
Acute Liver Failure (ALF) is rare, with an estimated incidence of 1–6 cases per million per year in Western countries¹². Despite its rarity, it carries significant morbidity and mortality¹. ALF most often affects previously healthy adults in their 30s; in North America, the median age is 38¹. Roughly 50% survive without transplant, 25% undergo transplant (with ~95% survival), and 25% die without transplantation¹.
Early recognition is essential¹². Improvements in specialty care have increased overall and transplant free survival¹, but timely diagnosis, stabilization, and referral to a transplant center remain critical¹². Early ED recognition has meaningful downstream impact¹.
Part 1 – Recognition and Workup of Acute Liver Failure
Definition
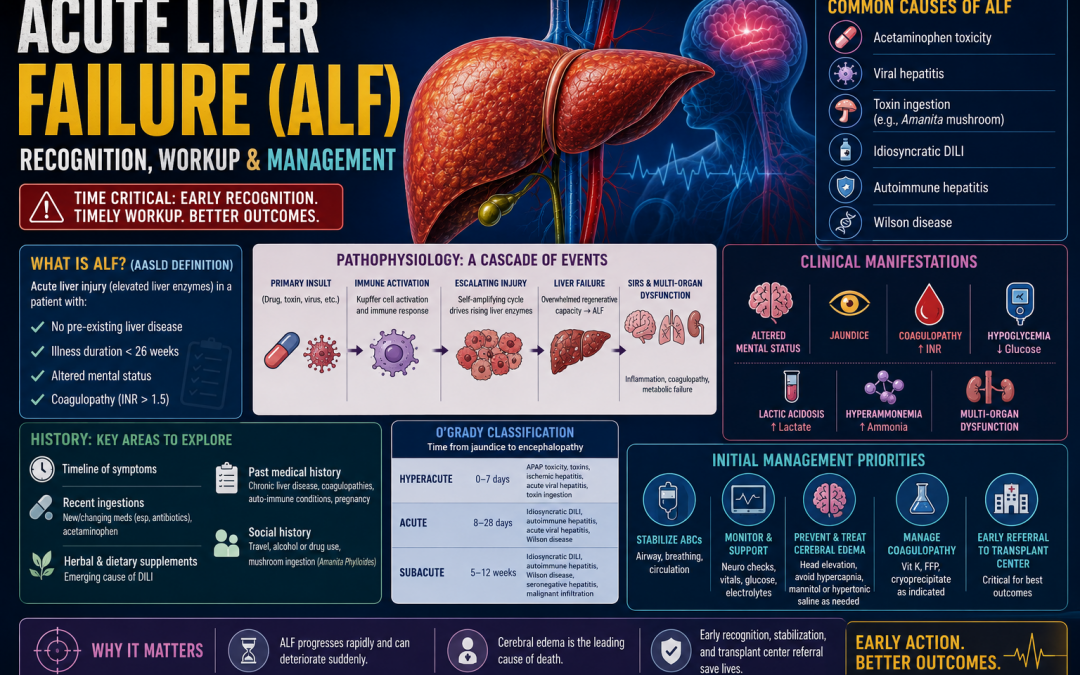
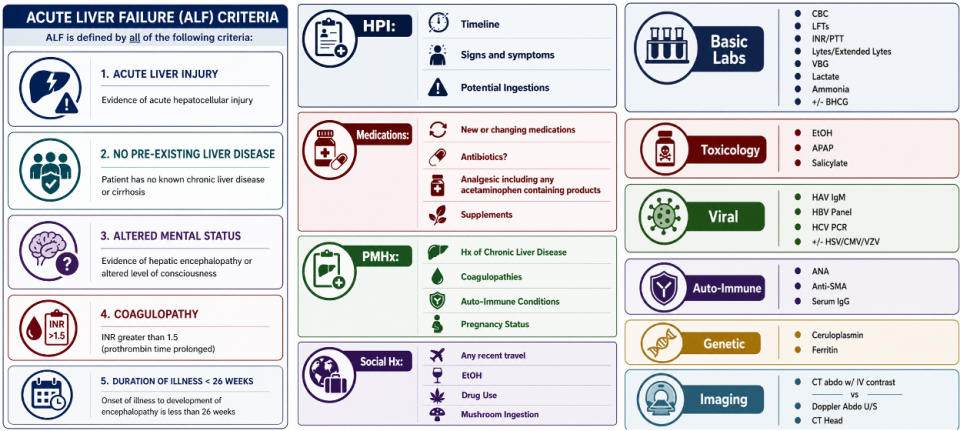
To recognize Acute Liver Failure, we first need to be able to define it. The most widely accepted definition comes from the American Association for the Study of Liver Diseases (AASLD) who define ALF as acute liver injury (elevated liver enzymes) in a patient with³:
- No pre existing liver disease
- Illness duration <26 weeks
- Altered mental status
- Coagulopathy (INR >1.5)
Exceptions include Budd Chiari syndrome, autoimmune hepatitis, and Wilson disease³⁴, where chronic disease may be present but cirrhosis is absent clinically and histologically.
