

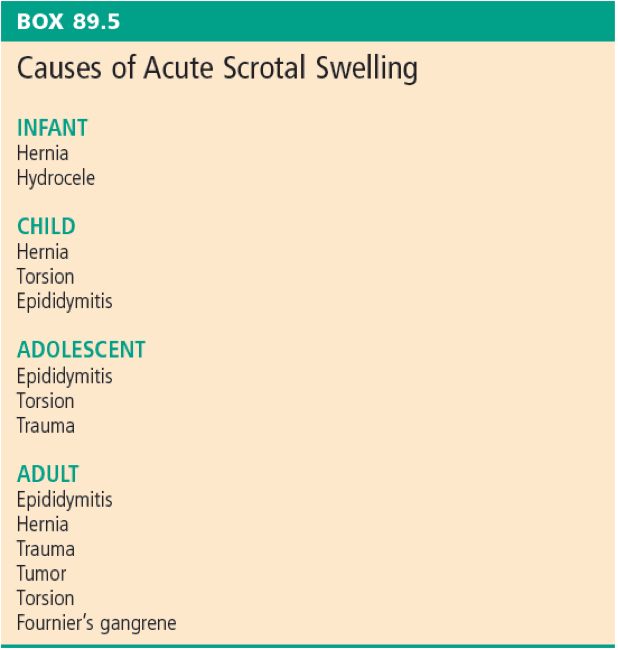
Acute scrotal pain is a common in emergency departments, comprising ~ 0.5% of all presentations. However, torsion is another very time sensitive diagnosis that is ubiquitous across all ages as seen by this Rosen’s table.
Incidence / Epidemiology
Unfortunately, epidemiological data is poor. Acute scrotal complaints make up approximately 0.5% of all ED visits and is estimated that annual incidence of testicular torsion is 1 in 4000 visits. Testicular torsion occurs more commonly in the first 25 years of life and incidence drops off as age increases. Zhao et al identified estimates of 3.8 per 100, 000 for patients < 18 years old16 and a 2020 cohort study by Greear et al reported adult incidence ranging from 10 -56%. 17
One thing that I want to mention up front and potentially debunk a myth that has been held about timing to intervention on testicular torsion is the 6-hour cut-off that has been thrown around for so many years and is likely still taught in med school. The 6-hour rule is an absolute figure for near 100% salvageability of the torsed testis. Mellick et al produced a systematic review in 2019 including 30 studies that outlined survival rates subdivided by time from onset of torsion/pain.18 What he wants to impress upon us as clinicians and by extension our non-physician colleagues seeing patients at triage, is that there is still worthwhile intervention that can potentially result in testicular survival up to 48 hours. Do not be a testicular torsion therapeutic nihilist!
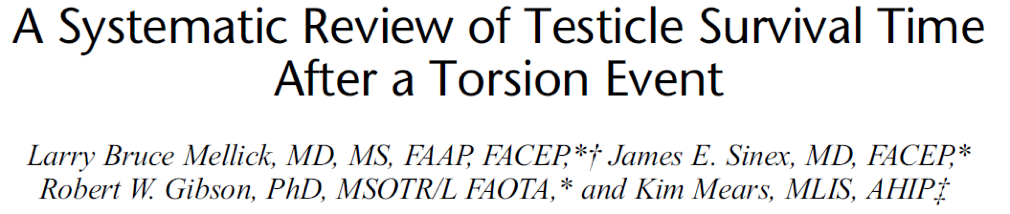
Unfortunately, older males typically present much later and thereby have much lower salvage rates than pediatric cases.
Etiology/Pathophysiology
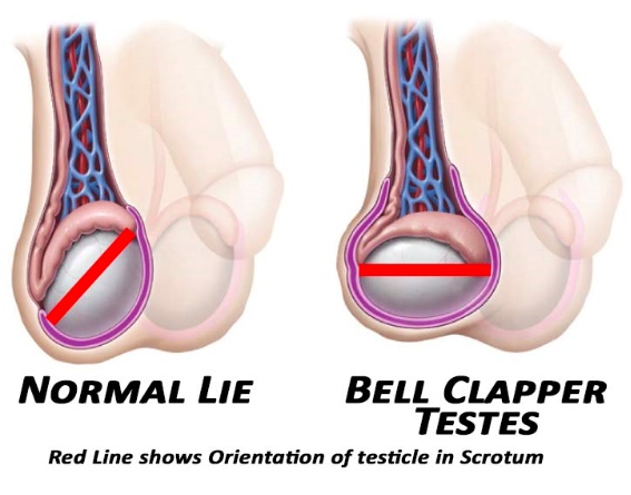
The majority of cases of testicular torsion are the result of the bell-clapper deformity, which is a congenital horizontal lie of the testicular that is the result in a defect in the gubernaculum as it pulls the testicle from the abdominal cavity through the tunica vaginalis and into the scrotum. However, minor trauma, vigorous activity, or an incident during sleep can result in the testicle rotating at the end of the spermatic cord’s axis, eventually resulting in ischemia and downstream effects.
