

There seems to be a growing cultural obsession with “inflammation”. Scroll through social media long enough and you’ll find sweeping claims: inflammation is the root of fatigue, weight gain, menstrual cramps, brain fog, and even depression. And alongside this obsession is the belief that there’s no such thing as too many tests, and that ordering non-specific tests like ESR and CRP is always helpful and never harmful. That testing is in inherently good.
As emergency physicians, we are the stewards of diagnostic testing. And inflammatory markers — ESR and CRP in particular — are some of the most misunderstood, overinterpreted, and misapplied tests we order.
What Are We Actually Measuring?
The term inflammation dates back to Aulus Cornelius Celsus, who described the cardinal signs rubor, calor, tumor, and dolor.
Broadly speaking, inflammatory markers (more accurately called acute phase reactants) are proteins whose plasma concentrations change by at least 25% during inflammatory states. There are many:
- C-reactive protein (CRP)
- Erythrocyte sedimentation rate (ESR)
- Ferritin
- Fibrinogen
- Serum amyloid A
- Procalcitonin
- Complement components
- Cytokines such as IL-6 and TNF-α
But in the ED, when we’re talking about inflammatory markers we mostly mean ESR and CRP.
CRP
CRP is synthesized in the liver in response to IL-6. It rises quickly and has a relatively short half-life (~7 hours). It increases in response to infection, inflammation, trauma, malignancy, and tissue necrosis.
It is also elevated in:
- Pregnancy
- Obesity
- Smoking
- Obstructive sleep apnea
- Oral contraceptive use
- Chronic disease
- Even social and psychosocial factors
CRP is sensitive, but not specific.
ESR
ESR measures how quickly red blood cells sediment in a vertical tube over one hour. It is influenced largely by fibrinogen levels. It rises more slowly than CRP and peaks later (around day 7).
ESR is affected by:
- Age
- Female sex
- Anemia
- Kidney disease
- Pregnancy
- Smoking
Again, ESR is sensitive, but not specific.
The Bayesian Problem
Inflammatory markers are particularly prone to misuse because they are high sensitivity, low specificity tests. Bayesian reasoning reminds us that a test result only has meaning when interpreted in the context of pre-test probability.
We do this constantly in the ED. Two patients present with pleuritic chest pain:


One gets a CT pulmonary angiogram, the other is diagnosed with musculoskeletal pain. Same symptom, different pre-test probabilities, different decisions.
The same applies to inflammatory markers.
If the pre-test probability is extremely low, a positive CRP creates noise.
If the pre-test probability is extremely high, a negative CRP may not meaningfully change management.
Inflammatory markers are most useful in the low-to-moderate pre-test probability zone, where a negative result meaningfully lowers disease likelihood.
When Are Inflammatory Markers Actually Helpful?
1. Diabetic Foot Infections
Case: A 65 year old man with poorly controlled TIIDM presents with an infected ulcer on his toe. He has recurrent history of infected foot ulcers. There is erythema extending >3cm around the ulcer, and you cannot probe to bone. His xray does not show any signs of osteomyelitis, but you are still suspicious. You order an ESR and it is 10, and his CRP is 3. How does that help you?
In 2023, the International Working Group on the Diabetic Foot and the Infectious Disease Society of America came out with new guidelines[1] on the diagnosis and management of infected diabetic foot ulcers and osteomyelitis. Although there is a multitude of very helpful information in here, as it pertains to the role of inflammatory markers, they make the following recommendations:
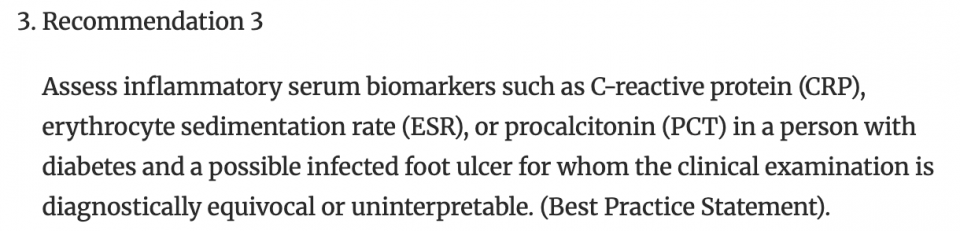
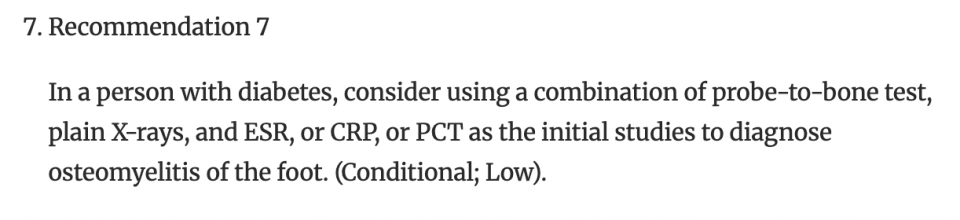
For osteomyelitis, ESR has a sensitivity of 70%, and a specificity of 77%. CRP has a sensitivity of 72% and a specificity of 76%.
