

In this post, we will sink our teeth into some details around venomous snake bites that all emergency clinicians should be aware of regardless of their location of clinical practice. Although the incidence of venomous snake bites in Canada is rare, this should be considered a HALO (high acuity low occurrence) presentation for which you should be prepared and have a basic approach. This post will arm you with the current guidelines tailored to Canadian practice based on expert opinion from the Ontario Poison Center.
Part 1 – The Fangs – Epidemiology
There are over 3000 species of snakes with approximately 800 categorized as venomous with approximately 8-10,000 snake bites reported to Poison Control Centers annually in US and Canada [1,2]. The truth is that the absolute number of annual envenomations in Canada is quite small and may even be underreported in some areas for a variety of reasons. This may include having a well-established protocol/algorithm at an institution or even the lack of presentation to care because of black market venomous snake bites. For Canadian practice, there are 3 Crotalinae species which are limited to relatively narrow geographic areas in British Columbia, Alberta, Saskatchewan, and Ontario [2]. These pit vipers include (Crotalinae) the western rattlesnake (Crotalus oreganus), the prairie rattlesnake (Crotalus viridis), and the eastern massasauga rattlesnake (Sistrurus catenatus) (Figure 1). Although this is a rare occurrence, a venomous snake bite is known to result in significant morbidity and mortality.
Specifically in Ontario, the distribution of the Eastern Massasauga Rattlesnake is geographically distributed over the southern portions of Ontario. The majority of presentations in Ontario are from Owen Sound and Parry Sound where a more protocolized approach to venomous snake bites has been generated.

Figure 1: Geographical distribution of venomous snakes in Canada.
Notably, it is important to understand that there may be variations of snakes brought into the country or individuals who have illegal exotic pets. We will not be experts in the speciation of snakes, however, there are common physical features that will help you identify the likelihood of a snake being venomous (Figure 2).
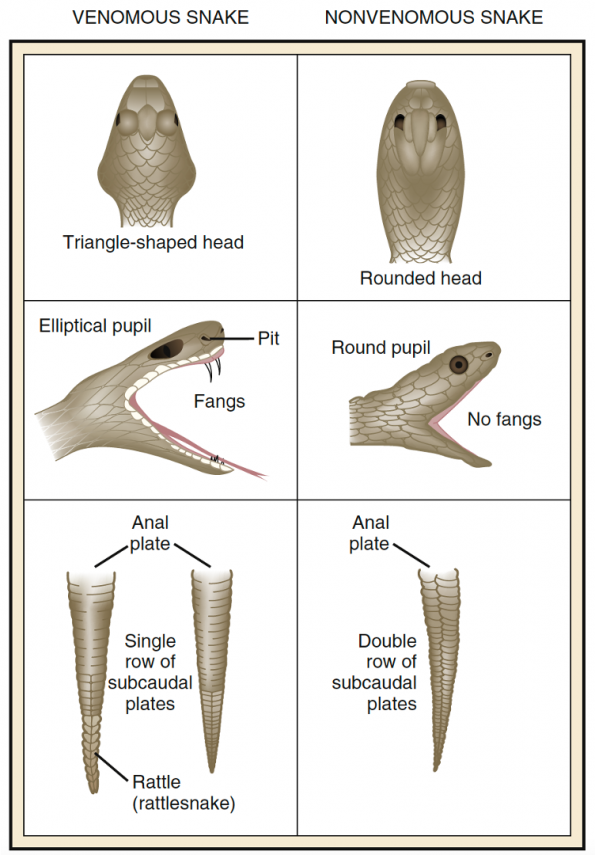
Figure 2: Physical features distinguishing venomous from non-venomous snakes [1].
 A final feature that is not captured in the above image includes the colouration of the snake which is specific to coral snakes. If red and yellow stripes are adjacent to each other, this suggests it is a venomous species. Other stripe variations whereby red and black stripes are adjacent indicates that it is a non venomous snake. We may also recall this by the classic rhyme as follows:
A final feature that is not captured in the above image includes the colouration of the snake which is specific to coral snakes. If red and yellow stripes are adjacent to each other, this suggests it is a venomous species. Other stripe variations whereby red and black stripes are adjacent indicates that it is a non venomous snake. We may also recall this by the classic rhyme as follows:
“Red and yellow, kill a fellow. Red and black, venom lack.”
