

In part 1 of this 2-part series on medicolegal risk in Emergency Medicine, we looked at two legal cases, with a primary focus on civil litigation and college complaints. In this section, we focus on risk assessment, documentation, and advice from lawyers and CMPA experts, with some frequently asked questions to conclude. Check out part one for the introductory primer and legal cases.
Section 2: The Landscape of Medicolegal Risk in Emergency Medicine
Now that we’ve broken down the process of medico-legal actions, let’s turn our attention to the landscape of risk—where complaints and lawsuits actually originate. What types of cases get physicians into trouble? What patterns are emerging? And most importantly—what can we do about it?
Where Complaints Come From: CMPA Data
A five-year analysis (2018–2022) of 1,892 cases by the CMPA sheds light on the most common patient complaints and peer expert criticisms (CMPA, 2023).

Top patient concerns:
- Deficient assessments – cited in 60% of complaints
- Diagnostic errors – 50%
- Delay or failure to perform a test – e.g., not ordering a CT or LP
But here’s where it gets interesting.
There’s a gap between what patients complain about and what experts actually flag:
- Deficient assessments:
- Cited by patients: 63%
- Cited by experts: 27%
- Unprofessional behavior:
- Patients: >20%
- Experts: 8%
- Documentation errors:
- Rarely cited by patients
- Cited by experts in 25% of cases
Patients need to feel like our assessments are thorough—even when they already are, clinically.
- 🗣️ Clear, compassionate communication reduces complaints.
- 📝 Even if patients don’t care about documentation, experts do. It’s what they review—and what you’ll be judged on.
Bottom line:
Focusing on patient perceptions by performing thorough assessments and communicating clearly reduces complaints.
CPSO Data Supports This (CPSO – Annual Report, 2024.)

In 2024, CPSO reported:
- 51% of all complaints related to communication in clinical practice
(e.g., failure to listen, explain, or obtain informed consent)
- 50% involved professionalism in communication
(e.g., perceived dishonesty, rudeness, or lack of compassion)
🧠 Note: Some complaints involved multiple concerns—so totals exceed 100%
What Plaintiff Lawyers Are Saying
Conversations with Toronto-based malpractice lawyers reinforced this trend.
“Many patients don’t initially call me because they think malpractice occurred. They call because they felt mistreated. The lawsuit often comes later—once potential negligence is uncovered.”
Another lawyer echoed this:
“Most people who call me don’t know what happened. They’re looking for an explanation, not a lawsuit.”
And perhaps most revealing:
“If a doctor is getting frequent complaints, they likely have a communication problem.”
Diagnostic Errors: Not Always Where You Expect
Another major contributor to medico-legal risk is diagnostic error. But here’s what surprised me:

(CMPA, 2023)
It wasn’t the critically ill patients in resus—the memorable, high-stakes cases. It was patients in urgent care—the high-volume, lower-acuity cases. Yes, there’s some natural confounding (fractures are more common than strokes), but it raises an important point:
➡️ Over five years, your college complaint is more likely to involve a missed fracture in urgent care than a missed stroke in resus.
🟢 Takeaway: The steps you take to protect yourself legally in resus? You should also be applying them in urgent care.
Reducing Diagnostic Errors: Evidence from Sepsis Cases
A study by Neilson et al. (2011–2020) analyzed medico-legal cases involving sepsis and found key patterns (Neilson et al., 2023):
- Repeat Presentations Are a Red Flag
- 49% of patients had multiple visits (family doctor, walk-in, or ED) before hospitalization
- 75% of these had >1 visit within 72 hours of admission
- 🟢 A patient returning to the ED = pause and reassess.
- Deficient Assessments Were Common (75% of cases)
Examples included:
-
- ❌ Not reassessing before discharge
- ❌ Failing to consider alternative diagnoses
- ❌ Attributing symptoms to medications without further workup
🧠 The key message:
Use your Type II brain.