Diagnosis
Exam
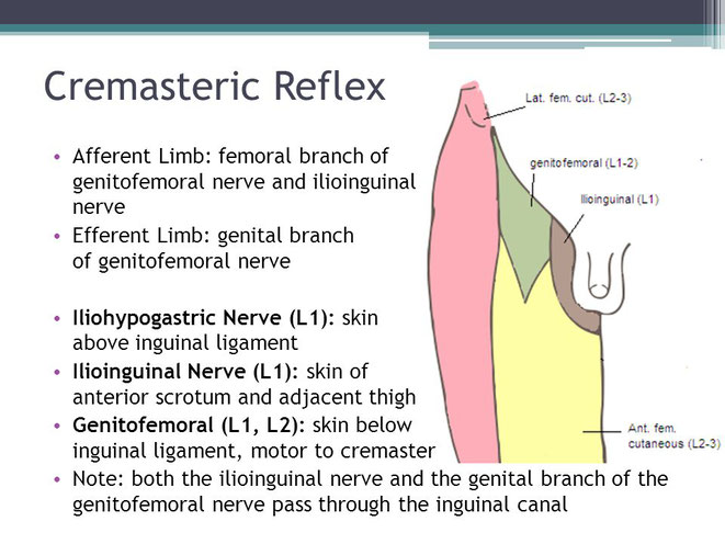
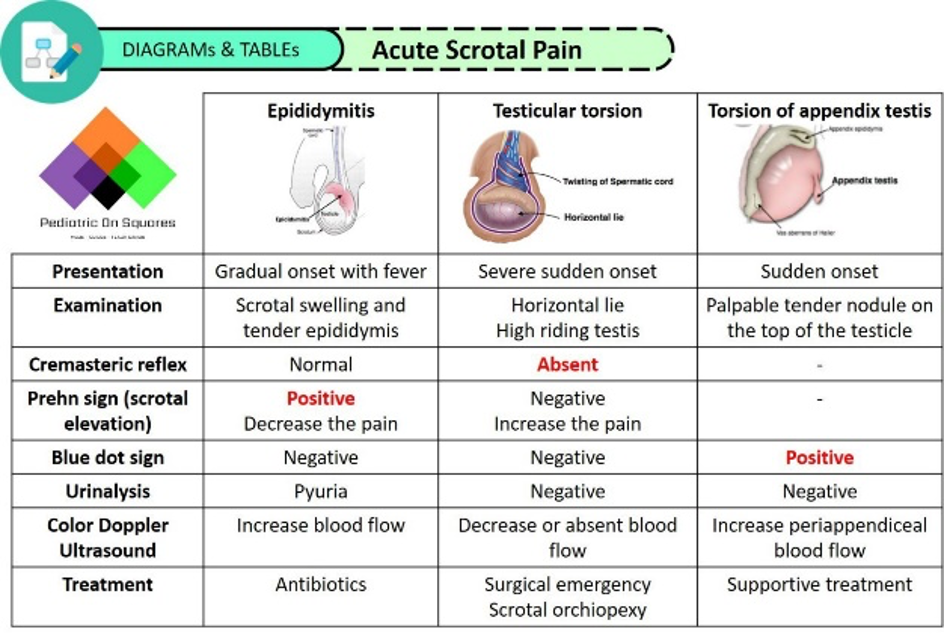
Physical examination is going to be one of the most important parts of diagnosing testicular torsion before doppler imaging. The cremasteric reflex and Prehn’s sign have long been considered pathognomonic for diagnosis of testicular torsion, however, these examination techniques are, practically speaking, not exceptionally helpful. Here is a quick refresher on how to properly illicit these two reflexes.
For the cremasteric reflex, you should expose the patient to be able to freely see the movement of both testicles and the medial thighs. Then, using a gloved hand or object, the clinician strokes along the L1-L2 cutaneous nerve distribution. A normal reflex should result in an elevation of the testis within the scrotum.
