
In Fall 2023, I was working an evening shift at a community hospital when we got a patch. A 3-year-old girl was being brought in by EMS with an out-of-hospital cardiac arrest. CPR was ongoing, and their ETA was 10 minutes.
Watch the entire Grand Rounds here
We prepared the ED for the patient’s arrival. According to EMS, the patient had been sick with upper respiratory symptoms for 2-3 days, including cough, fever, and rhinorrhea. She hadn’t eaten much and had been vomiting that day. Then, she had collapsed in front of her mother 30 minutes prior. We checked a blood glucose and found it to be 2.5. We put in bilateral intraosseous lines and began administering glucose in addition to saline boluses. Bedside ultrasound showed she had a large right pleural effusion, and we placed a chest tube during CPR which produced purulent appearing fluid. We administered antibiotics through the IOs. We ran the resuscitation for 45 minutes, but unfortunately, we were never able to achieve ROSC.
The next day, when I arrived for another shift, I was informed by my staff that the patient’s blood and fluid cultures were positive for Group A Strep. The patient had died of septic shock from an invasive Group A Strep (iGAS) infection. The case was discussed with ID, and I would need to take a 10 day course of Keflex for prophylaxis.
Unfortunately, the tragic story of this young girl was not so unusual in the last year.
In recent months, headline after headline has alerted us to the alarming spike of in cases of invasive group A strep over the last year. In Ontario, 11 children died from invasive group A strep infections between October 2023 and March 2024. In BC, 4 children died in December 2023 due to iGAS infections.
So what’s going on? Why do iGAS infections seem to be surging? And more importantly, what do we as Emergency Physicians need to know about identifying and managing these deadly infections? In part 1 we focus on recognition, investigations, and in part 2 (coming next week!) we will focus on treatment, treatment of pharyngitis in this era, and post-exposure prophylaxis.
Take home #1: Invasive Group A Strep refers to GAS infection infection in the setting of culture isolation of GAS from a normally sterile site
As we know, Streptococcus Pyogenes is a species of gram-positive aerobic bacteria.
These bacteria are the main species that have the Group A antigen, and so are also referred to as Group A Streptococcus (GAS). Group A Strep can cause a wide range of infections, but most commonly pharyngitis or skin and soft tissue infections.
So what makes group A strep invasive?
Invasive Group A Strep (iGAS) infection refers to infection in the setting of culture isolation of GAS from a normally sterile site (most commonly blood; less commonly pleural, pericardial, joint, or cerebrospinal fluid)1.
Keep in mind that this definition means we cannot make a diagnosis of invasive group A strep acutely in the ED. We can only suspect it and manage accordingly.
Generally, iGAS infections take one of the following forms:
- Necrotizing skin and soft tissue infection
- Pregnancy-associated infection
- Bacteremia
- Respiratory tract infection
iGAS infections can be further categorized into those complicated by toxic shock syndrome, and those that are not. Streptococcal toxic shock syndrome has a very specific case definition according to the Center for Disease Control (CDC)2:

Literature suggests that somewhere around one-third of patients with iGAS will progress to meeting the criteria for toxic shock syndrome. This number is as high as 50% in necrotizing fasciitis3,4.
Take home #2: iGAS infections are deadly, and are increasing throughout North America. Yet they are still relatively rare.
So with definitions out of the way, let’s talk about the Epidemiology of iGAS infections, and what’s going on with these infections in North America recently.
Invasive group A strep infections are deadly. In fact, it is one of the leading causes of death attributable to a single pathogen. Estimates vary based on studies, but fatality rates are estimated to range from 11% to as high as 60%. Group A strep is the 9th leading cause of human mortality worldwide that is attributable to a single pathogen 1,5.
These infections are also elusive. In up to 45% of cases, no portal of entry for bacteria is identified 1,4. The most common presentation is skin and soft tissue infections (i.e necrotizing fasciitis). But as you can see below the second most common presentation is occult bacteremia 6. That makes these infections very difficult to catch.
We think that in many cases of isolated bacteremia, skin is actually the portal of entry, but it’s hard to capture this in the data.

These infections are not isolated to children, despite these cases being most prominent in the news. There seems to be a bimodal distribution of iGAS infections. Infections peak before the age of 2, and then prevalence begins to increase after age 50.

Neilson et al, 2016
These infections tend to occur throughout the winter and early spring in North America, with a temporal variation similar to the viral season we are familiar with.

