
Necrotising soft tissue infections are an significant cause of morbidity and mortality, so an timely diagnosis is critical for the Emergency Physician. Here we discuss the publication of a new systematic review and meta-analysis on this challenging diagnostic entity, and include an helpful infographic to help interpret the findings [1].
Background
Necrotizing soft tissue infection (NSTI, commonly referred to as ‘necrotizing fasciitis’) is a life-threatening skin and soft tissue diagnosis that is characterized by widespread tissue necrosis [2]. NSTI is a rare diagnosis, and as such, is often missed, especially in its early stages. The treatment of NSTI is primarily surgical, as these patients require debridement of necrotic tissue. Gold standard diagnosis is therefore made intraoperatively, or on tissue biopsy. Delay to surgical intervention in these cases is associated with increased morbidity and mortality [3]. In the Emergency Department (ED), we often see patients with more benign skin and soft tissue infections, and the large majority of these patients are sent home with oral antibiotics. Differentiating NSTI from other skin and soft tissue infections can be extremely difficult, but is important to ensure better outcomes in these patients.
Physical Exam
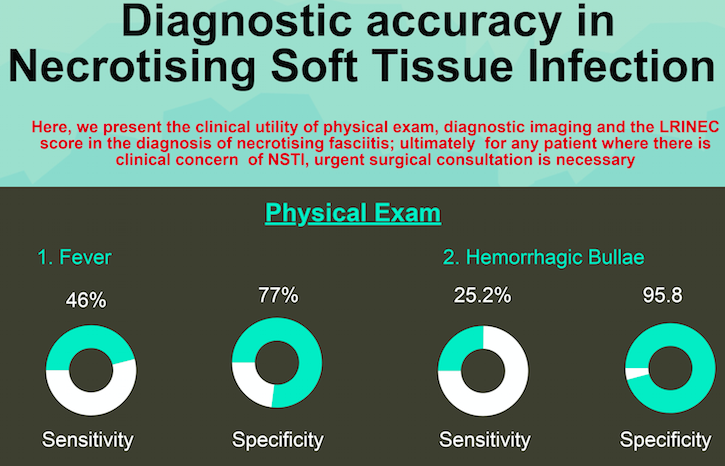
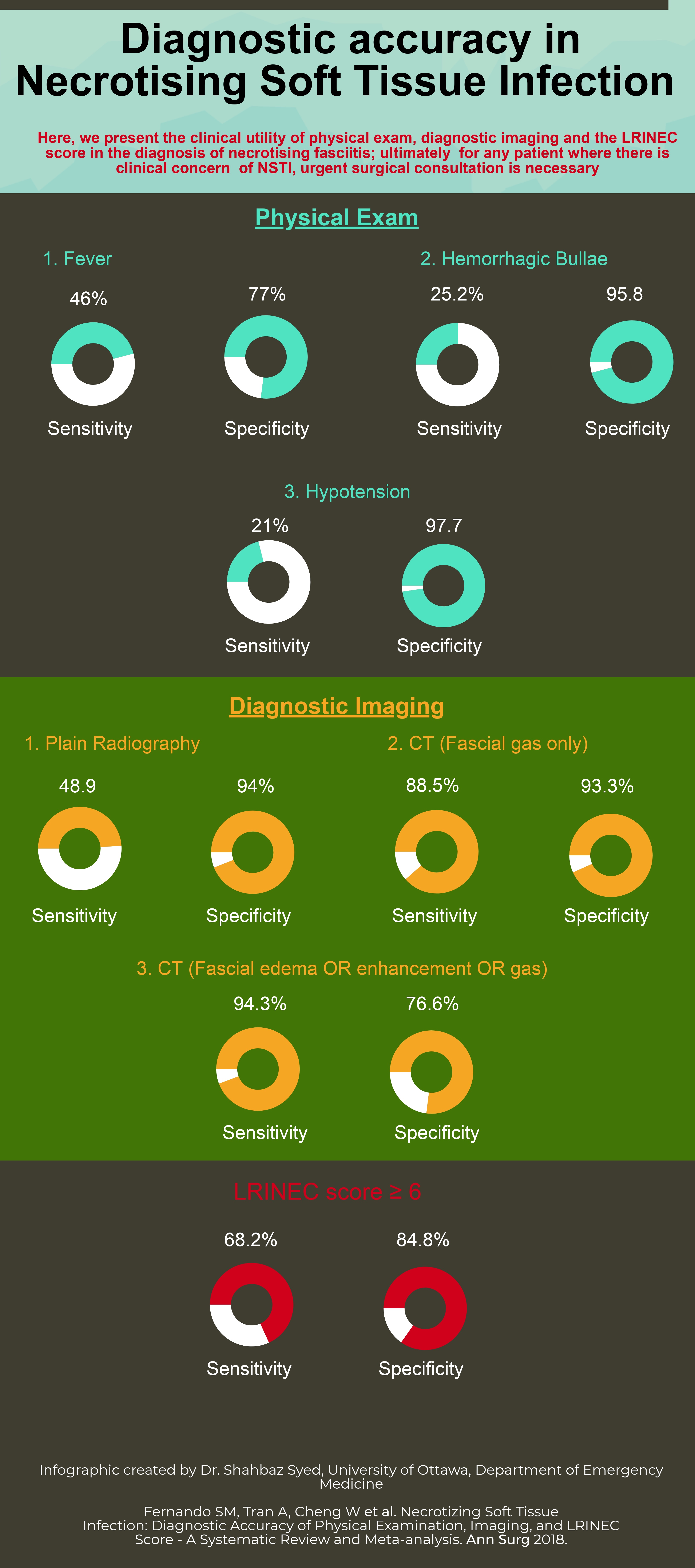
Certain physical examination findings are commonly associated with diagnosis of NSTI. These include fever, hypotension, severe pain (often referred to as “pain out of proportion”), crepitus, and hemorrhagic bullae. Unfortunately, very few of these physical examination findings were evaluated in the available literature. Our search allowed for the meta-analyses of three physical findings. Fever (defined as body temperature ≥ 38 degrees Celsius) had a sensitivity of 46.0% and a specificity of 77.0% for diagnosis of NSTI. Presence of hemorrhagic bullae had a sensitivity of 25.2%, and a specificity of 95.8%. Finally, hypotension (defined as a systolic blood pressure < 90 mmHg) had a sensitivity of 21.0%, but a specificity of 97.7%. The poor sensitivity of these physical examination findings suggests that none of them should be individually used to rule out the diagnosis of NSTI. A patient with a 50% pre-test probability of NSTI, but the absence of fever, hemorrhagic bullae, or hypotension still retains a post-test probability of 41.3%, 43.9%, and 44.7%, respectively. Of note, in practice, we often use a combination of physical exam features to diagnose NSTI, but such combinations were not evaluated in the available literature.