Therefore ESR and CRP can meaningfully contribute, not because they diagnose osteomyelitis, but because, when combined with:
- Probe-to-bone testing
- Plain radiographs
- Clinical exam
A normal ESR and CRP can substantially lower post-test probability. So, moving back to our case, in this patient with a negative probe to bone test, a normal xray, and normal inflammatory markers, you have significantly reduced the likelihood that this infected foot ulcer overlies an osteomyelitis.
Take home point:
- ESR and CRP should be ordered in infected foot ulcers if:
- Grade 4 or 4O severity of diabetic foot infection
- You suspect osteomyelitis despite a normal xray
- The diagnosis of diabetic foot ulcer is unclear (this should not happen very often).
2. Giant Cell Arteritis
Case: A 75 year old woman presents to the emergency department with two months of a headache. It is pulsating, and she reports that her jaw gets tired when she eats or talks. You suspect GCA. You decide to order inflammatory markers.
Inflammatory markers are frequently elevated in GCA, but like in other conditions, they are sensitive but not specific.
A recent meta-analysis demonstrated that the sensitivity of CRP was in the 87.4, with a specificity of 31.4. ESR was similar, with a sensitivity of 82.6 and specificity of 33.8.
So, how do we apply this? In our patient who is elderly with classic symptoms of GCA, our pretest probability might be in the 75% range. If she has a positive CRP, her post-test probability only improves to 79%, which is not very helpful. If it is negative, her post-test probability is 56%. Given that the risk is of loss of vision, this is insufficient to adequately rule out GCA. This is why the recommendation is that even with negative inflammatory markers, people are started on treatment and referred to ophthalmology. this occurs in roughly 3% of patients, so it is uncommon.
But let’s say it was a different patient, and your pre-test probability was lower, say 25%, your post-test probability would 12%, which, depending on your risk tolerance, might be low enough to state that this patient does not have GCA. This demonstrates that inflammatory markers are better at ruling out GCA in someone with low to moderate pre-test probability.
Key takeaway:
- ESR and CRP should be ordered in the work up of GCA, but know how to interpret them
- Negative inflammatory markers do not rule out GCA.
- In someone with low pre-test probability, negative inflammatory markers make the diagnosis much less likely
- Inflammatory markers can be elevated in many different conditions, so order them with caution.
3. Inflammatory Bowel Disease (IBD)
Undifferentiated Chronic Diarrhea
In patients being referred to GI for suspected IBD, fecal calprotectin – an inflammatory marker specific for GI inflammation – is the more useful test. It reflects neutrophilic intestinal inflammation and helps triage referrals.
Known Ulcerative Colitis Flare
In moderate-to-severe presentations, the pre-test probability of endoscopic inflammation is already high (~85%). A normal CRP does not rule out a flare.
CRP is better used for:
- Prognostication
- Monitoring response
- Supporting severity assessment
And importantly: CT scans are rarely indicated in uncomplicated ulcerative colitis flares. Prevalence of surgical complications is extremely low (<3%).
4. Back Pain
Back pain presentations to the emergency department represent a significant amount of the visits we see each shift. Most of these are low risk, mechanical back pain. However, back pain can also be an a sign of something insidious, some of which includes pyogenic spinal infections.
Spinal infections includes pathologies such as SEA, vertebral osteomyelitis, septic facet joint, paravertebral abscess and paraspinal abscess.