Neilson et al, 2016
And finally, these infections are in fact increasing in frequency. Group A strep cases doubled, increasing from 4.0 to 8.1 cases per 100,000 between 2009 and 2019. Cases declined slightly during the pandemic, but then reached a new peak in 2023. In Ontario, we’ve seen a 62% increase in cases over the last year, with a 13% fatality rate (Unpublished surveillance data, Public Health Agency of Canada).

Unpublished surveillance data NML, PHAC Feb 29 2024
While cases are on the rise, it’s worth putting things in perspective and pointing out that these infections are still extremely rare. Cellulitis is the 9th most common reason people seek medical attention in emergency departments. 4 out of 10 adults in the US seek medical care for a SSTI each year. The incidence of lower extremity cellulitis alone is estimated to be about 200 cases per 100,0007. And so while these infections are deadly and scary, they still make up a tiny proportion of the patients we are going to see in the ED.
So what explains the sharp increase in iGAS infections in recent years? Group A strep has several cell surface molecules and secreted products, which are known as virulence factors. The most important of these is known as the M protein8. The M protein is encoded by the emm gene, and protects the organism against phagocytosis by PMNs. Because mutations of the emm gene are constantly emerging, we use these M types to categorize GAS infections. For example, from the 1980s through the 2000s, the most common strain of invasive Group A Strep was known as the M1 Global strain.
In England, during the 2015–16 season, there was a significant spike in both invasive Group A Strep infections and cases of scarlet fever. These seemed to be associated with the emergence of a new strain of GAS known as the Emm 1 UK strain9. Researchers have observed that the prevalence of this M1 strain has been increasing in prevalence around the world, and have theorized that this new emm1 UK strain may be responsible for the surge of cases around the world and in North America.

However, so far studies haven’t demonstrated a clear link. For example, one study characterized the more recent London UK outbreak in December 2022, and found that only 12% of cases were the emm1 UK clone10. Then again, another study looked at 86 cases of Group A Strep in an ICU in Belgium from 2022-23. It found that 73% of cases were an emm1 strain – and of these, almost all were the new UK lineage.11
So this strain probably is contributing to the growing cases, but it’s likely only part of the picture. For example, some have suggested that humans lost some of their immunity to strep during the pandemic. Others have theorized that because we are more susceptible to viruses post-pandemic, when we do get viral illnesses we are more susceptible to invasive infections. Finally, it’s possible that climate change and globalization are also playing a role.
Take home #3: Necrotizing fasciitis is a clinical diagnosis. Imaging should not delay surgical consultation and treatment, and we should not rely on labs to rule in or out the diagnosis.
So with all that said, when should we suspect these infections in the emergency department?
As a reminder, roughly 40% of cases present as skin and soft tissue infections.6 With that said the first thing we must be able to do to catch iGAS infections is recognize necrotizing fasciitis.
Dr. Krishan Yadav et al. recently developed an ED Best Practices Checklist for Skin and Soft Tissue infections. These guidelines have been endorsed by CAEP, and will be published in CJEM in the coming months. The guideline recommendations were developed by reviewing existing guidelines, systematic reviews, and relevant literature.
The recommendations were also modified by the steering committee specifically for the Canadian emergency department context.
One important message about necrotizing fasciitis in this guideline is that it is a clinical diagnosis requiring clinical judgment. Features suggesting the involvement of deeper structures may include:
- Pain out of proportion
- Hard, wooden feel of subcutaneous tissue
- Systemic toxicity, often with altered mental status
- Edema or tenderness beyond cutaneous erythema
- Crepitus
- Bullous lesions
- Skin necrosis
Some exam findings have been shown to have good specificity for identifying necrotizing fasciitis, including fever, hemorrhagic bullae, and hypotension12. If you see these in a patient with a soft tissue infection, you need to think about necrotizing fasciitis. However, the sensitivity of all of these is poor and so we cannot use any of these to individually rule out NSTI.