Acute liver Failure is NOT:
-
-
- Alcoholic hepatitis: these patients typically have chronic alcohol use and structurally abnormal livers³⁴.
- Acute decompensated cirrhosis: these patients differ markedly from ALF in baseline liver function, etiologies, precipitants, workup, management, and complications³⁴.
-
Pathophysiology
ALF begins with a primary hepatocellular insult (drug, toxin, virus), triggering Kupffer cell activation and an escalating immune response (“secondary injury”)⁵⁶. This self amplifying cycle drives rising liver enzymes⁵. Normally, the liver is able to respond to this insult but when this regenerative capacity is overwhelmed, uncontrolled liver injury ensues, leading to Acute Liver Failure⁵.
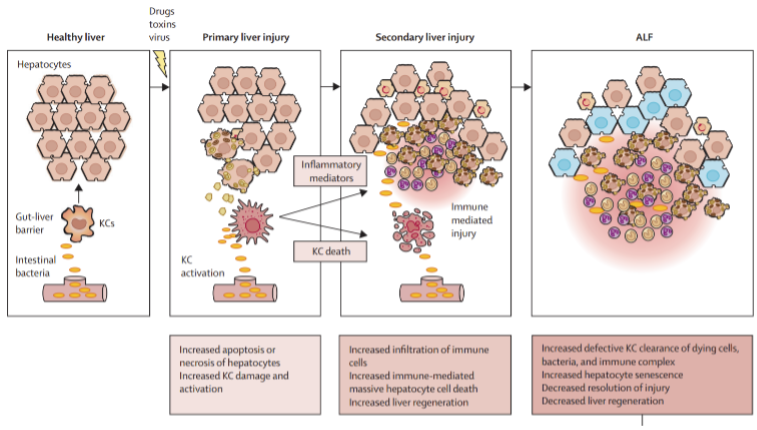
Image Source: Acute Liver Failure – The Lancet⁵
The resulting inflammatory cascade produces a SIRS‑like state and multi‑organ dysfunction.56
Loss of hepatic metabolic function lead to hypoglycemia, lactic acidosis and hyperammonemia. Bilirubin will also be elevated due to decreased update, conjugation and excretion as well as leaking of bilirubin from hepatocytes, resulting in jaundice.