Prehn’s sign is used to help differentiate the etiology of the acute scrotal pain. The maneuver is performed simply by elevating the suspected testis in the scrotum, determining if the patient’s pain worsens or improves. Conceptually, if the pain is relieved with testicular elevation (a positive Prehn’s sign), it is believed the pain is more likely due to epididymitis. If Prehn’s is negative, then this would more likely point to testicular torsion. However, there do not appear to be any studies that confirms this correlation and, in fact, a 2018 paper by Roth et al reported an odds ratio of 5.9 in favour of a positive Prehn’s in confirmed testicular torsion compared to confirmed genital/paragenital infections.19 Don’t rely on Prehn’s sign.
What is more useful is what you would expect simply from the presentation of acute scrotum: testicular tenderness, redness, swelling, and possibly some retraction of the affected testicle, which you will then pair with history and imaging investigations.
Twist Score
The Testicular Workup for Ischemia and Suspected Torsion (or TWIST) score score was initially derived and validated in the pediatric population by Barbosa et al in 201320 and then later externally validated by Sheth et al in 2016.21 Barbosa prospectively evaluated 338 patients < 18 years old with acute scrotum, of whom 51 had testicular torsion. All patients were examined by a urologist and all underwent scrotal ultrasound. They identified 5 features that were consistent across those who were diagnosed with testicular torsion and attributed point values, identifying those that were low or high risk.
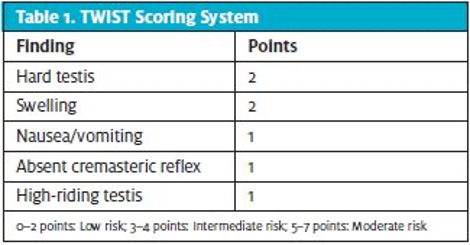
Two points were allocated to each “testicular swelling” and “hard testicle and one point was allocated to each “absent cremasteric reflex”, “presence of nausea/vomiting”, and “high-riding testis”. Patients with score < 2 were considered low risk and those with score > 5 were considered high risk. For the low-risk cut-off of 2, negative predictive value and sensitivity were both 100%. For the high-risk cut-off of 5, both positive predictive value and specificity were both 100%. Barbosa recommended against ultrasound for the low risk group and direct surgical consultation for exploration for the high risk group, effectively decreasing the need for scrotal ultrasound in 80% of patients with acute scrotum. They acknowledge some limitations of their study, i.e., physiologic absence of cremasteric reflex in younger children, inability to clarify other differential diagnoses, especially among the low risk patients. A last limitation, not entertained by Barbosa, is that the TWIST exam findings were all reported by urologists, not emergency providers, potentially limiting its utility.
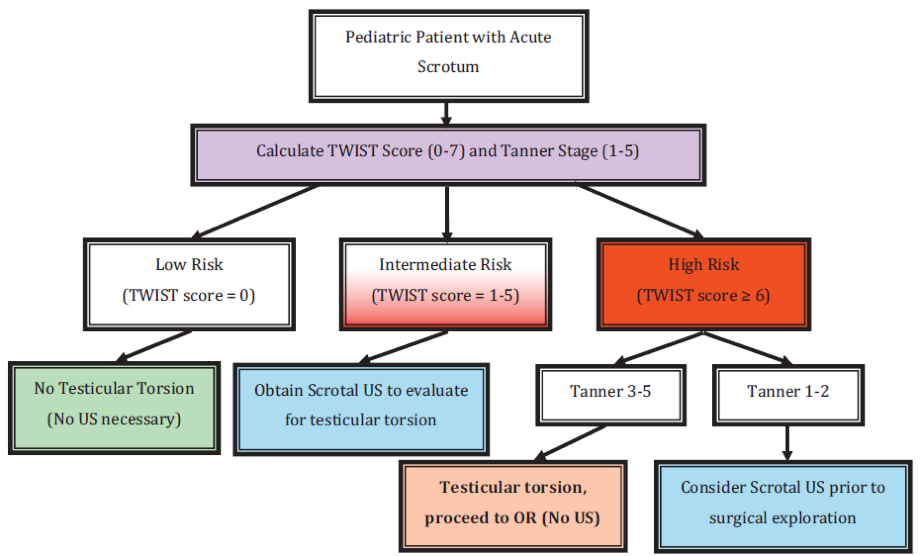
Sheth et al sought to validate the performance of the TWIST score among non-physician medical professionals, using emergency medical technicians (EMTs) to apply the score to a total of 128 patients between the ages of 1 month and 21 years. As with Barbosa’s initial study, all patients had a diagnostic ultrasound performed and for those without torsion, all were offered urologic follow up in 2 weeks. They also performed subgroup analysis using varying Tanner stages of development. They found that their population required cut-offs of 0 for low risk and 6 for high risk, with NPV of 100% and PPV of 93.5% respectively. Subgroup analysis of Tanner stages 3-5 had PPV of 100% for score ≥ 6 but only 78% for Tanner stages 1-2, suggesting that the TWIST score may be more challenging to apply to prepubertal children. There were 3 patients reported to have a score of 1, who were positive for torsion and required surgical intervention, contrasting the results in Barbosa’s paper. Sheth believes that, as these scores were determined by EMTs, their suggested cut-offs, and the following algorithm are more appropriate for use in the ED than the original score by Barbosa. The authors propose that this new algorithm could reduce need for diagnostic ultrasound by 54.5%, notably lower than the 80% proposed by Barbosa.