- If a patient isn’t responding as expected—rethink.
- If a patient looked sick at any point—reassess before discharge.
- Document your reasoning. If you ruled out something serious, make it explicit.
High-Risk Patient Populations

CMPA data confirms that certain patients have inherently higher risk of bad outcomes (CMPA, 2023).
- Patients with complex or preexisting conditions
- Elderly patients
This isn’t surprising—but it matters.
🟢 For patients with high baseline risk, lower your threshold for testing, monitoring, and reassessment.
Night Shifts: A Quiet Risk Factor
Emerging data suggests that complaints and legal cases are more common at night (Cortel-LeBlanc et al., 2023; Haroutunian et al., 2018). Why?
- Fatigue
- Fewer resources
- Decision fatigue later in the shift
- Longer wait times → more dissatisfied patients
But here’s the reality: Courts don’t care what time it is or how long you’ve been on shift. So if it’s 6:00 AM and you’re deciding whether to do that second troponin…
- 💡 Ask yourself: “What would I be doing if this were the first patient of my shift?”
🔑 Key Takeaways from This Section
✅ Complaints are often about perception – not negligence
- Patients want to feel heard
- Clear communication and a “thorough-seeming” assessment reduce complaints
- Plaintiff lawyers confirm: Many lawsuits could be avoided with simple empathy and explanation
✅ Most diagnostic errors happen in urgent care – not resus
- These cases move quickly – slow down and stay sharp
✅ Repeat visits are a red flag
- Pause and reassess the story
✅ Severely ill and elderly patients require extra caution
- Lower thresholds for testing, monitoring, and reassessment
✅ Night shifts carry a higher legal risk
- Fatigue is real – but the legal standard doesn’t change
- Treat every patient like it’s your first of the shift
Documentation
Let’s talk about documentation. From a medico-legal perspective, documentation is critical. Deficient documentation was cited as peer criticism in 25% of all medico-legal cases involving emergency physicians over a 10-year period. (CMPA, 2023)
What Carries Weight in Court?
According to leading malpractice lawyers, there’s a hierarchy of weight when it comes to evidence in court:
- 🔝 The medical record: If it’s written down, it’s difficult to dispute.
- 🧠 The patient’s recollection: Courts assume patients remember their medical encounters better than physicians remember individual patients.
- 👨⚕️ The physician’s recollection: Judges recognize we see thousands of patients. Patients typically see only a few physicians.
There’s nuance here. A physician’s “standard invariable practice” (i.e., what they say they do in all cases) is also afforded some weight. But if there’s a conflict between the patient’s memory and your specific recollection? The court may side with the patient unless you can clearly explain why you remember that case—and that patient.
🟢 Bottom line: Documentation is like insurance. You hope you don’t need it. But when you do, you’ll be very glad it’s there.
Where are we Making Mistakes?
