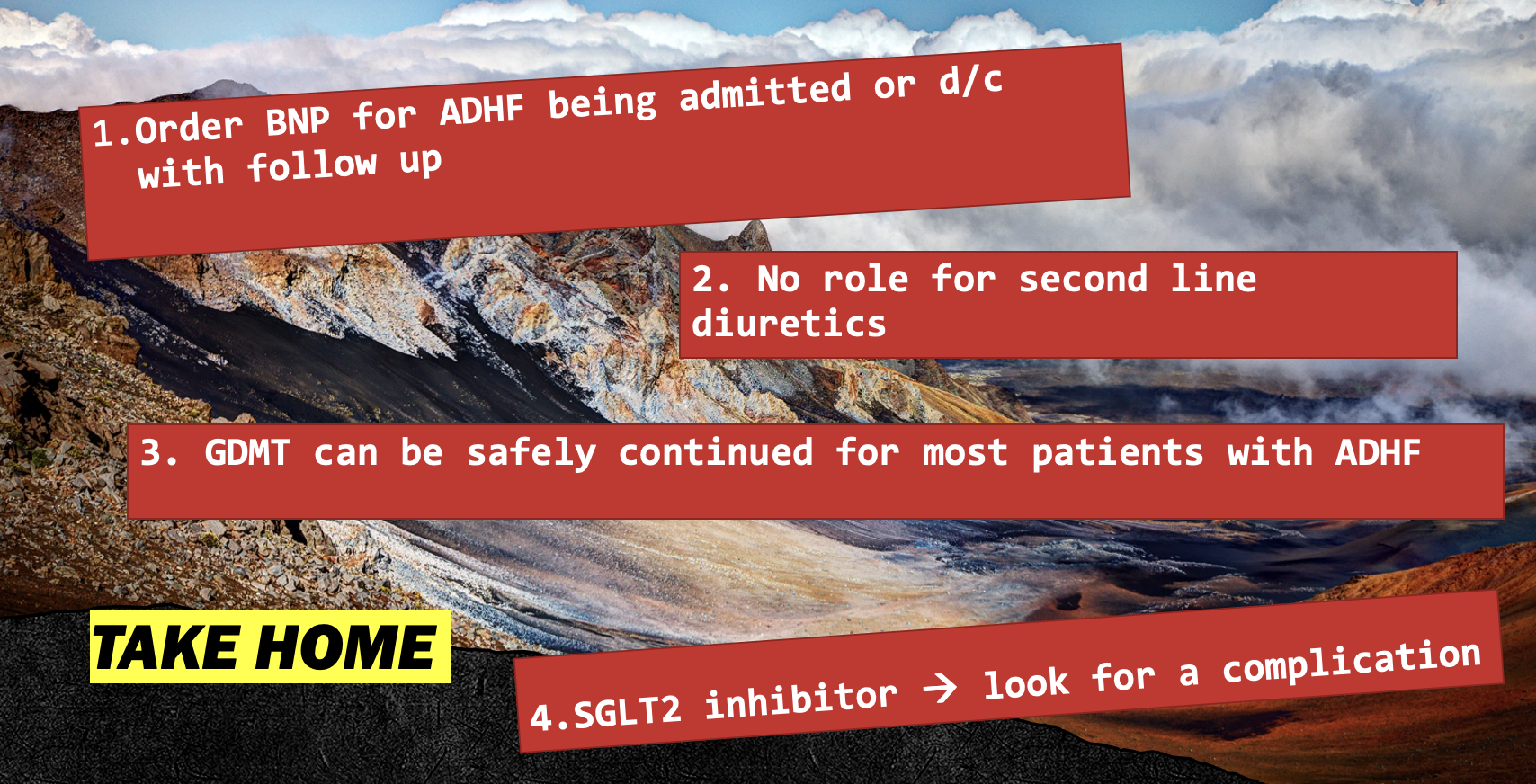
TAKE HOME POINTS
- Order BNP for patients with ADHF and considering ordering if discharging home to help guide patient’s outpatient management with cardiologist
- Furosemide remains our main diuresis agent, there is likely no role for acetazolamide in the ED
- Don’t be afraid to provide larger doses of Lasix
- Most commonly, you can continue GDMT once patient is admitted to hospital for ADH
- Euglycemic DKA is a thing, don’t miss it.
References
- , R., Moertl, D., Peter, S. (2010). N-terminal Pro-BNP guided intensive patient management in addition to multidisciplinary care in chronic heart failure: A 3 arm prospective randomized pilot study. Journal of the American College of Cardiology. 55(7). p.645-653.