Imaging
Multiple imaging modalities can be used to evaluate for NSTI. Plain radiography (X-ray) has the advantage of being available in the large majority of centres, and can be performed at the bedside in an unstable patient. The classic finding seen on plain radiography for diagnosis of NSTI is fascial air or gas. We found that plain radiography had a sensitivity of 48.9%, and a specificity of 94.0%. Therefore, the presence of fascial gas on plain radiography is highly suggestive of NSTI, but absence does not rule out the diagnosis. Computed tomography (CT) is available less ubiquitously, and also can be more time-consuming. Furthermore, transfer of unstable patients to CT is problematic. CT is beneficial in equivocal cases, because while it can similarly demonstrate evidence of fascial gas, it can also evaluate for more subtle findings, such as fascial enhancement or edema. Presence of fascial gas on CT had a sensitivity of 88.5%, and a specificity of 93.3%. Broadening CT criteria to additionally evaluate for the presence of either fascial gas, enhancement or edema increased the sensitivity to 94.3%, but decreased the specificity to 76.6%. In a patient with a 50% pre-test probability of NSTI, the presence of fascial gas on CT increases the post-test probability to 93%, while the absence of fascial enhancement, edema, or gas decreases the post-test probability to 7%. Therefore, patients with evidence of fascial enhancement or edema, but without evidence of fascial gas still require surgical consultation for possible NSTI. Future work should evaluate the accuracy of Point-of-Care Ultrasound (PoCUS) for the diagnosis of NSTI.
Laboratory Risk Indicator for Necrotizing Fasciitis (LRINEC) Score
The LRINEC score, initially derived and validated in 2004 [4], is the most widely-used clinical decision instrument for diagnosis of NSTI. It consists of six laboratory values: White blood cell count, hemoglobin, sodium, glucose, creatinine, and C-reactive protein (CRP). A score ≥ 6 is suggestive of a diagnosis of NSTI. However, even in tertiary care centres, it can often take a significant amount of time to obtain laboratory values (particularly CRP), during which time a patient with NSTI can continue to deteriorate. We found that a LRINEC ≥ 6 for diagnosis of NSTI only had a pooled sensitivity of 68.2%, and a specificity of 84.8%. Therefore, a patient with a 50% pre-test probability of NSTI, but a LRINEC score < 6, would still retain a 27.3% risk. Therefore, the available evidence suggests that the LRINEC score should not be used to rule-out NSTI, and surgical consultation should not be delayed in order to obtain laboratory values.
How can I use this evidence to care for my patients?
NSTI is one of the scariest diagnoses for the ED physician. It is rare, and it is often difficult to recognize, particularly in its early stages. What this study demonstrates is that, in isolation, the tools we have commonly used for diagnosis of NSTI are not sufficiently sensitive to rule-out the diagnosis. As such, for any patient where there is clinical concern of NSTI, urgent surgical consultation is necessary. Such consultation should not be delayed in order to obtain imaging or laboratory values, as they cannot rule out the diagnosis. For physicians in centres where immediate surgical consultation is not available in-house, patients should be transferred for surgical evaluation.
The authors would like to thank Drs. Shahbaz Syed and Hans Rosenberg for their hard work in creating the above infographic, and for their consistent efforts in promoting the research of the University of Ottawa Department of Emergency Medicine.
References
- Fernando SM, Tran A, Cheng W et al. Necrotizing Soft Tissue Infection: Diagnostic Accuracy of Physical Examination, Imaging, and LRINEC Score – A Systematic Review and Meta-analysis. Ann Surg 2018.
- Stevens DL, Bryant AE. Necrotizing Soft-Tissue Infections. N Engl J Med 2017;377:2253-2265.
- Elliott DC, Kufera JA, Myers RA. Necrotizing soft tissue infections. Risk factors for mortality and strategies for management. Ann Surg 1996;224:672-683.
- Wong CH, Khin LW, Heng KS et al. The LRINEC (Laboratory Risk Indicator for Necrotizing Fasciitis) score: a tool for distinguishing necrotizing fasciitis from other soft tissue infections. Crit Care Med 2004;32:1535-1541.