Studies suggest that ESR <20 and CRP <10 are highly sensitive for spinal infection. But these were retrospective cohorts of patients already selected for MRI, which biases towards cases with a higer pre-test probability and might over-inflate the sensitivity.
Given that the sensitivity of these markers is not 100, and the risk of missing one of these infections is devastating, it is recommended to only use inflammatory markers to rule out a pyogenic spinal infection if you feel someone to be low risk. The IDSA Native Vertebral Osteomyelitis Guidelines supports ESR/CRP as sensitive screening tools but still states that an MRI should be ordered in patients with suspected spinal infection
However a word of caution. Inflammatory markers are helpful in patients you judge to be low-to-moderate risk — not in every patient with back pain and diabetes.
A mildly elevated CRP in a 75-year-old with mechanical back pain is far more likely to reflect chronic inflammation than a spinal epidural abscess.
5. Pericarditis
Case: You see a 45 year old male presents with chest pain. He had a viral infection two weeks ago. He has sharp, pleuritic chest pain that is relieved by sitting up or learning forward. His ECG shows some PR depression but no significant ST elevation. He has no pericardial effusion or friction rub – you wonder, does he have pericarditis?
This year, the American College of Cardiology published novel diagnostic criteria for acute pericarditis that includes the use of inflammatory markers in the diagnosis
These new criteria are also supported by the European Society of Cardiology.
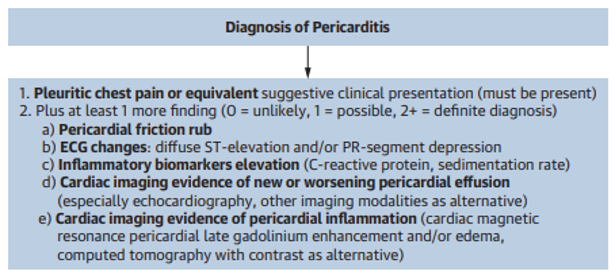
The new criteria emphasized the importance of typical chest pain, and then adds a value of unlikely, possible and definite diagnosis.
Going back to our case, inflammatory markers might be elevated in this patient because of his recent viral infection. However, given the fact that he has typical symptoms, as well as ECG changes, if his inflammatory markers were elevated that would change his diagnosis from possible pericarditis to definite.
Read more on the assessment and management of pericarditis and myocarditis here.
Take home points:
- There are new diagnostic criteria for pericarditis, which include inflammatory markers
- The diagnosis of pericarditis is made with a strongly suggestive clinical history and one other objective feature – either inflammatory marker elevation, ECG changes, pericardial effusion, friction rub, or imaging evidence of pericardial inflammation
The TL/DR;
Inflammatory markers:
- Are highly sensitive
- Are poorly specific
- Shift probabilities
- Do not diagnose disease
They are most useful when:
- You have a clear clinical question
- Pre-test probability is low-to-moderate
- The result will meaningfully change management
They are least useful when:
- You are ordering them reflexively
- Pre-test probability is very low
- Pre-test probability is already extremely high
The belief that “more testing is always better” is seductive. But every test introduces noise, false positives, incidental findings, anxiety and further testing.
Bayesian thinking protects our patients from that cascade.
Inflammatory markers are neither inherently good nor inherently harmful, but another set of tools at our disposal. It’s our responsibility to use them wisely.
References
Alharthi, A. H., Al-Shehri, S. H. A., Albarqi, M. A. A., Alshehri, M. S., Alshehri, A. M., Amer, A. M., … & Alassiry, A. M. A. (2024). Laboratory markers of inflammation: CRP and ESR in clinical practice. Journal of International Crisis and Risk Communication Research, 7(S8), 2376.
Ansar, W., & Ghosh, S. (2016). Inflammation and inflammatory diseases, markers, and mediators: Role of CRP in some inflammatory diseases. In Biology of C reactive protein in health and disease (pp. 67–107). Springer India.
Ashby, D. (2006). Bayesian statistics in medicine: A 25-year review. Statistics in Medicine, 25(21), 3589–3631.
Berbari, E. F., Kanj, S. S., Kowalski, T. J., Darouiche, R. O., Widmer, A. F., Schmitt, S. K., … & Osmon, D. R. (2015). Executive summary: 2015 Infectious Diseases Society of America (IDSA) clinical practice guidelines for the diagnosis and treatment of native vertebral osteomyelitis in adults. Clinical Infectious Diseases, 61(6), 859–863.