Part 2 – The Guidelines
Although these presentations are quite rare, it is important to be aware of the general guidelines used for the treatment of venomous snake bites. In this section, we will review the clinical presentation and common antidotes with medical management used in the emergency department.
Pathophysiology
Before we get too far into the guidelines, let’s take a look at the pathophysiology of venom and how it impacts the body. Venom consists of a concoction of enzymes, polypeptides, and glycol proteins which work specifically in different manners. Depending on the contents of the venom, you can have either neurotoxic effects or hematologic effects on the body [3].
Generally, neurotoxicity is achieved by venom through phospholipase A2 neurotoxin which binds to the acetylcholine receptor at the motor end plate or in nerve endings preventing further release of the transmitter [3]. This presents clinically through cranial nerve dysfunction and skeletal muscle weakness. Over time, this can result in paralysis of the victim and subsequent respiratory failure with diaphragm involvement. These are the patients that you’re concerned about from a respiratory standpoint and when you would consider securing the airway. It is important to note that these are common findings in the Elapidae class of venomous snakes.
Hematologic effects start locally with necrotic and hemorrhagic blisters around the site of envenomation and then can result in systemic coagulopathy [3]. This is demonstrated through market thrombocytopenia and hypofibrinogenemia. These patients can deteriorate further and present with DIC.
Clinical Presentation
The challenge with snakebite management comes down to their variable clinical presentation. When assessing a patient who comes in with a suspected snakebite, it is important to assess their wounds to determine the possibility of systemic toxicity. The least severe presentation is what we refer to as a dry bite (Figure 3). This is noted in particular when you see puncture wounds on the skin with no surrounding hematologic or erythema effects. A more severe presentation concerning for possible progression is when you begin to see hemorrhagic blisters and local necrosis (Figure 4)

Figure 3: Dry bite from a snake. |

Figure 4: Local wound necrosis following a venomous snake bite. |
The initial workup in the emergency department is guided primarily by the neurotoxic and hematotoxicity effects of the venom. The crux to assessing neurotoxicity is through physical examination and assessment of respiratory status. Frequent assessment for coagulopathy with CBC, INR/PTT, and fibrinogen should be done every six hours for all patients except for when there is a high suspicion of a dry bite. Electrolyte disturbances are also common and we should monitor for signs of tissue breakdown through CK, lactate, and hyperkalemia.
The workup and management of venomous snake bites outlined in this post are derived from the Antivipmyn Treatment Package by Dr. KC Mills [4]. The link to the package can be found here. The steps for management are outlined in the following sections.
Management
There are a variety of medications that can be used to treat patients who have venomous snake bites. The most commonly documented medications include trypsin, lymphatic flow inhibitors and antivenoms. Trypsin is a proteolytic enzyme that breaks down the protein components of venom to either decrease potency or eliminate toxic effects [3]. This substance can be used in the absence of antivenom agents or in conjunction with anti-venom when there is a potent snake bite. In discussions with toxicologists at the OPC, this substance is no longer used given the efficacy and reasonable availability of antivenom. Another medication includes lymphatic flow inhibitors which are nitric oxide-releasing agents, such as glyceryl trinitrate, which decreases lymphatic spread thereby delaying time to toxicity [3]. Again, these substances have limited utility unless in a remote location where transport of the patient is not feasible and access to antivenom is limited. In summary, the mainstay to treatment of a venomous snake bite is antivenom which we will explore further in the coming segments.
Antivenom
There exist two types of antivenom that you should be aware of when working in the US or Canada. These include CroFab and Antivipmyn.
Currently, CroFab is approved for all North American crotalids whereas Antivipmyn is only approved for North American rattlesnakes due to immunoglobulin affinity for the venom [5]. Now as we previously discussed, rattlesnakes are what we will see most often in Canada and will be the main focus of this post. It is worth noting that there are a variety of antivenoms that exist worldwide and your practice should be tailored to the location and native species of snakes where you work.