Fernando et al., 2019
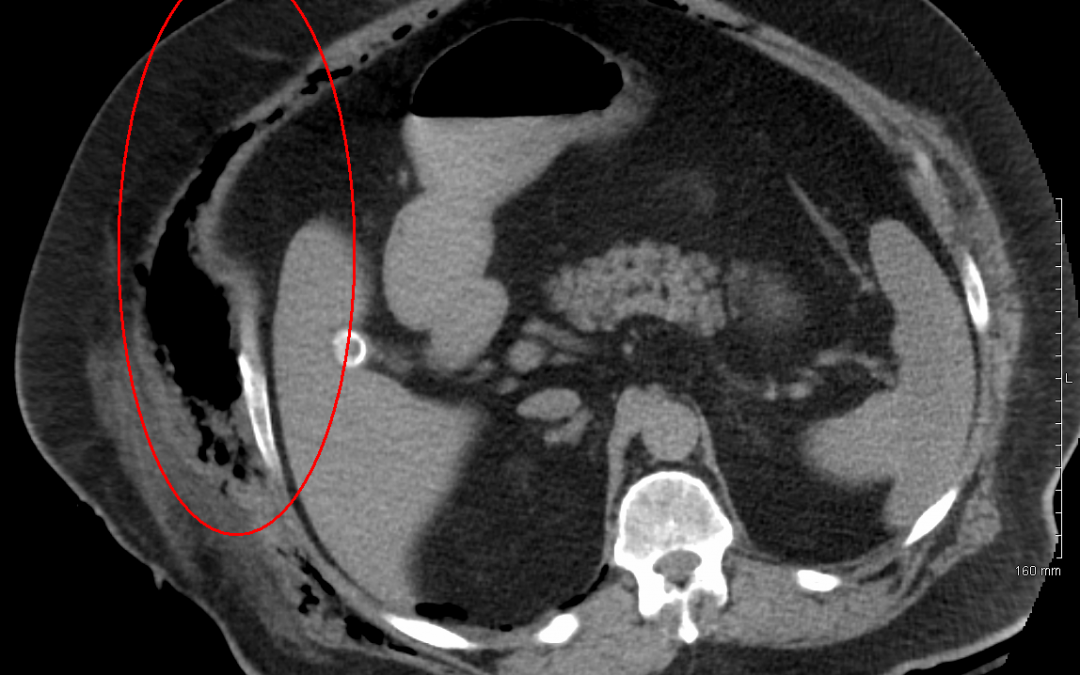
The guideline also addresses the question of whether there is a role for imaging in diagnosing necrotizing fasciitis. In 2019, Fernando and colleagues performed a systematic review looking at the diagnostic accuracy of imaging for necrotizing fasciitis12. As you can see, the sensitivity of X ray for diagnosing necrotizing fasciitis is extremely poor, and should not be relied on. CT has better sensitivity though still not good enough, at 88.5%. The specificity of these tests though is quite good – meaning if you do see gas on imaging, necrotizing fasciitis is highly probable. However, a major concern with CT is that it may delay surgical consultation, which is required for definitive diagnosis and management.

Fernando et al., 2019
For that reason, the working group recommended that clinicians not rely on imaging tests to help diagnose necrotizing fasciitis. That does not mean the CT is not helpful in necrotizing fasciitis. For example, CT may be very important from a surgical planning standpoint. Imagine a patient has necrotizing fasciitis on their upper arm. It may be very important to determine if the infection extends into the chest, in which case thoracics will need to be involved. The message here is that we should not be relying on CT as emergency physicians for making this diagnosis.
What about laboratory investigations? Can we use bloodwork to help rule in or rule out a Nec Fasc diagnosis? Many of us will be familiar with the LRINEC score. This is a score that uses a combination of lab values to assign patients a risk level of necrotizing fasciitis. Scores of greater than 8 are considered high risk.

The same systematic review also looked at the accuracy of the LRINEC score for diagnosing necrotizing fasciitis, and found that it performs quite poorly. For extremely high scores of > 8, there is a reasonable specificity of 95%. But still extremely poor sensitivity. So if you suspect necrotizing fasciitis, you should not be reassured by normal lab values.