The true reliable cut-offs for ruling out or ruling in testicular torsion are uncertain. Frolich prospectively validated the score in 2017, identifying low-risk as having a TWIST score of 0 or 1 and high risk patients with a score of 7.22 Manohar et al collected retrospective data and reported mean TWIST scores for those with confirmed testicular torsion at 4.75 (range 2-7) whereas those without torsion had mean scores of 1.46 (range 0-5).23
There were two systematic analyses published by Qin in 2022 and Choudhury in 2023 that seem to further support the risk groups as presented by Sheth. Qin extracted 13 prospective and retrospective studies, including 527 cases of testicular torsion, and reported pooled sensitivity and specificity of 0.993 and 0.069, respectively for a TWIST score of zero. For a TWIST score of 7, the pooled sensitivities and specificities were 0.276 and 0.994, respectively. Qin concluded that while Barbosa’s cut-offs were more reliable with an AUC of 0.924 and only required ultrasound in 19.9% of patients, Sheth minimized both missed torsion cases (0.6 vs 1.6 per 100 presentations) and unnecessary surgical exploration (1.6 vs 2.5 per 100 presentations).24
Validation in Adults
But what about our population? What about adults? In 2021, Barbosa collected prospective data on 81 patients > 16 years of age who were evaluated by a surgeon in the ED for acute scrotum, of which 68 were included in the analysis. The same cut-offs as his original TWIST paper were used: 0-2 for low risk, 3-4 for intermediate, and 5-7 for high risk and all had diagnostic ultrasound. 50% of patients were diagnosed with torsion. A score of 2 or less had NPV of 100% for TT but a score 5 or greater had sensitivity of 79% and PPV of 91%. If high risk cut-off was moved to 6 or greater, PPV became 100%. Barbosa concluded that the score performed similarly to the original paper but that increasing the high-risk cut-off to 6 or greater had higher PPV.25
Ultimately, I would say that in both pediatric and adult populations, the safest approach would be the algorithm proposed by Sheth et al., albeit requiring ~ 25% more diagnostic ultrasounds.
Ultrasound/PoCUS
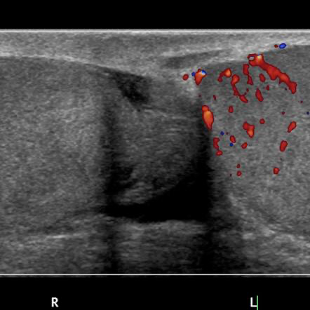
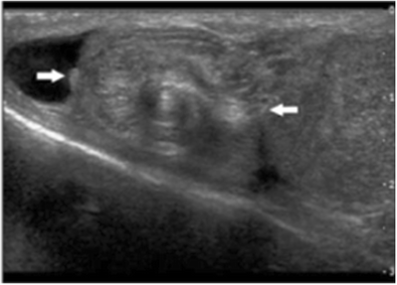
Doppler ultrasound is considered the GOLD STANDARD test for diagnosis of testicular torsion before actual surgical exploration. Testicular torsion should be high on the differential if there is evidence of decreased or absent blood flow in the affected testicular compared to the contralateral side, as well as testicular edema, heterogenous echopattern, increased testicular and epidydimal size, reactive hydrocele, or the whirlpool sign.
A systematic review published in 2021 by McLaren et al evaluated 5 studies that included acute scrotum patients of all ages, reported utilization of B-mode and colour doppler, patients who underwent surgical exploration, and reported positive/negative testicular torsion cases. Unfortunately, the studies did not report level of training for those completing or interpreting. They reported that when B-mode and colour doppler modes were used in combination, the five studies reported a sensitivity between 81-100% and accuracy between 90 – 98%.28
So how well do emergency physicians with access to point of care ultrasound (POCUS) do in making this diagnosis? There are several researchers that have published on this topic but I’d like to highlight just a few.