Coagulopathy is a result of decreased hepatic synthesis of clotting factors as the liver synthesizes all clotting factors with the exception of von Willebrand factor and factor VIII. This leads to elevation in INR.5
The brain is the most frequently affected organ in ALF and cerebral edema is the leading cause of death in these patients. It is the combination of this SIRS response leading to leaky capillaries and cerebral vasodilation as well as the accumulation of toxins, notably ammonia, that is hypothesized to lead to cerebral edema in these patients. 56
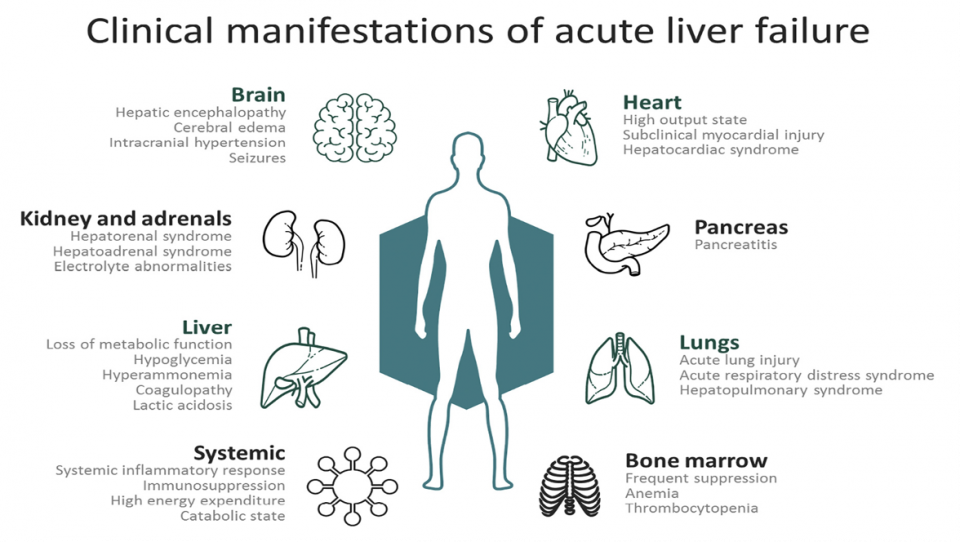
Image Source: T. Montrief et al. / American Journal of Emergency Medicine⁶
Compared to ALF, cirrhosis has a much slower course, with gradual loss of hepatocytes from chronic inflammation, and progressive fibrosis. This leads to both structural and dynamic obstruction through the liver and subsequent portal hypertension, a phenomenon that is not seen in ALF. This portal hypertension leads to ascites and varices, neither of which are seen in ALF.
While hepatic encephalopathy is seen in both patients with ALF and cirrhosis, the underlying etiologies differ. In cirrhosis, HE is driven by elevated ammonia levels but does not have a linear relationship with the measured value. These patients have chronic, low-grade swelling and inflammation of astrocytes which, when a precipitant such as infection is present, leads to HE. ALF patients are not preconditioned to cope with hyperammonemia and are therefore more susceptible to intracranial hypertension. In these patients, measuring an ammonia level has value as there is a much more linear relationship between ammonia levels and degree of hepatic encephalopathy in these patients.56
Clinical Assessment
History
A thorough history should be taken with an emphasis on establishing the timeline of the patient’s symptoms as this can help point towards the potential cause. History should also focus on recent ingestions including any new or changing medications, in particular antibiotics as these are the most common cause of drug induced liver injury after acetaminophen containing products. Patients should also be asked about dietary supplements which are an emerging cause of drug induced liver injury.
Patient’s past medical history should be reviewed to determine if patient has a history of chronic liver disease, coagulopathies, auto-immune conditions and to assess if they are pregnant.
Finally, a social history should be taken to assess for any recent travel, any alcohol or drug use or any mushroom ingestion, in particular Amanita Phylloides.
The O’Grady classification divides ALF into hyperacute, acute, and subacute based on time from jaundice to encephalopathy. APAP toxicity and toxins tend to be hyperacute; idiosyncratic DILI and autoimmune hepatitis tend to be subacute.
