
The 2025 American Heart Association Guidelines for Cardiopulmonary Resuscitation (CPR) and Emergency Cardiovascular Care (ECC) introduce several important updates across the resuscitation spectrum. Below is a concise, clinically focused summary tailored for emergency medicine physicians.

Neonatal Life Support
Umbilical Cord Management
-
For term and preterm neonates in stable condition, defer cord clamping ≥ 60 s.
-
For non-vigorous neonates 35–42 weeks, intact-cord milking may be considered as an adjunct.
Ventilation and Airway
-
Initiate PPV with peak pressures around 20–30 cm H₂O, titrating to adequate chest rise (standard NRP range; not a new AHA change).
-
Ventilation rate 30–60 breaths per minute (remains NRP practice).
-
Video laryngoscopy recognized as a useful tool for intubation.
-
Laryngeal mask airway is appropriate when face-mask ventilation fails and may be used first-line in some settings (the ≥ 34-week threshold comes from NRP device sizing, not the AHA text).
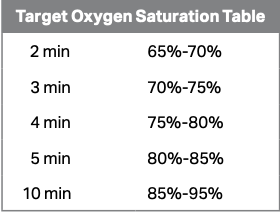
Oxygen Therapy
-
Apply pulse oximetry early and titrate FiO₂ to time-based SpO₂ targets rather than a fixed 30–100 % range.
Chest Compressions
-
Compress over the lower third of the sternum, avoiding the xiphoid process.
Pediatric Basic Life Support
CPR Technique
-
Limit interruptions to < 10 s.
-
Use the two-thumb encircling method (or heel of one hand). The two-finger technique is no longer recommended.
Foreign Body Airway Obstruction (FBAO)
-
Children: alternate 5 back blows and 5 abdominal thrusts.
-
Infants: alternate 5 back blows and 5 chest thrusts (abdominal thrusts not recommended).
Adult Basic Life Support
Airway Management
-
If jaw-thrust fails in trauma, head-tilt–chin-lift is acceptable despite cervical-spine concerns.
Ventilation
-
Deliver enough tidal volume for visible chest rise while prioritizing high-quality compressions.
Compression-Ventilation Ratio
-
Continue standard 30:2 compressions-to-breaths; asynchronous ventilations only after advanced airway placement.
Mechanical CPR
-
Routine use is discouraged; may be considered when manual CPR is unsafe or impractical.
FBAO
-
Repeat 5 back blows followed by 5 abdominal thrusts until cleared or unresponsive.
Pediatric Advanced Life Support (PALS)
Drug Administration
-
In cardiac arrest with non-shockable rhythms, give epinephrine as early as possible, then every 3–5 min.
Monitoring During CPR
-
EtCO₂ and arterial diastolic pressure help assess quality and detect ROSC.
-
Targets: ≥ 25 mm Hg (infants) and ≥ 30 mm Hg (children > 1 year).
-
No single parameter should guide termination of resuscitation.
-
SVT Management
-
If vagal maneuvers, adenosine, and cardioversion fail, consider IV procainamide or amiodarone.
Post-Arrest Care
-
Maintain systolic and mean arterial pressures above the 10th percentile for age.
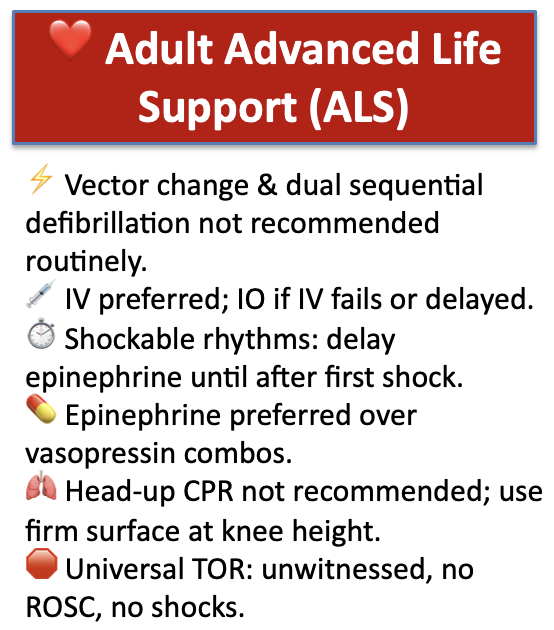
Adult Advanced Life Support (ALS)
Defibrillation
-
Vector change and dual sequential defibrillation are not recommended for routine use in refractory VF/pulseless VT (utility uncertain).