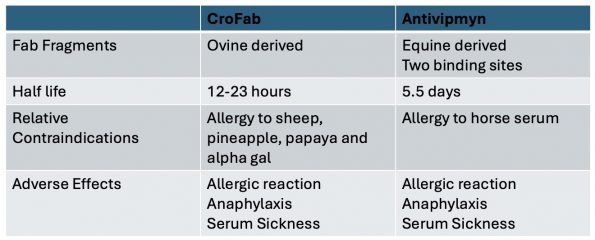
Table 1 summarizes a few basic differences between CroFab and Antivipmyn. CroFab is derived generally from ovine serums whereas Antivipmyn is from equine derivatives and has two distinct binding sites. This additional binding site allows for an even longer half-life of 5 ½ days whereas CroFab only has a half-life of 12 to 23 hours [5]. This element is very important when considering treating a patient in the emergency department and follow-up treatments. Notably, this longer half-life reduces rebound coagulopathy which is a common issue with shorter half-life derivatives. Generally, relative contraindications around anti-venom are focused on the known allergies of the individual receiving treatment. For example, Antivipmyn is relatively contraindicated when there’s an allergy to horse serum since this is where it’s derived whereas CroFab is contraindicated in the event of allergies to sheep serum, pineapple, papaya or alpha-gal [5]. That being said, these are relative contraindications since treatment can proceed but in a slightly different manner which we will discuss later. Overall, the adverse effects that you see following the use of anti-venom are the same between the two including allergic reaction, anaphylaxis, and serum sickness which we will discuss later on in this talk.
Table 1: Summary of differences between CroFab and Antivipmyn antivenoms.
Antivenom Fab fragments can bind to a variety of snake venoms. As such they are effective treatments for a multitude of different snakes within similar classes. This highlights the importance of identifying the snake or geographical region of where the bite took place so Ontario Poison Control can ensure that the antivenom they are providing you is effective.
The complete treatment algorithm with Antivipmyn is outlined in Figure 5 below [4]. Treatment with antivenom is guided by your clinical assessment and identification of the presence of pain and swelling to the bite site. If there is no pain or swelling in the area, this is when we suspect a dry bite. All patients would receive lab work to assess for coagulopathy. If there is clinical suspicion of a dry bite and lab work is normal, we repeat those labs again after six hours and can potentially discharge this patient home if they remain unremarkable. Should the workup return as abnormal, we consider further investigation and subsequent treatment with antivenom. If the patient has pain and swelling right from the start this is when we would order stat labs and determine the level of envenomation which dictates the amount of anti-venom we would use for treatment.
Envenomation level is broken down into three distinct categories which is based on clinical assessment and laboratory findings [4]. Minimal envenomation is defined by minimal pain and swelling, or minimal and absent coagulopathy, where the INR is less than 1.5. In this instance, we can continue to observe and consider treatment if they progress. Modern envenomation is defined by moderate findings of pain and swelling in addition to mild coagulopathy. In this event, initiation of antivenom treatment is recommended with a test dose of one vial (to ensure no or minimal allergic reaction) followed by a final five vial treatment dose. The final category includes severe envenomation. These patients tend to be hemodynamically unstable with evidence of end organ damage, evidence of severe pain or swelling, or severe neurologic/hematologic involvement resulting in respiratory dysfunction. This category also includes patients with evidence of compartment syndrome. Patients with severe envenomation will also receive the test dose followed by treatment with nine vials in the absence of further reaction.
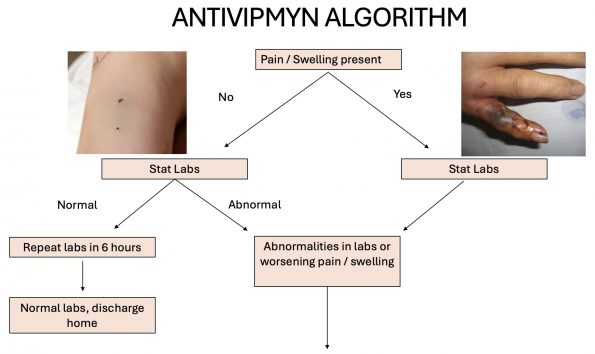
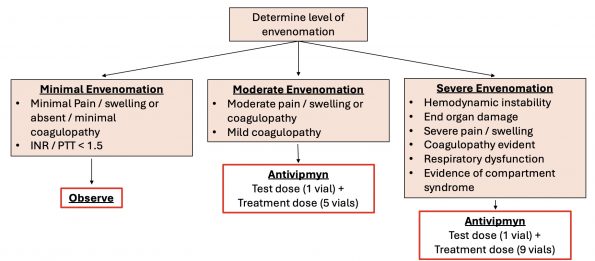
Figure 5: Antivipmyn treatment protocol for venomous snake bites.