A study analyzed a random sample of 20% of medico-legal cases (2016–2020) where emergency physicians were criticized for documentation issues (Smith et al., 2023)
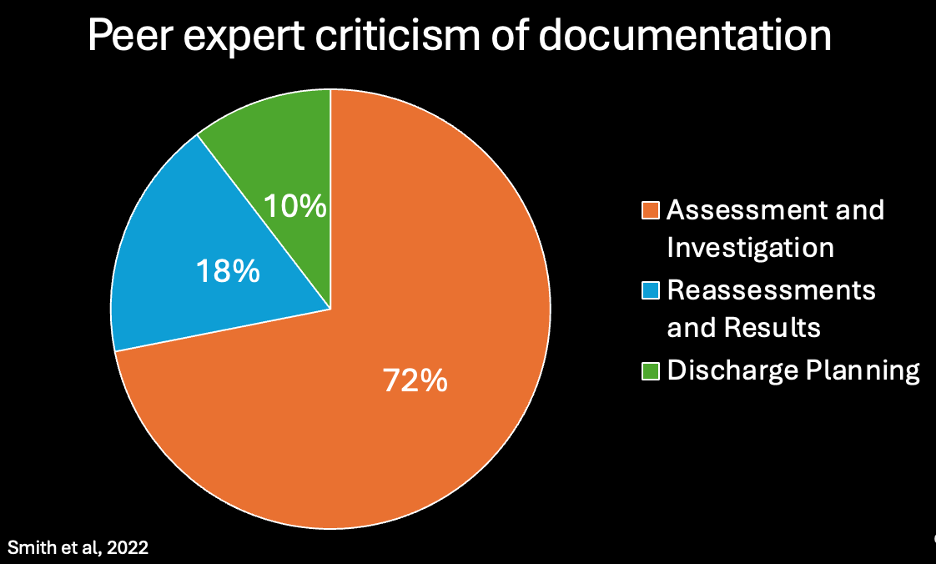
Most common problem areas:
- Assessment and investigation
-
- Missing pertinent negatives in history or exam
- Not addressing abnormal vital signs
- Reassessments and test results
-
- Failing to document reassessments
- Ignoring abnormal labs or imaging
- Discharge planning
-
- Missing documentation of instructions or medication risks
So, how much should you document?
It’s tempting to think the answer is: document everything. But that’s not what the experts recommend. One leading malpractice lawyer put it this way:
“You don’t have to write a novel. We’re talking about going from four hen scratches to a SOAP note. It doesn’t need to take that much time. But another ER physician should be able to read your note, understand your history and physical exam, and know what you were thinking.”
And beyond medico-legal protection, documentation is also about patient care:
“The medical record is the best way to communicate with your team. If you don’t do this properly, it doesn’t look good.”
Documentation Tips from Dr. David Carr
Dr. David Carr is an emergency physician at UHN in Toronto with extensive experience as an expert witness for the CMPA and various plaintiff firms. He has reviewed over 250 medico-legal files.
Here are his Top 5 Documentation Pearls:
- Everything in the medical record is fair game.
-
- Abnormal vitals, lab results, and nursing notes—if you don’t address them, they can work against you.
- If a triage note suggests a serious diagnosis but your assessment differs, document why.
- Pertinent positives and negatives matter.
-
- Writing “neuro normal” isn’t enough.
- If this goes to discovery, it becomes your word vs. the patient’s. Spell it out.
- Late documentation is a red flag.
-
- If something goes wrong and you reopen the chart the next day to add a note, it looks suspicious.
- Epic is completely traceable and timestamped.
-
- If you open an ECG before picking up the chart, that’s recorded—and can be used against you.
- Document your thinking—but don’t repeat yourself.
-
- If you ruled out DVT, you don’t need to list it again in the plan.
- You don’t always need to explain why you’re doing something.
- But you might need to explain why you’re not.
Documentation – Take Home Points
- ✅ The medical record is the most important piece of evidence in court.
- If it’s not documented, it didn’t happen.
- ✅ You don’t need to write a novel.
- Just enough so another ER doc can follow your thinking.
- ✅ Focus on specific, pertinent positives and negatives.
- “Neuro normal” isn’t enough. Be explicit.
- ✅ Consider documenting your reasoning.
- If you ruled out something significant, note it.
- If you chose not to do a test, explain why.
Frequently Asked Questions
To wrap things up, let’s address some of the most common questions physicians have around medico-legal risk in emergency medicine.
Question 1: Do a lack of resources put me at risk?
With overcrowded EDs, hallway medicine, and limited resources, many physicians wonder if they’re at increased legal risk simply for working in a broken system.
Short answer? No.
In the few legal cases where this has come up, courts have considered the available resources when assessing the standard of care (CMPA, 2022). Ultimately, your peers are the ones determining whether care met the standard—and your peers understand the realities of emergency medicine. The standard is not perfection. It’s what a reasonable colleague would have done in similar circumstances—not in an ideal, fully resourced hospital.