Friedman et al completed a retrospective chart review of 120 pediatric patients with acute scrotum over a three-year period who had recorded POCUS diagnosis and subsequent radiology performed ultrasound diagnosis within 24 hours. In addition to torsion, they collected findings for 8 other diagnoses. They determined that the across all diagnoses, all POCUS users made the diagnosis with a mean 70% accuracy, and up to 79% for those who had completed PED POCUS fellowships. However, torsion was the only diagnosis in which there were 100% agreement with final diagnosis. 29
On a much smaller scale, Koppel et al conducted a retrospective case review of 73 cases, of which all underwent orchiopexy and 23 of which had POCUS preoperatively. All POCUS images were obtained by PEM fellows or attendings, some of which had completed a PEM POCUS fellowship. As with the Friedman study, POCUS was diagnosed torsion with 100% accuracy and even prompted attempt at manual detorsion in 3 cases prior to urology assessment. They also reported a median length of stay from ED admission to orchipexy of 184 minutes for the radiology only ultrasound and 121 minutes for POCUS.30 Although the numbers here or low, this reinforces the accuracy of POCUS for identifying torsion, and in some centres, may expedite time to surgical correction.
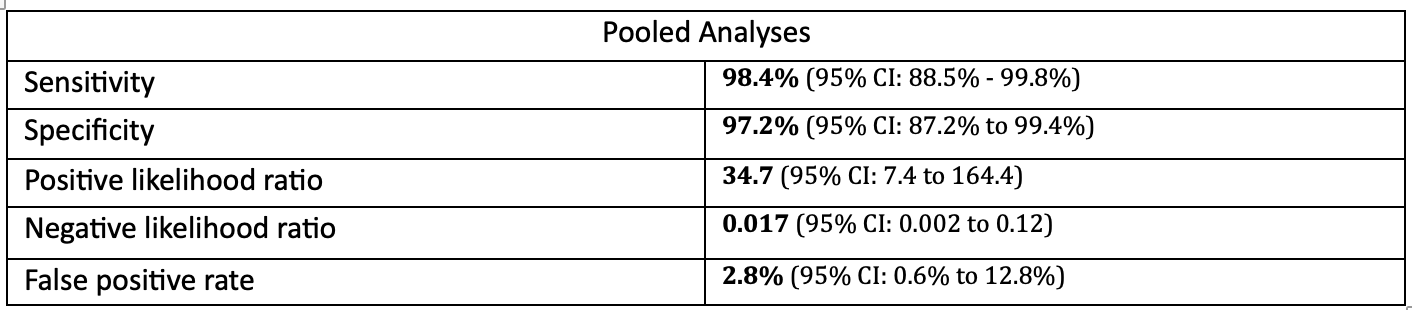
Lastly, a systematic review and meta-analysis by Mori et al further reinforces the accuracy of POCUS examination in the pediatric realm.31 They included 4 studies with a total of 784 patients, of which pooled sensitivity, specificity, positive and negative likelihood ratios, and false positive rate were as follows:
Just as a refreshed for how to most efficiently perform, here is a short video by EM:RAP:– I skip the M-mode part as this is more technically difficult and unnecessary in most cases. With that said, I think that everyone should be adding POCUS to their clinical examination if torsion is suspected as it will likely enable you to call urology before the patient can get to radiology performed ultrasound.
ED Management
Open-Book Detorsion
So now that you’ve diagnosed testicular torsion, apart from calling urology, what should we do next? The answer to that question is, it depends. It depends on where you are working, if you have access to urology at your site, or if you’re in a community hospital with expected prolonged transport times to a centre with urology in house.
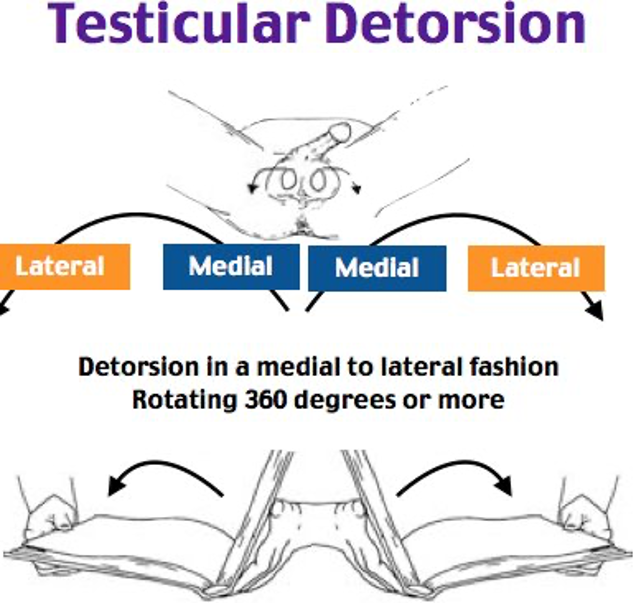
The recommended approach to detorsion is described as the “open-book” detorsion method. The majority of sponatneously torsed testicles are typically rotated internally, i.e. lateral to medial direction, counter clockwise for the left testicle, clockwise for the right testicle. This is often a very painful procedure just by virtue of presenting testicular tenderness so analgesia should be administered if possible, however, sedating the patient would be ill-advised as you won’t be able to verify pain relief.