Carpenter, C. R., Raja, A. S., & Brown, M. D. (2015). Overtesting and the downstream consequences of overtreatment: Implications of “preventing overdiagnosis” for emergency medicine. Academic Emergency Medicine, 22(12), 1484–1492.
Chan, F. L. Y., Lester, S., Whittle, S. L., & Hill, C. L. (2019). The utility of ESR, CRP and platelets in the diagnosis of GCA. BMC Rheumatology, 3(1), 14.
Chandrashekara, S. (2014). C-reactive protein: An inflammatory marker with specific role in physiology, pathology, and diagnosis. Internet Journal of Rheumatology and Clinical Immunology, 2(S1).
Davis, W. T., April, M. D., Mehta, S., Long, B., & Shroyer, S. (2020). High risk clinical characteristics for pyogenic spinal infection in acute neck or back pain: Prospective cohort study. The American Journal of Emergency Medicine, 38(3), 491–496.
Gonzalez-Gay, M. A., Lopez-Diaz, M. J., Barros, S., Garcia-Porrua, C., Sanchez-Andrade, A., Paz-Carreira, J., Martin, J., & Llorca, J. (2005). Giant cell arteritis: Laboratory tests at the time of diagnosis in a series of 240 patients. Medicine, 84(5), 277–290. https://doi.org/10.1097/01.md.0000180043.19285.54
Gutovitz, S., Blaskowsky, J., Lindstrom, D., Arnold, D., Hardin, J., Montgomery, K. M., & Roshan, L. (2025). An assessment of C-reactive protein and erythrocyte sedimentation rate in ruling out acute infectious spinal pathology in emergency department patients: A retrospective cohort study. JACEP Open, 6(4), 100213.
IWGDF/IDSA Guidelines on the Diagnosis and Treatment of Diabetes-related Foot Infections. (2023).
Kermani, T. A., Schmidt, J., Crowson, C. S., Ytterberg, S. R., Hunder, G. G., Matteson, E. L., & Warrington, K. J. (2012). Utility of erythrocyte sedimentation rate and C-reactive protein for the diagnosis of giant cell arteritis. In Seminars in Arthritis and Rheumatism (Vol. 41, No. 6, pp. 866–871). WB Saunders.
Ma, C., Battat, R., Khanna, R., Parker, C. E., Feagan, B. G., & Jairath, V. (2019). What is the role of C-reactive protein and fecal calprotectin in evaluating Crohn’s disease activity? Best Practice & Research Clinical Gastroenterology, 38, 101602.
Marshall, J. C., & Aarts, M. A. (2001). From Celsus to Galen to Bone: The illnesses, syndromes, and diseases of acute inflammation. In Yearbook of Intensive Care and Emergency Medicine 2001 (pp. 3–12). Springer Berlin Heidelberg.
Singh, S., Ananthakrishnan, A. N., Nguyen, N. H., Cohen, B. L., Velayos, F. S., Weiss, J. M., … & AGA Clinical Guidelines Committee. (2023). AGA clinical practice guideline on the role of biomarkers for the management of ulcerative colitis. Gastroenterology, 164(3), 344–372.
Tversky, A., Kahneman, D., & Slovic, P. (1982). Judgment under uncertainty: Heuristics and biases (pp. 3–20).
van der Geest, K. S., Sandovici, M., Brouwer, E., & Mackie, S. L. (2020). Diagnostic accuracy of symptoms, physical signs, and laboratory tests for giant cell arteritis: a systematic review and meta-analysis. JAMA internal medicine, 180(10), 1295-1304
Wang, T. K. M., Klein, A. L., Cremer, P. C., Imazio, M., Kohnstamm, S., Luis, S. A., … & Wohlford, G. F. (2025). 2025 concise clinical guidance: An ACC expert consensus statement on the diagnosis and management of pericarditis: A report of the American College of Cardiology Solution Set Oversight Committee. Journal of the American College of Cardiology.
Zipkin, D. A., Umscheid, C. A., Keating, N. L., Allen, E., Aung, K., Beyth, R., … & Feldstein, D. A. (2014). Evidence-based risk communication: A systematic review. Annals of Internal Medicine, 161(4), 270–280.