➡️ If you document that you’re doing the best you can for the patient given the circumstances, you’re on solid ground. CMPA statements support this (CMPA, 2022).
Question 2: Can residents be named in a medico-legal action?
Yes—but it’s far less common than for staff physicians.
- Over a 10-year period, only 4% of residents were named in a legal action (Crosbie et al., 2022)
- College complaints against residents have remained stable even as overall complaint volumes have increased
- Most civil cases involving learners are in surgical specialties (McDougall et al., 2022)
There’s no evidence that staff working with learners are at increased legal risk.
⚕️ Key points for residents:
- You are judged based on the standard of care for your level of training.
- Most peer criticism centers around: communication and professionalism.
- If an interaction with a patient isn’t going well—escalate to staff.
Question 3: Do medical directives put me at legal risk?
Some physicians worry that medical directives—tests or treatments initiated by nurses under standing orders—might expose them to legal action. But the data says otherwise. Out of 1,957 medico-legal cases involving emergency physicians between 2016 and 2021, only 28 involved medical directives (Cortel-LeBlanc et al., 2023).
➡️ The issue isn’t the directive itself. It’s how the physician handles the result.
Physicians were criticized when they:
- Didn’t acknowledge investigations ordered under a directive
- Didn’t review or act on results
🟢 Takeaway:
- Medical directives don’t increase risk on their own.
- But you are responsible for reviewing and responding to what they uncover.
Question 4: Should I apologize if I make a mistake?
Some physicians worry that apologizing could be interpreted as an admission of guilt. But in Ontario, legislation explicitly states: An apology is not an admission of liability. That said, if you’re concerned you’ve made an error, it’s absolutely appropriate to contact the CMPA before apologizing. Often, what patients are looking for is clarity and closure, and a sincere explanation may prevent a lawsuit before it even starts.
Question 5: Should I be practicing defensive medicine?
The fear of litigation leads some physicians to over-test, consult early, and practice in a way that feels “safe”—but isn’t always in the patient’s best interest. Every expert I spoke with—CMPA physicians, malpractice lawyers, emergency physicians—agreed:
This is not the right approach.
- 🔴 Reason 1: It’s bad medicine. You may cause harm through unnecessary testing.
- 🔴 Reason 2: It doesn’t even lower your legal risk.
Dr. Lisa Thurgur, CMPA Physician Advisor, said:
“We all have medico-legal risk. But you can’t practice looking over your shoulder—that’s just bad medicine. Practice to the best of your ability, doing what’s best for your patient.” “We can be emergency docs because of the CMPA. Every day you practice to the best of your ability. If something goes wrong, you’ll be okay because of the CMPA.”
One malpractice lawyer explained:
“You cannot practice out of fear. This is not a good way to be, and it will lead to burnout. Know that the standard is not perfection—it’s what is reasonable. What would a reasonable emergency physician in your shoes do?.. And if you order 55 tests but don’t take time to communicate with the patient, you still might get a claim because they felt you were not treated properly.”
Another lawyer added:
“I’m not advocating defensive medicine. No one is asking you to do this, and it’s arguably negligent. Even a blood test is not benign. You don’t have to act as a referral service.”
Dr. Shahbaz Syed, Emergency Physician at the University of Ottawa, reflected:
“We do a lot of unnecessary harm by practicing defensively. Some of it we never see because it happens down the road. Ask yourself—do you want to do this job so you can sleep better at night, or so you can help people?”
🟢 Takeaway:
Practicing defensively doesn’t protect you – it causes harm, burnout, and doesn’t lower your legal exposure.
Question 6: How should I approach a medico-legal claim?
Dr. Shahbaz Syed offers four key pieces of advice:
- Don’t reach for the chart.
- You are not the chart custodian, and this can work against you.
- ➡️ First step: Call the CMPA.
- Feel your feelings – but set a timer.