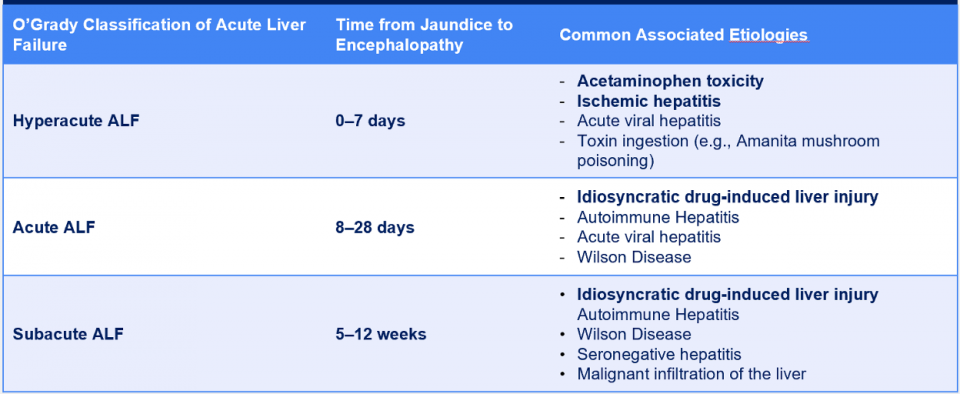
Similarly, while hyperacute etiologies of acute liver failure present more dramatically with high rates of cerebral edema, paradoxically they carry a lower risk of transplant and death. This is because hyperacute etiologies typically involve a single, time-limited insult; a bolus of acetaminophen, a transient ischemic event, or a self-limited viral infection. Once the offending agent is cleared or the insult resolves, the injury stops and the liver can begin to recover.
In contrast, subacute etiologies (idiosyncratic DILI, indeterminate causes) involve ongoing, smoldering hepatocyte destruction over weeks, which continuously undermines the regenerative response. This progressive destruction results in lower likelihoods of hepatic recovery. As such, despite subacute ALF presenting significantly less dramatically, these patients are more likely to require transplant and ultimately have a higher mortality. 57
Physical Exam
A full exam is important, though many findings lack sensitivity or specificity. Mental status assessment is key. Findings help grade hepatic encephalopathy using the West Haven Criteria, which guides management:
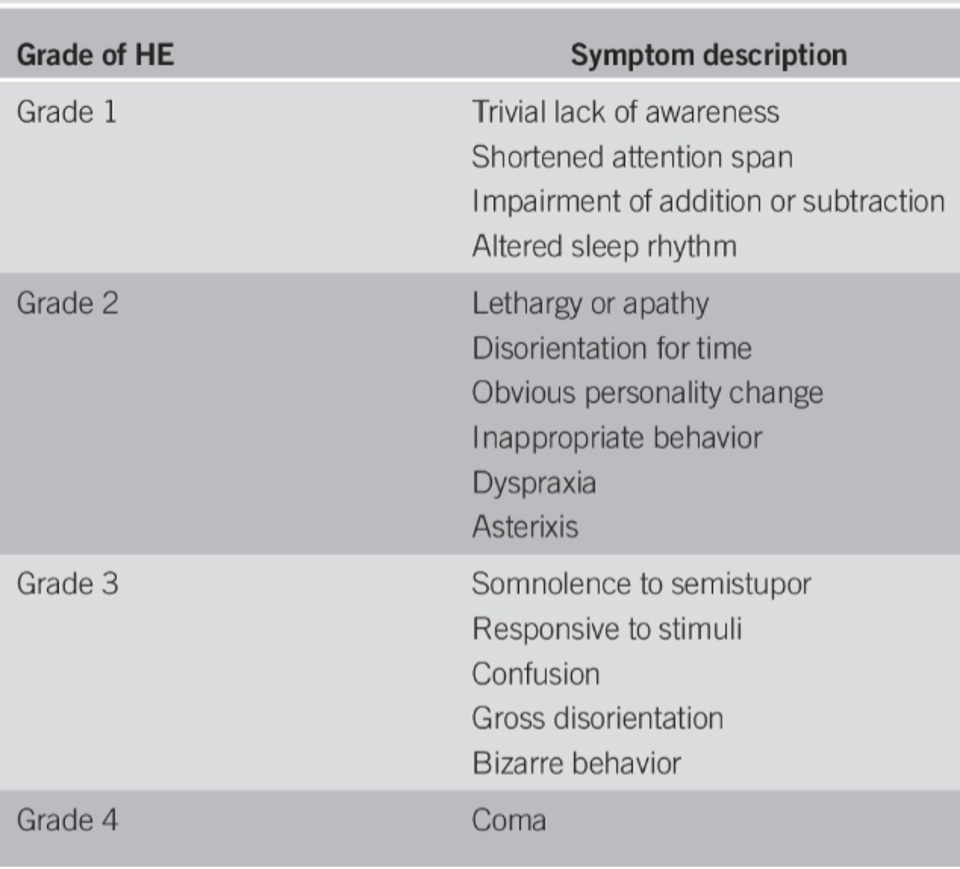
Table source: American College of Gastroenterology. ACG Clinical Guideline: Acute Liver Failure. Am J Gastroenterol. 2023;118:1128–1153.