Fernando et al., 2019
Take home #4: Clinical clues suggesting iGAS infection include:
- Rapidly progressive syndromes
- Hypotension despite aggressive therapy
- The critically ill patient with no clear source
- Peripartum or post-op patients
- Varicella infection
- Rapidly progressing pneumonia
We know how to diagnose necrotizing fasciitis. But again, somewhere around 25%-40% of cases won’t present with any skin and soft tissue infection. So in which patients without SSTIs should we be suspecting iGAS? Unfortunately, there is a paucity of evidence regarding the syndrome of group a strep without necrotizing SSTI.
I spoke to Dr. Fahad Chowdury, an Infectious Disease physician at the Ottawa Hospital.
He explained the pathophysiology is the same as in toxic shock syndrome secondary to necrotizing fasciitis – shock and multiorgan failure secondary to streptococcal toxins. With that said, the same things we look for in necrotizing fasciitis, even in the absence of skin and soft tissue infection, should prompt us to think about iGAS, as highlighted above.
Dr. Chowdhury also pointed out that in most cases of iGAS without any source, skin is actually the portal of entry, it just isn’t obvious. And so in these patients, it’s really important to do a thorough head to toe exam, looking for any signs of minor trauma or skin lesions. Finally, Dr. Chowdhury also pointed out that the insecurely housed are disproportionately at risk of group a strep infections. Patients who are homeless or who inject drugs that present critically ill should also prompt you to think about this diagnosis.
Finally, you should think about iGAS in a patient with pneumonia or empyema who doesn’t seem to be responding to usual management or who has progressed rapidly. The same Belgian case series we looked at earlier found that in those admitted to ICU with GAS infections, 45% of adults and 77% of children had pneumonia, with a significant proportion in each group progressing to empyema11.
I also spoke with Dr. Krishan Yadav, an ED physician at University of Ottawa, and lead author on the CAEP endorsed skin and soft tissue infection best practice checklist. He said the following:
“We see a ton of sepsis. But invasive group A strep – these patients deteriorate in front of you. Look for clear signs of evolution and consider it in fever without a source. Perform a good head to toe exam. Also consider the diagnosis in the patient not responding to usual sepsis care.”
Stay tuned for part 2 next week where we focus on treatment, the management of pharyngitis given the increasing invasive group A strep prevalence, and prophylaxis for exposures!
References
- Waddington CS, Snelling TL, Carapetis JR. Management of invasive group A streptococcal infections. J Infect. 2014;69 Suppl 1:S63-69. doi:10.1016/j.jinf.2014.08.005
- Streptococcal Toxic Shock Syndrome (STSS) (Streptococcus pyogenes) 2010 Case Definition | CDC. Published June 11, 2021. Accessed June 29, 2024. https://ndc.services.cdc.gov/case-definitions/streptococcal-toxic-shock-syndrome-2010/
- Kaul R, McGeer A, Low DE, Green K, Schwartz B. Population-based surveillance for group A streptococcal necrotizing fasciitis: Clinical features, prognostic indicators, and microbiologic analysis of seventy-seven cases. Ontario Group A Streptococcal Study. Am J Med. 1997;103(1):18-24. doi:10.1016/s0002-9343(97)00160-5
- Stevens DL, Tanner MH, Winship J, et al. Severe group A streptococcal infections associated with a toxic shock-like syndrome and scarlet fever toxin A. N Engl J Med. 1989;321(1):1-7. doi:10.1056/NEJM198907063210101
- Carapetis JR, Jacoby P, Carville K, Ang SJJ, Curtis N, Andrews R. Effectiveness of clindamycin and intravenous immunoglobulin, and risk of disease in contacts, in invasive group a streptococcal infections. Clin Infect Dis Off Publ Infect Dis Soc Am. 2014;59(3):358-365. doi:10.1093/cid/ciu304
- Nelson GE, Pondo T, Toews KA, et al. Epidemiology of Invasive Group A Streptococcal Infections in the United States, 2005-2012. Clin Infect Dis Off Publ Infect Dis Soc Am. 2016;63(4):478-486. doi:10.1093/cid/ciw248
- Miller LG, Eisenberg DF, Liu H, et al. Incidence of skin and soft tissue infections in ambulatory and inpatient settings, 2005-2010. BMC Infect Dis. 2015;15:362. doi:10.1186/s12879-015-1071-0
- Walker MJ, Barnett TC, McArthur JD, et al. Disease Manifestations and Pathogenic Mechanisms of Group A Streptococcus. Clin Microbiol Rev. 2014;27(2):264-301. doi:10.1128/CMR.00101-13