Vasconcelos-Castro et al conducted a retrospective case series of 122 patients in which manual detorsion was attempted in 58 (48%). Successful detorsion was defined as relief of pain or return of blood flow on colour doppler ultrasound. Of those patients who underwent attempted manual detorsion, 18% had presented to ED > 6 hours from pain onset and 6% > 24 hours. 26% had both complete pain relief and normal colour doppler after manual detorsion and there was NO gonadal loss or testicular atrophy during follow up. 10 out of 15 of these patients were able to undergo non-emergency bilateral orchiopexy within 24 hours and 5 had elective orchiopexy within 3-21 days after manual detorsion. 26% had residual cord torsion on surgical exploration occurred in those with either incomplete pain relief or persistently abnormal colour doppler ultrasound. Among these patients, 5 experienced atrophy at follow up, despite surgical detorsion, and subsequently gonadal loss. Lastly, of the 64 patients (52%) of patients that did not undergo manual detorsion, 28 had testicular loss despite attempt at surgical correction.32
Filho et al reported their own retrospective review of 133 patients eventually treated for testicular torsion, among which 57% had manual detorsion attempted preoperatively. They were all assessed within 24 hours Of those who had manual detorsion attempted, only 2 patients required orchiectomy compared with 15 of the 61 (24.6%) who did not undergo manual detorsion. They also performed a logistic regression, reporting an odds ratio (OR) of 17.38 for testicular salvage among those who had manual detorsion. Filho does argue that there may be a selection bias for manual detorsion among patients who have less edema or pain and thereby may have arguably had more favourable outcome from the beginning. They also advocate for repeat doppler ultrasound to confirm or monitor manual detorsion attempts.33
I was unable to find any larger studies, however, there were a couple of case reports that described successful manual detorsion using concurrent testicular POCUS to confirm reperfusion of the affected testicle. In each of them, manual detorsion was attempted in stages and reassessed with POCUS to correlate relief of pain with reperfusion.34,35
Traction Detorsion
Larry Mellick, a pediatric emergency physician in the US wrote a letter to the editor of Pediatric Emergency Care, describing a modified approach to manual detorsion, which he proposes could promote more uptake on manual detorsion among emergency providers. He suggests a hesitancy among EPs to attempt the procedure for fear of worsening the condition, as approximately 30% of spontaneous torsion rotates externally. He proposes to add a component of downward traction to the affected testicle to first observe if it tends to detorse in one direction or another before attempting either internal or external rotation.36 Just envision an telephone cord, recognizing that if it’s pulled straight it will often be easier to untangle.
..Or should we just call Urology?
Dr. Matthew Roberts, Program Director and Assistant Professor of Urology at the University of Ottawa, recommends that if we have a strong clinical suspicion for testicular torsion, even prior to ultrasound, we should feel comfortably consulting his team. Ultrasound still remains a diagnostic mainstay, however, time to urologic assessment should be minimized if there is strong evidence pointing towards testicular torsion. Perhaps this could be one of the next ED-surgical relationships that could be fostered by our POCUS group, especially on ultrasound off-hours. Detorsion, I think, should be attempted but not if it will result in delay to definitive care by our urologist colleagues. Where I think it could really shine as an ED procedure is if you expect delay in transport from a peripheral hospital and can potentially decrease ischemia time, resulting in high rates of salvage.
References
- Roghmann F, Becker A, Sammon JD, et al. Incidence of Priapism in Emergency Departments in the United States. The Journal of Urology. 2013;190(4):1275-1280.
- Eland IA, van der Lei J, Stricker BHC, Sturckenboom MJCM. Incidence of priapism in the general population. Urology. 2001;57(5):970-972.
- Salonia A, Bettochi C, Capogrosso P, et al. EAU Guidelines on Sexual and Reproductive Health. Edn. presented at the EAU Annual Congress of Milan 2023. European Association of Urology; 2023.
- Dean RC. Physiology of Penile Erection and Pathophysiology of Erectile Dysfunction. Published online 2006.