Vascular Access
-
IV preferred; IO if IV access fails or is delayed.
Vasopressors
-
In shockable rhythms, delay epinephrine until after initial defibrillation.
-
Epinephrine alone is preferred over combinations with vasopressin.
CPR Positioning
-
Head-up CPR not recommended outside clinical trials.
-
Perform compressions on a firm surface at rescuer knee height when possible.
Termination of Resuscitation
-
The Universal TOR Rule applies (arrest not witnessed by EMS, no ROSC, no shocks).
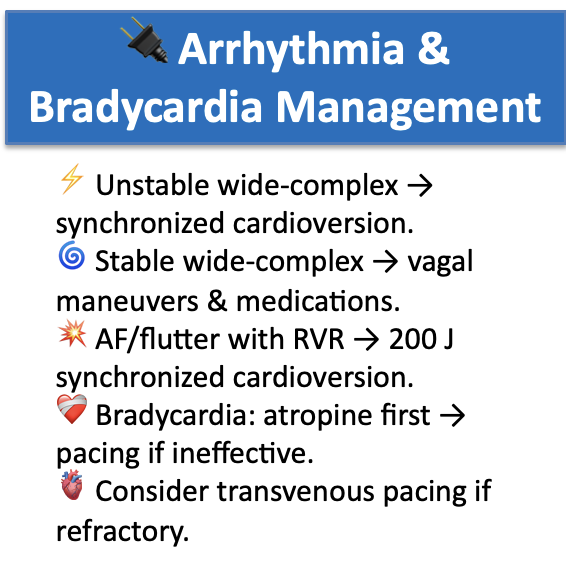
Arrhythmia Management
-
Wide-complex tachycardia with instability: synchronized cardioversion.
-
Stable wide-complex: attempt vagal maneuvers and pharmacologic therapy.
AF / Flutter with RVR
-
Use 200 J for synchronized cardioversion; avoid low-energy shocks and double cardioversion.
Bradycardia
-
Atropine first; if ineffective, initiate transcutaneous pacing.
-
Transvenous pacing is reasonable when bradycardia persists despite TCP and medical therapy (with expert consultation).
Post-Cardiac Arrest Care
Hemodynamics
-
Maintain MAP ≥ 65 mm Hg; avoid hypotension.
Diagnostics
-
Whole-body CT (from head to pelvis) may be considered after stabilization to identify arrest etiology or resuscitation-related injury.
Temperature Control
-
Maintain core temperature 32–37.5 °C for ≥ 36 h in patients not following commands.
Myoclonus and Seizure Management
-
Obtain EEG to evaluate for seizures.
-
Treat confirmed seizures; avoid prognosticating based on myoclonus alone.
Cardiac Arrest in Special Circumstances
Asthma
-
Consider ECLS or inhaled volatile anesthetics if standard therapy fails.
Hyperkalemia
-
Continue standard ACLS management (IV calcium for ECG changes, insulin/glucose, β-agonists, bicarbonate as indicated). The AHA did not de-prioritize calcium.
Hypothermia
-
Consider ECLS for profound hypothermia (core < 28 °C) when resources allow; HOPE and ICE scores are external decision aids, not formal AHA recommendations.
Hyperthermia
-
Rapid cold-water immersion (1–5 °C) is recommended for exertional heat stroke; cool as rapidly as possible (no specific rate given by AHA).
LVAD Patients
-
If unresponsive with impaired perfusion, begin CPR while troubleshooting the device. Read more on LVADs here.
Pregnancy
-
Initiate resuscitative hysterotomy immediately upon recognition of cardiac arrest with the goal of delivery ≤ 5 min.
-
Consider ECPR if standard resuscitation fails.
-
Use a balanced massive transfusion for suspected amniotic fluid embolism.
Opioid Overdose
-
Naloxone may be given for suspected opioid-related cardiac arrest, but must not delay standard CPR and epinephrine administration.
References
-
American Heart Association. 2025 Highlights of the Guidelines for CPR and ECC.
-
AHA Algorithms: Adult BLS, Adult ALS, PALS, Post-Cardiac Arrest Care (2025 update).
-
EMOttawa Blog: Braving the Electrical Storm in the ED (2020).