- Lynskey NN, Jauneikaite E, Li HK, et al. Emergence of dominant toxigenic M1T1 Streptococcus pyogenes clone during increased scarlet fever activity in England: a population-based molecular epidemiological study. Lancet Infect Dis. 2019;19(11):1209-1218. doi:10.1016/S1473-3099(19)30446-3
- Alcolea-Medina A, Snell LB, Alder C, et al. The ongoing Streptococcus pyogenes (Group A Streptococcus) outbreak in London, United Kingdom, in December 2022: a molecular epidemiology study. Clin Microbiol Infect Off Publ Eur Soc Clin Microbiol Infect Dis. 2023;29(7):887-890. doi:10.1016/j.cmi.2023.03.001
- Peetermans M, Matheeussen V, Moerman C, et al. Clinical and molecular epidemiological features of critically ill patients with invasive group A Streptococcus infections: a Belgian multicenter case-series. Ann Intensive Care. 2024;14(1):19. doi:10.1186/s13613-024-01249-7
- Fernando SM, Tran A, Cheng W, et al. Necrotizing Soft Tissue Infection: Diagnostic Accuracy of Physical Examination, Imaging, and LRINEC Score: A Systematic Review and Meta-Analysis. Ann Surg. 2019;269(1):58. doi:10.1097/SLA.0000000000002774
- Babiker A, Li X, Lai YL, et al. Effectiveness of adjunctive clindamycin in β-lactam antibiotic-treated patients with invasive β-haemolytic streptococcal infections in US hospitals: a retrospective multicentre cohort study. Lancet Infect Dis. 2021;21(5):697-710. doi:10.1016/S1473-3099(20)30523-5
- DeMuri GP, Sterkel AK, Kubica PA, Duster MN, Reed KD, Wald ER. Macrolide and Clindamycin Resistance in Group a Streptococci Isolated From Children With Pharyngitis. Pediatr Infect Dis J. 2017;36(3):342-344. doi:10.1097/INF.0000000000001442
- Lu B, Fang Y, Fan Y, et al. High Prevalence of Macrolide-resistance and Molecular Characterization of Streptococcus pyogenes Isolates Circulating in China from 2009 to 2016. Front Microbiol. 2017;8:1052. doi:10.3389/fmicb.2017.01052
- Parks T, Wilson C, Curtis N, Norrby-Teglund A, Sriskandan S. Polyspecific Intravenous Immunoglobulin in Clindamycin-treated Patients With Streptococcal Toxic Shock Syndrome: A Systematic Review and Meta-analysis. Clin Infect Dis Off Publ Infect Dis Soc Am. 2018;67(9):1434-1436. doi:10.1093/cid/ciy401
- Mariani F, Gentili C, Pulcinelli V, Martino L, Valentini P, Buonsenso D. State of the Art of Invasive Group A Streptococcus Infection in Children: A Scoping Review of the Literature with a Focus on Predictors of Invasive Infection. Child Basel Switz. 2023;10(9):1472. doi:10.3390/children10091472
- Miller KM, Barnett TC, Cadarette D, Bloom DE, Carapetis JR, Cannon JW. Antibiotic consumption for sore throat and the potential effect of a vaccine against group A Streptococcus: a systematic review and modelling study. EBioMedicine. 2023;98:104864. doi:10.1016/j.ebiom.2023.104864
- Fine AM, Nizet V, Mandl KD. Large-scale validation of the Centor and McIsaac scores to predict group A streptococcal pharyngitis. Arch Intern Med. 2012;172(11):847-852. doi:10.1001/archinternmed.2012.950
- Sauve L, Forrester AM, Top KA. Group A streptococcal pharyngitis: A practical guide to diagnosis and treatment. Paediatr Child Health. 2021;26(5):319-320. doi:10.1093/pch/pxab025
- Spinks A, Glasziou PP, Del Mar CB. Antibiotics for treatment of sore throat in children and adults. Cochrane Database Syst Rev. 2021;12(12):CD000023. doi:10.1002/14651858.CD000023.pub5
- Shulman ST, Bisno AL, Clegg HW, et al. Clinical practice guideline for the diagnosis and management of group A streptococcal pharyngitis: 2012 update by the Infectious Diseases Society of America. Clin Infect Dis Off Publ Infect Dis Soc Am. 2012;55(10):e86-102. doi:10.1093/cid/cis629
- Overview | Sore throat (acute): antimicrobial prescribing | Guidance | NICE. Published January 26, 2018. Accessed April 30, 2024. https://www.nice.org.uk/guidance/ng84
- Khan F, Bai Z, Kelly S, et al. Effectiveness and Safety of Antibiotic Prophylaxis for Persons Exposed to Cases of Invasive Group A Streptococcal Disease: A Systematic Review. Open Forum Infect Dis. 2022;9(8):ofac244. doi:10.1093/ofid/ofac244
- The Prevention of Invasive Group A Streptococcal Infections Workshop Participants. Prevention of Invasive Group A Streptococcal Disease among Household Contacts of Case Patients and among Postpartum and Postsurgical Patients: Recommendations from the Centers for Disease Control and Prevention. Clin Infect Dis. 2002;35(8):950-959. doi:10.1086/342692