- Idris IM, Burnett AL, DeBaun MR. Epidemiology and treatment of priapism in sickle cell disease. Hematology. 2022;2022(1):450-458. doi:10.1182/hematology.2022000380
- Sangiorgi G, Cereda A, Benedetto D, et al. Anatomy, Pathophysiology, Molecular Mechanisms, and Clinical Management of Erectile Dysfunction in Patients Affected by Coronary Artery Disease: A Review. Biomedicines. 2021;9(4):432. doi:10.3390/biomedicines9040432
- Ahuja G, Ibecheozor C, Okorie NC, et al. Priapism and Sickle Cell Disease: Special Considerations in Etiology, Management, and Prevention. Urology. 2021;156:e40-e47. doi:10.1016/j.urology.2021.06.010
- Ericson C, Baird B, Broderick GA. Management of Priapism 2021 Update. Urol Clin N Am. 2021;48(4):565-576.
- Wakrim S, Ziouziou I, Ralph D, Khabbal Y. Penile Doppler ultrasound study in priapism: A systematic review. Progrès en Urologie. 2022;32(1):61-69. doi:10.1016/j.purol.2021.03.009
- Gravel J, LeBlanc C, Varner C. Management of priapism with a trial of exercise in the emergency department. CJEM. 2019;21(1):150-153. doi:10.1017/cem.2018.3
- Moussa M, Abou Chakra M, Papatsoris A, et al. An update on the management algorithms of priapism during the last decade. Arch Ital Urol Androl. 2022;94(2):237-247. doi:10.4081/aiua.2022.2.237
- Bobo GA, Almajed W, Conlon J, Morenas RA, Hellstrom WJG. An overview of emergency pharmacotherapy for priapism. Expert Opinion on Pharmacotherapy. 2022;23(12):1371-1380. doi:10.1080/14656566.2022.2099271
- Martin C, Cocchio C. Effect of phenylephrine and terbutaline on ischemic priapism: a retrospective review. The American Journal of Emergency Medicine. 2016;34(2):222-224. doi:10.1016/j.ajem.2015.10.029
- Ridyard DG, Phillips EA, Vincent W, Munarriz R. Use of High-Dose Phenylephrine in the Treatment of Ischemic Priapism: Five-Year Experience at a Single Institution. The Journal of Sexual Medicine. 2016;13(11):1704-1707. doi:10.1016/j.jsxm.2016.09.010
- Siegel J, Rich M, Brock W. Association of sickel cell disease, priapism exchange transfusion and neurological events: ASPEN syndrome. Journal of Urology. November1993;150(5):1480-1482.
- Zhao LC, Lautz TB, Meeks JJ, Maizels M. Pediatric Testicular Torsion Epidemiology Using a National Database: Incidence, Risk of Orchiectomy and Possible Measures Toward Improving the Quality of Care. Journal of Urology. 2011;186(5):2009-2013. doi:10.1016/j.juro.2011.07.024
- Greear GM, Romano MF, Katz MH, Munarriz R, Rague JT. Testicular torsion: epidemiological risk factors for orchiectomy in pediatric and adult patients. Int J Impot Res. 2021;33(2):184-190. doi:10.1038/s41443-020-0331-8
- Mellick LB, Sinex JE, Gibson RW, Mears K. A Systematic Review of Testicle Survival Time After a Torsion Event. Pediatric Emergency Care. 2017;Publish Ahead of Print. doi:10.1097/PEC.0000000000001287
- Roth B, Giannakis I, Ricklin ME, Thalmann GN, Exadaktylos AK. An Accurate Diagnostic Pathway Helps to Correctly Distinguish Between the Possible Causes of Acute Scrotum. Oman Med J. 2018;33(1):55-60. doi:10.5001/omj.2018.10
- Barbosa JA, Tiseo BC, Barayan GA, et al. Development and Initial Validation of a Scoring System to Diagnose Testicular Torsion in Children. Journal of Urology. 2013;189(5):1859-1864. doi:10.1016/j.juro.2012.10.056
- Sheth KR, Keays M, Grimsby GM, et al. Diagnosing Testicular Torsion before Urological Consultation and Imaging: Validation of the TWIST Score. Journal of Urology. 2016;195(6):1870-1876. doi:10.1016/j.juro.2016.01.101
- Frohlich LC, Paydar-Darian N, Cilento BG, Lee LK. Prospective Validation of Clinical Score for Males Presenting With an Acute Scrotum. Zonfrillo MR, ed. Acad Emerg Med. 2017;24(12):1474-1482. doi:10.1111/acem.13295
- Manohar C, Gupta A, Keshavamurthy R, Shivalingaiah M, Sharanbasappa B, Singh V. Evaluation of testicular workup for ischemia and suspected torsion score in patients presenting with acute scrotum. Urol Ann. 2018;10(1):20. doi:10.4103/UA.UA_35_17