Workup
- Most of these patients will already have a CBC, Chem 7, LFTs, Coags and a VBG drawn, either at triage or as part of nursing directive.
- Unlike in patients with cirrhosis where Ammonia levels have little utility or predictive value, in patients with ALF, ammonia levels correlate more directly with cerebral complications and can help dictate need for dialysis. 56
- I will also emphasize the importance of a BHCG in patients with a uterus, as pregnancy is a risk factor for some of the conditions highlighted here.
- Additionally, most guidelines assume that a CT head has been ordered on presentation for altered LOC, although these are not ED guidelines and again, data for this population is limited. My recommendation would therefore be, in patients with mild aLOC, use your clinical judgement to assess likelihood of alternative explanations and decide accordingly. In patients, with severely decreased GCS, the yield may be higher, as is the need to rule out alternative causes.
1000’s Club
The 1000s Club refers to a group of etiologies causing acute liver injury classically associated with an AST or ALT greater than 1000. The original members of this club included Toxin associated ALF, Ischemic ALF and Viral ALF.
In North America, the most common causes of Drug Induced liver Injury (DILI) other than acetaminophen are antimicrobials (Notably Clavulin, Septra, Isoniazid and Macrobid) and Herbal and Dietary Supplements.
A 2023 systematic review and meta-analysis (7 studies, n=1,608 patients with transaminases >1,000 IU/L) found the following pooled frequencies:
- Ischemic hepatitis: 51%
- Viral hepatitis: 13.1%
- Toxins/DILI: 13%
- Pancreaticobiliary causes: 7.8%
The classic triad therefore accounts for roughly ~77% of cases — meaning approximately 1 in 4–5 patients with transaminases >1,000 has a cause outside the traditional differential.9
So what accounts for the other 23%? Practically speaking, any process causing acute liver injury could potentially wind up with LFTs greater than 1000. This includes processes such as auto-immune hepatitis, pregnancy associated conditions and genetic conditions such as Wilson’s disease and hemochromatosis. 348
I do want to take a moment to shout out Dr Kaitlin Endres for her grand rounds on Splanchnic Vein Thrombosis and shock liver:
When it comes to Acute Liver Failure, we specifically care about Hepatic Vein thrombosis, otherwise known as Primary Budd-Chiari syndrome, which causes venous outflow track obstruction from the liver and therefore venous congestion. This venous congestion can cause ischemic liver injury by reducing portal vein flow. We should maintain a high degree of suspicion in patients who are hypercoagulable, including patients with underlying coagulopathies, pregnant patients and patients with underlying malignancy.
Understanding the most common causes of acute liver failure allows us to systematically and thoroughly workup these patients:
Toxin:
-
- EtOH
- APAP
- Salicylate Levels
- Medication review
Ischemic:
-
- Hepatic Vein Thrombosis: CT Abdo with IV contrast -> call rads to protocol.
Viral Hepatitis:
-
- Hep A, B and C serologies
- +/- HSV, CMV, VZV
Auto-Immune Hepatitis:
-
- ANA
- Anti-SMA
- Serum IgG
Pregnancy Associated Conditions:
-
- HELLP workup
Genetic Conditions:
-
- Ceruloplasmin -> Wilson’s Disease
- Ferritin -> Hemochromatosis
Summary
Recognizing that a patient has Acute Liver Failure can help rapidly and effectively mobilize consultants. Another way of thinking of this is that if a patient comes in and is altered and newly coagulopathy or jaundiced, we should we worried about ALF and liver enzymes should be added!