- “The hardest part is getting over the fact that you messed up. We’re used to being good and succeeding. It’s hard to convince yourself you’re not a bad doctor. But you’re not. You’re not a bad person.”
- Don’t let resentment toward patients carry into your work.
-
- It’s easy to feel jaded after a complaint. But don’t let it affect the next patient.
- “The patient in front of you is a person with lived experience. You owe it to them to treat them as a fresh patient.”
- Find the learning point—but don’t overcorrect.
-
- “There’s always something to learn from a case. Take that insight, apply it, but it doesn’t have to change your entire practice.”
🧠 A medico-legal claim is a process – not a reflection of your worth as a physician. Learn from it—but don’t let it define you.
Conclusion: What Made the Difference?
Let’s come back to the two cases we started with (click here for a refresher).
Case 1: Philisha Sutherland
Dr. Booth documented her assessment thoroughly, including multiple reassessments throughout the patient’s stay in the emergency department.
At trial:
- The defense relied entirely on the medical record.
- The plaintiff relied on the family’s account, which was not corroborated in the documentation.
The judge made a critical statement:
“If I had to make a choice, I would prefer an opinion based on the medical documentation and how Philisha Sutherland presented at the Sault Area Hospital over an opinion which relied on information from collateral sources.”
(Sutherland et al. V. Booth, 2024)
Case 2: Kamal Baines
Dr. Abounaja’s case played out differently. There were documentation gaps that became problematic:
- Nurses documented that the physician was aware of the pulseless leg, but this wasn’t recorded in the physician’s chart until several hours later.
- The first discussion with CritiCall didn’t clearly mention the pulseless limb. While the emergency physician requested transfer, it wasn’t made explicit that the concern was for vascular injury to the lower extremity.
At trial, the two key issues were:
- Failure to insist on urgent transfer, and failure to explicitly communicate the pulseless limb.
- Reliance on personal recollection during discovery, rather than a clear, contemporaneous medical record.
Despite early involvement of consultants and efforts to escalate care, deficient documentation and communication breakdowns left him legally exposed.
➡️ The case was decided in favor of the plaintiff.
(Baines v Abounaja, 2023; Cahill, 2023)
So What Made the Difference?
- Clear, thorough documentation
- Consistent communication
- Explicit documentation of key clinical concerns
- A medical record that could stand on its own in court
🔑 Final Takeaways
- Emergency physicians face greater medico-legal risk than any other non-surgical specialty.
-
- ➡️ While this is stressful, proactive awareness is essential.
- If you receive a complaint or lawsuit, contact the CMPA immediately.
-
- ➡️ They will guide you through every step of the process.
- Despite the high volume of actions, outcomes in Canada are generally favourable for physicians.
-
- ➡️ Most cases are dismissed, abandoned, or settled. Very few go to trial—and most that do are decided in favor of the physician.
- You are not held to a standard of perfection.
-
- ➡️ The legal standard is what a reasonable emergency physician would do in your situation.
- The best way to reduce legal risk is through communication.
-
- ➡️ Make patients feel heard, and make their assessment feel thorough.
- Documentation is key. You don’t need to write a novel.
-
- But you do need to document:
- Pertinent positives and negatives
- Your clinical reasoning (especially in key decisions)
- Discharge instructions
- But you do need to document:
- Defensive medicine is not the answer.
-
- ➡️ It is not good medicine.
- ➡️ It does not reliably prevent complaints.
- ➡️ And it can cause real harm to patients.