All of these patients will be observed for at least 24 hours in the hospital depending on the severity of their envenomation. Repeat labs are done every six hours or two hours post anti-venom treatment. Further, repeat dosing of antivenom is done depending on reassessment clinically every 2 to 4 hours. Should a patient in any of these envenomation categories show improvement in their symptoms, maintenance dosing can be initiated (outlined below). This maintenance dose is divided into three doses delivered over 18 hours. Should a patient develop worsening symptoms or transition up within a severity category, a repeat dose of what you have already given that patient can be given.
Maintenance Dose: 2/3 of treatment dose divided into three doses
There will be many times when diagnostic clarity may be lacking and where treatment would be dependent on patient history. In consultation with Dr. E. Austin from Ontario Poison Center, if the diagnosis is unclear, it is reasonable to wait and observe for 4-6 hours while bloodwork is being done. This would provide certainty to the clinician and is reassuring when there are no clinical symptoms after this time period.
Special Populations

Now let’s consider some special populations. Interestingly, in our pediatric population, the dosing of antivenom remains the exact same as the adult dose. The reason for this is that the envenomation level is the exact same regardless if you’re an adult versus a pediatric patient [1, 4]. This means that the same amount of venom delivered to an adult would similarly be delivered to a child who has a smaller total body weight. Ultimately, we are treating the venom level and not the patient’s weight! The second population includes pregnant patients. Briefly, anti-venom can be safely used in patients who are pregnant regardless of their trimester [1,4]. Finally, when considering someone who comes in with a long list of allergies there are a couple ways you can go about treatment which we will discuss in the following section.
Adverse Events
Allergic reactions can commonly occur with the use of antivenom since their fab fragments have been developed in ovine or equine species. Treatment of an allergic reaction will generally depend on the severity of symptoms. If an individual is experiencing mild symptoms, you can consider observation after a patient-centered discussion. If someone has severe envenomation, then you can continue with treatment as per the protocol and consider decreasing your infusion rate by ½ while having epinephrine at the bedside in the event of an anaphylactic reaction [3]. Should anaphylaxis occur you would proceed down your typical anaphylaxis regimen and stop further infusion of the antivenom.
Another adverse event with antivenom includes serum sickness [4]. Less than 5% of patients who receive anti-venom will develop serum sickness anywhere from 5 to 24 days post-administration. Typical symptoms of these patients include fever, hives, swollen lymph nodes, edema, myalgias, and nausea/vomiting. In some cases, neurologic symptoms can develop in addition to muscle weakness and permanent muscle wasting. Once a patient receives antivenom, it is important to advise them of the potential of serum sickness down the line so they can notify their healthcare team if they return for care with the above symptoms.
Additional Supportive Care
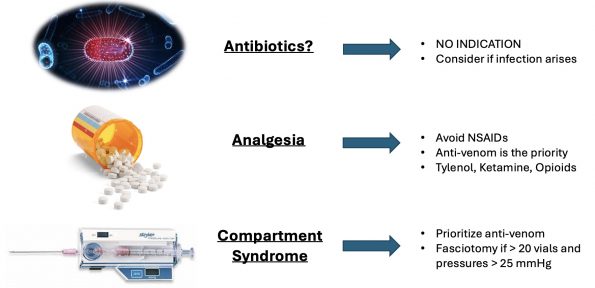
Other considerations during the management of an individual following a venomous snake bite includes elements of supportive care. There is no recommendation for routine antibiotics out of concern for possible infection in these patients [4]. Should a patient later on develop signs or infection around this site, you can consider initiation of antibiotics for cellulitis based on your regional antibiogram.
Analgesia would be another important consideration in these patients. Notably, the use of antivenom is considered a form of analgesia that has a rapid onset and decreases swelling of an extremity as it actively treats the venom. Since venom impacts the coagulation system, it is not advised to use any NSAIDs or aspirin for the treatment of pain in these patients. You may consider using alternatives including Tylenol, ketamine, or opioids.
Further considerations are to monitor for elements of compartment syndrome but intervention including fasciotomy is not immediately indicated unless high doses of anti-venom have already been used given that the swelling can reduce with the use of anti-venom [4]. It is recommended to only consider fasciotomy if you’ve already superseded the use of 20 vials and your compartment pressures are greater than 25 mmHg [4].
“If I had a pulseless limb in front of me, and both antivenom and a surgeon available, I would proceed with both.”
-Dr. Margaret Thompson, MD FRCPC, Ontario Poison Center
For more details on Antivipmyn use, please follow this link for the West Parry Sound guidelines from which this talk was derived [4].