- Qin KR, Qu LG. Diagnosing with a TWIST: Systematic Review and Meta-Analysis of a Testicular Torsion Risk Score. Journal of Urology. 2022;208(1):62-70. doi:10.1097/JU.0000000000002496
- Barbosa JABA, De Freitas PFS, Carvalho SAD, et al. Validation of the TWIST score for testicular torsion in adults. Int Urol Nephrol. 2021;53(1):7-11. doi:10.1007/s11255-020-02618-4
- Boettcher M, Bergholz R, Krebs TF, Wenke K, Aronson DC. Clinical Predictors of Testicular Torsion in Children. Urology. 2012;79(3):670-674. doi:10.1016/j.urology.2011.10.041
- Klinke M, Elrod J, Stiel C, et al. The BAL-Score Almost Perfectly Predicts Testicular Torsion in Children: A Two-Center Cohort Study. Front Pediatr. 2020;8:601892. doi:10.3389/fped.2020.601892
- McLaren PSM. A systematic review on the utility of ultrasonography in the diagnosis of testicular torsion in acute scrotum patients. Radiography. 2021;27(3):943-949. doi:10.1016/j.radi.2020.12.012
- Friedman N, Pancer Z, Savic R, et al. Accuracy of point-of-care ultrasound by pediatric emergency physicians for testicular torsion. Journal of Pediatric Urology. 2019;15(6):608.e1-608.e6. doi:10.1016/j.jpurol.2019.07.003
- Koppel JH, Patt YS, Berant R. Point of Care Ultrasound for the Diagnosis of Pediatric Testicular Torsion: A Retrospective Case Series Analysis. Pediatr Emer Care. 2022;Publish Ahead of Print. doi:10.1097/PEC.0000000000002863
- Mori T, Ihara T, Nomura O. Diagnostic accuracy of point-of-care ultrasound for paediatric testicular torsion: a systematic review and meta-analysis. Emerg Med J. 2023;40(2):140-146. doi:10.1136/emermed-2021-212281
- Vasconcelos-Castro S, Flor-de-Lima B, Campos JM, Soares-Oliveira M. Manual detorsion in testicular torsion: 5 years of experience at a single center. Journal of Pediatric Surgery. 2020;55(12):2728-2731. doi:10.1016/j.jpedsurg.2020.02.026
- Dias Filho AC, Oliveira Rodrigues R, Riccetto CLZ, Oliveira PG. Improving Organ Salvage in Testicular Torsion: Comparative Study of Patients Undergoing vs Not Undergoing Preoperative Manual Detorsion. Journal of Urology. 2017;197(3 Part 1):811-817. doi:10.1016/j.juro.2016.09.087
- Smith W, Midgley S, Kummer T. Real-time Ultrasound-Guided Manual Testicular Detorsion: A Case Report. Clinical Practice and Cases in Emergency Medicine. 2022;6(3):248-251. doi:10.5811/cpcem2022.6.57256
- Nene RV, Subramony R, Marcias M, Campbell C, Aminlari A. Real-time Point-of-care Ultrasound for the Diagnosis and Treatment of Testicular Torsion. pocus. 2021;6(2):70-72. doi:10.24908/pocus.v6i2.15186
- Mellick L. The Torsed Tesicle Traction Technique and 2 Case Reports. Pediatric Emergency Care. 2023;39(5).

Thank you for shedding light on testicular torsion. The detailed explanation of symptoms and the importance of prompt treatment really emphasizes how crucial it is to seek medical attention quickly. This post is a great resource for raising awareness about such a serious condition!
Thank you for such an informative post on testicular torsion! I had no idea how critical it was to seek immediate medical attention and how quickly it can happen. This is a topic that definitely needs more awareness. I appreciate the detailed explanation and the emphasis on recognizing the symptoms early.
Thank you for shedding light on such an important topic! I appreciate the detailed information about the symptoms and the urgency of seeking treatment for testicular torsion. It’s crucial for everyone to be aware of this condition, especially young men. Your post could help save lives!
Thank you for shedding light on such an important topic! The detailed explanations and symptoms of testicular torsion were really helpful. I appreciate the emphasis on seeking immediate medical attention; it’s crucial for reducing the risk of complications. Great job on raising awareness!
This post is incredibly informative! I had heard of testicular torsion before, but your detailed explanation of the symptoms and the importance of seeking immediate treatment really opened my eyes. Thanks for raising awareness about such a crucial health issue!