References
Baines v Abounaja, 84070/13 (Superior Court of Justice March 31, 2023). https://canlii.ca/t/jxjhz
Cahill, P. (2023, June 9). Baines v Abounaja – Amputation From Pulseless Leg Transfer Delay | Paul Cahill Medical Malpractice Lawyer. https://paulcahill.ca/baines-v-abounaja-amputation-from-pulseless-leg-transfer-delay/
CMPA. (2022.). Being on call when resources are limited. CMPA. Retrieved April 7, 2025, from https://www.cmpa-acpm.ca/en/advice-publications/browse-articles/2008/being-on-call-when-resources-are-limited
CMPA. (2023). CMPA – Medico-legal risk: What physicians working in emergency medicine need to know. CMPA. https://www.cmpa-acpm.ca/en/research-policy/know-your-risk/what-physicians-working-in-emergency-medicine-need-to-know
CMPA. (2024). What to do if you’re notified of a College complaint. CMPA. https://www.cmpa-acpm.ca/en/advice-publications/browse-articles/2018/what-to-do-if-you-re-notified-of-a-college-complaint
CMPA – 2023 Annual Report. (n.d.). CMPA. Retrieved January 28, 2025, from https://www.cmpa-acpm.ca/en/about/annual-report/2023-cmpa-annual-report
Cortel-LeBlanc, M. A., Lemay, K., Woods, S., Bakewell, F., Liu, R., & Garber, G. (2023). Medico-legal risk and use of medical directives in the emergency department. CJEM, 25(7), 589–597. https://doi.org/10.1007/s43678-023-00522-1
CPSO – Alternative Dispute Resolution. (n.d.). Retrieved April 7, 2025, from https://www.cpso.on.ca/en/Public/Services/Complaints-and-Concerns/Alternative-Dispute-Resolution
CPSO – Annual Report. (n.d.). Retrieved April 4, 2025, from https://www.cpso.on.ca/en/News/Publications/Annual-Report
CPSO – Complaints and Concerns. (n.d.). Retrieved March 8, 2025, from https://www.cpso.on.ca/en/Public/Services/Complaints-and-Concerns
Crosbie, C., McDougall, A., Pangli, H., Abu-Laban, R. B., & Calder, L. A. (2022). College complaints against resident physicians in Canada: A retrospective analysis of Canadian Medical Protective Association data from 2013 to 2017. Canadian Medical Association Open Access Journal, 10(1), E35–E42. https://doi.org/10.9778/cmajo.20210026
Ep #84 – What happens if I get sued as a physician in Canada? With Dr. Todd Watkins, Associate CEO of the CMPA. (2025, February 6). [Audio recording]. https://open.spotify.com/episode/2Xf3i2vr1fHRwQxk6J1Wed
Haroutunian, P., Alsabri, M., Kerdiles, F. J., Adel Ahmed Abdullah, H., & Bellou, A. (2018). Analysis of Factors and Medical Errors Involved in Patient Complaints in a European Emergency Department. Advanced Journal of Emergency Medicine, 2(1), e4. https://doi.org/10.22114/AJEM.v0i0.34
Limited healthcare resources: The difficult balancing act. (2022). CMPA. https://www.cmpa-acpm.ca/en/advice-publications/browse-articles/2007/limited-health-care-resources-the-difficult-balancing-act
Medico-legal handbook for physicians in Canada. (n.d.). CMPA. Retrieved January 14, 2025, from https://www.cmpa-acpm.ca/en/advice-publications/handbooks/medical-legal-handbook-for-physicians-in-canada
Neilson, H. K., Fortier, J. H., Finestone, P. J., Ogilby, C. M., Liu, R., Bridges, E. J., & Garber, G. E. (2023). Diagnostic Delays in Sepsis: Lessons Learned From a Retrospective Study of Canadian Medico-Legal Claims. Critical Care Explorations, 5(2), e0841. https://doi.org/10.1097/CCE.0000000000000841
Smith, J. D., Lemay, K., Lee, S., Nuth, J., Ji, J., Montague, K., & Garber, G. E. (2023). Medico-legal issues related to emergency physicians’ documentation in Canadian emergency departments. Canadian Journal of Emergency Medicine, 25(9), 768–775. https://doi.org/10.1007/s43678-023-00576-1
Sutherland et al. v. Booth, 26898/15 (Superior Court of Justice January 8, 2024). https://canlii.ca/t/k24gw