- Destantis, A., Nathan, D., Rubinow, K. (2023). Sodium-glucose cotransporters 2 inhibitors for the treatment of hyperglycemia in type 2 diabetes mellitus. Retrieved on Up to date April 10th, 2023: https://www.uptodate.com/contents/sodium-glucose-cotransporter-2-inhibitors-for-the-treatment-of-hyperglycemia-in-type-2-diabetes-mellitus?search=sglt2%20inhibitors&source=search_result&selectedTitle=2~125&usage_type=default&display_rank=1
- Douros A, Lix LM, Fralick M, Dell’Aniello S, Shah BR, Ronksley PE, TremblayÉ, Hu N, Alessi-Severini S, Fisher A, Bugden SC, Ernst P, Filion KB, Canadian Network for Observational Drug Effect Studies (CNODES) Investigators. Sodium-Glucose Cotransporter-2 Inhibitors and the Risk for Diabetic Ketoacidosis : A Multicenter Cohort Study. Ann Intern Med. 2020;173(6):417. Epub 2020 Jul 28.
- Felker, G., Lee K, Bull D, et al. Diuretic strategies in patients with acute decompensated heart failure (2011). New England Journal of Medicine. 364(9). p.797-805.
- Fonaro, G., Stough, W., Abraham, W. (2007). Characteristics, treatments and outcomes of patients with preserved systolic function hospitalized for heart failure: A report from the OPTIMIZE-HF registry. (2007). Journal of the American Colege of Cardiology. 50(8). p.768-777.
- Flint, K., Allen, L., Pham, M. (2014). B-type natriuretic peptide predicts 30-day readmission for heart failure but not readmission for other causes. Journal of Maerican Heart Association. 3(3).
- Huelsmann M, Neuhold S, Resl M, et al. PONTIAC (NT-proBNP Selected PreventiOn of cardiac eveNts in a populaTion of dIabetic patients without A history of Cardiac disease) (2013). Journal of the American College of Cardiology. 62 (15) p.1365–1372.
- Heidenrech, Paul. Et al. (2022). 2022 AHA/ACC/HFSA Guidelines for the Management of Heart Failure: A Report of the American College of Cardiology /American Heart Associated Joint Committee on Clinical Practice Guidelines. Circulation. 145 (18).
- Ibrahim, N., Januzzi, J. (2018). The future of biomarker-guided thrapy for heart failure after the guiding evidence-based therapy using biomarker intensified treatment in heart failure (GUIDE-IT) study. Current Heart Failure Reports. 15(1) 37-43.
- Januzzi, J., Kimmenade, R., Lainchbury, J. et al. (2006). NT-proBNP for diangosis and short-term prognosis in acute destabilized heart failure: an international pooled analysis of 1256 patients: The International Collaborative of NT-pro BNP Study. European Heart Journal. 27 (3). P.330-337
- Kagiyama, N., Matsue, Y. (2018). The time-to-treatment concept in acute heart failure: Lessons and implications from REALITY-AHF. The Anatolian Journal of Cardiology. 20(2). 125-129.
- Maisel, A., Krishnaswarmy, P., Nowak, R. et al. (2002). Rapid measurement of B-type natriuretic peptide in the emergency diagnosis of heart failure. The New England Journal of Medicine. 347.p161-167.
- Maisel, A., Silver, Marc., Yancy, C. (2004). BNP Consensus Panel 2004: A clinical approach for the diagnosis, prognostic screening, treatment monitoring and therapeutic roles of natriuretic peptides in cardiovascular diseases. Congestive Heart Failure. 10(5) p.1-30.
- Maisel, A., Xue, Y., Veldhuisen, D. et al. (2014). Effect of spironolactone on 30-day death and heart failure rehospitalization (from the COACH study). The American Journal of Cardiology. 114(5). p.737-742.
- Matsue Y et al. Time-to-Furosemide Treatment and Mortality in Patients Hospitalized With Acute Heart Failure. JACC 2017. PMID: 28641794
- Mullen, W., Dauw, J., Martens, P. et a. (2022). Acetazolamide in decompensated heart failure with volume overload trial (ADVOR) : baseline characteristics. European Journal of Heart Failure. 24(9).1601-1610.
- Sanam, K., Bhatia, V., Nawkaranbir, S. et al. (2016). Renin-angiotensin system inhibition and lower 30-day all-cause readmission in medicare beneficiaries with heart failure. The American Journal of Medicine. 129(10). 1067-1073.
- Sanders-van Wijk, S., Van Empel, N., Davarzani, M. (2015). Circulating biomarkers of distinct pathophysiological pathways in heart failure with preserved vs. reduced left ventricular ejection fraction. European Journal of Heart Failure. 17(10).1006-1014.
- Salim Rezaie, “Door to Furosemide (D2F) in Acute CHF…Really?”, REBEL EM blog, November 27, 2017. Available at: https://rebelem.com/door-to-furosemide-d2f-in-acute-chfreally/.
- Stienen, S., Salah, K., Moons, A. (2018). NT-proBNP guided therapy in acute decompensated heart failure. 137(16). p.1671-1683.