Part 3 – The Myths
In this final section, we’re going to review the typical myths associated with prehospital management and what you should do in the event of seeing someone with a venomous snake bite. Truthfully, the research surrounding prehospital management of venomous snake bites is not very robust, however, we will draw out some clinical pearls that can be carried forward into your next fanged encounter.
There are a lot of misconceptions and false information on the internet. In this section, we will review pre-hospital management and what to do if you encounter a snake bite in a remote area. Interestingly, there was a study performed by Barker and colleagues that analyzed two major search engines and identified 48 web sources for prehospital treatment of snake bites [6]. Unfortunately, 54% contained inappropriate recommendations surrounding management with suction, ice, incision, and electric shock. Now, we won’t dive into each of these techniques but we will focus on the most popular methods of envenomation management.
|
Tourniquets
|
Venom Extractors
|
Pressure Immobilization Bandages
|



Tourniquets
The first commonly described first aid intervention includes the application of a tourniquet to the affected limb immediately following a snakebite. This technique focuses on minimizing the transition of the venom to the system thereby delaying toxic effects. This method, as described in trauma literature, is commonly associated with increased local necrosis and pain for the patient followed by subsequent hyperkalemia with prolonged tourniquet application time [7].
A study by Michael and Khalid in 2010 evaluated the use of any prehospital intervention, including tourniquets, in 72 victims of a venomous snake bite in Nigeria [8]. These interventions were compared to no prehospital intervention and evaluated the level of antivenom required for treatment and length of hospital stay. In this study, most subjects (58, 81%) attempted at least one first aid measure after the bite, including a tourniquet application (53, 74%). Interestingly, the use of any first aid was associated with a longer hospital stay than no use (4.6 ± 2.0 days versus 3.6 ± 2.7 days, respectively, P = 0.02). Furthermore, the antivenom requirement was greater in subjects who had used a tourniquet (P = 0.03) and in those who presented late (P = 0.02) [8]. This may be secondary to the delay to hospital presentation in addition to a sudden surge of venom following the release of the tourniquet resulting in hemodynamic instability.
In summary, tourniquet use was previously described to be useful in remote areas to stabilize an individual before definitive care. However, reported complications include hyperkalemia, ischemia, nerve damage as well as death secondary to these metabolic disturbances [7]. Therefore, there is no recommendation for tourniquet use and prehospital management of venomous snake bites.
Venom Extractors
The next common prehospital intervention includes venom extractors. This includes any device, including someone’s mouth, whereby the venom is extracted via negative pressure applied to the local wound site [7].
A human study by Alberts and colleagues used mock venom with radiotracers to simulate envenomation by the western diamondback snake in a human model [9]. The intervention used the classic Sawyer extractor pump followed by an evaluation of the envenomation level in the blood at 15 minutes. This study demonstrated only an average decrease of 2.0% in total body venom load and an average 0.04% decrease of mock venom at the site of envenomation after 15 min of extraction. It is hypothesized by Albert and colleagues that the extractors could have collapsed the subcutaneous tissue, and pulled fluid from superficial capillaries that contain minimal venom load thereby rendering this technique futile [9].
Ultimately, classic venom extractor devices have been used to control local envenomation sources immediately upon snakebites. However, this is associated with local tissue destruction, user error with improper placement over the envenomation site, and a false sense of security that you extracted a significant amount of venom [7]. Above all else, using this type of extractor in a prehospital setting has been demonstrated to delay the time to definitive care which someone may need [10]. Therefore, there is no recommendation for venom extractors in the prehospital management setting.
Pressure Immobilization Bandages
Our final prehospital intervention includes the pressure of mobilization bandages which is a technique where tensor bandages are applied over the length of the limb to accomplish two goals [7, 11]:
- Block the lymphatic flow of the venom thereby reducing time to toxic effect
- Splint application which prevents muscle contraction thereby decreasing potential lymphatic flow.
However, as with any immobilization or any tensor applied to a limb, this must be removed in a very controlled setting such as the ED. There has been a demonstrated risk of hyperkalemia following envenomation due to local necrosis of tissues.
One pilot study in particular conceptualizes the utility of pressure dressings in the prehospital setting. This study was performed in 2010 by Meggs and colleagues and looked at six anesthetized pigs randomized to pressure dressings vs no intervention with the primary outcome of survival at 24 hours after subcutaneous injection of western diamondback rattlesnake venom [12]. Notably, all subjects receiving pressure dressings survived to 24 hours while none survived in the control group. Post removal of the dressing, one subject died from hyperkalemia which highlights the complication of local necrosis with this intervention.
While there is no study looking solely at immobilization of the limb without compression, it is hypothesized that this may have similar benefits by decreasing muscular contractions.
Consensus
As demonstrated throughout this section, the evidence behind pre-hospital interventions is weak although outlines some important key theories around general management. So what do our leading experts think? Notably, there was general consensus achieved among all toxicologists when we discussed pre-hospital care for these patients. The bottom line is that no intervention should delay the time to definitive care! There are highly effective antidotes for these patients which ultimately impact morbidity and mortality.
In summary, general recommendations are as follows:
- Do not delay time to definitive care when suspecting a venomous snake bite!
- Immobilize the limb if possible.
Take Home Points
- Venomous snake bites are rare due to geographic isolation in Canada but can be fatal.
- Venomous snakes have common physical features which can be utilized for risk stratification.
- The clinical presentation of snake bites is variable due to the anatomy and pathophysiology of venom.
- Patients should be assessed for neurotoxic and hematotoxicity effects (which depends on the snake envenomation suspected).
- Anti-venom is the mainstay of treatment for venomous snake bites.
- There are no contraindications for anti-venom in pregnancy and consideration of dilution for known allergy to anti-venom.
- Pre-hospital management should NOT delay transport to definitive care.
- Recommendations for limb immobilization of snake bites in the pre-hospital setting.
- Recommendations for limb immobilization of snake bites in the pre-hospital setting.
References
- Walls RM, Hockberger RS, Gausche-Hill M, Erickson TB, Milcox SR, Rosen P. Venomous animal injuries. In: Rosen’s emergency medicine: Concepts and clinical practice. Philadelphia, PA: Elsevier; 2023.
- Curran-Sills G, Kroeker J. Venomous snakebites in Canada: A national review of patient epidemiology and antivenom usage. Wilderness & Environmental Medicine. 2018;29(4):437–45. doi:10.1016/j.wem.2018.06.005
- Ahmed S, Ahmed M, Nadeem A, Mahajan J, Choudhary A, Pal J. Emergency treatment of a snake bite: Pearls from literature. Journal of Emergencies, Trauma, and Shock. 2008;1(2):97. doi:10.4103/0974-2700.43190
- Mills, KC. Antivipmyn Treatment Package for Eastern Massasauga Rattlesnake Bites. The Ontario Massasauga Rattlesnake Antivenom Depot. 2022.
- Battle of the Antivenoms: CroFab vs ANAVIP. Blue Ridge Poison Center, University of Virginia Health. 2020.
- Barker S., Charlton N.P., Holstege C.P. Accuracy of internet recommendations for prehospital care of venomous snake bites. Wilderness Environ. Med. 2010;21:298–302. doi: 10.1016/j.wem.2010.08.016.
- Parker-Cote J, Meggs W. First aid and pre-hospital management of venomous snakebites. Tropical Medicine and Infectious Disease. 2018;3(2):45. doi:10.3390/tropicalmed3020045
- Michael G.C., Thacher T.D., Shehu M.I. The effect of pre-hospital care for venomous snake bite on outcome in Nigeria. R. Soc. Trop. Med. Hyg. 2011;105:95–101. doi: 10.1016/j.trstmh.2010.09.005.
- Alberts MB, Shalit M, LoGalbo F. Suction for venomous snakebite: A study of “mock venom” extraction of pit viper envenomations in the United States and Canada. Annals of Emergency Medicine. 2004;43(2):181–6. doi:10.1016/s0196-0644(03)00813-8
- Bush S.P., Hegewald K.G., Green S.M., Cardwell M.D., Hayes W.K. Effects of a negative pressure venom extraction device (Extractor) on local tissue injury after artificial rattlesnake envenomation in a porcine model. Wilderness Environ. Med. 2000;11:180–188.
- Kanaan N.C., Ray J., Stewart M., Russell K.W., Fuller M., Bush S.P., Caravati E.M., Cardwell J., Norris R.L., Weinstein S.A. Wilderness Medical Society practice guidelines for the treatment of pit viper envenomations in the United States and Canada. Wilderness Environ. Med. 2015;26:427–487.
- Meggs W.J., Courtney C., O’Rourke D.P., Brewer K.L. Pilot studies of pressure-immobilization bandages for rattlesnake envenomations. Toxicol. 2010;48:61–63. doi: 10.3109/15563650903376071.