A careful history should be taken to establish timeline of symptoms, potential ingestions, contributory medical conditions and to exclude pre-existing liver failure.
A broad workup should be initiated to expedite the determination of the underlying cause as this carries important prognostic and management considerations.
Part 2 – ED Management of Acute Liver Failure
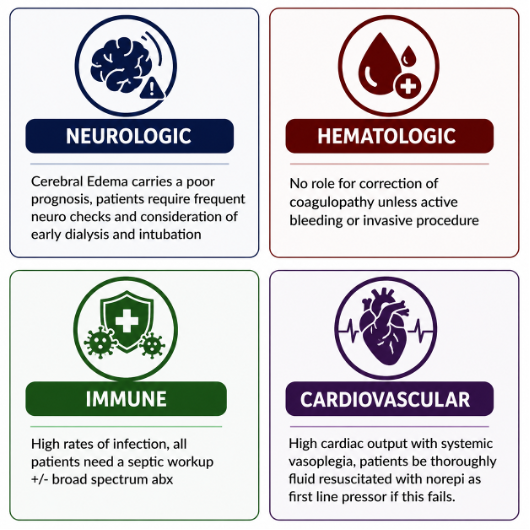
The most common cause of death in patients with acute liver failure is systemic complications, which follow the release of pro-inflammatory cytokines and damage to hepatocytes. While these processes impact almost every organ system, we will focus on supportive management of Neurologic, Cardiovascular, Hematologic and Immune complications, where we as Emergency Physicians can make the biggest impact.12
Neurologic
By definition, patients with ALF will have some degree of hepatic encephalopathy. As we have previously discussed this process is unique in ALF and is driven by the bodies inability to cope with hyperammonemia which leads to astrocyte swelling and cerebral edema. This is worsened by the underlying SIRS response which causes increased permeability of the blood brain barrier. Together, this makes patients with ALF more susceptible to cerebral edema and subsequent intracranial hypertension. Prevention and recognition of cerebral edema is important as it is the leading cause of death in ALF. 12
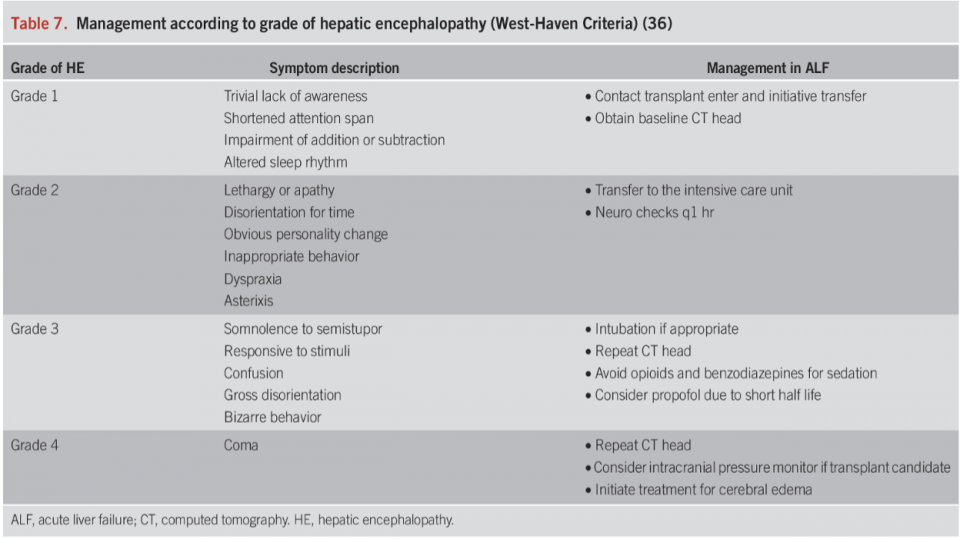
Table Source: American College of Gastroenterology. ACG ALF Guideline. Am J Gastroenterol. 2023;118:1128 1153.
Management of patient’s Neuro status depends on the Grade of Hepatic Encephalopathy12:
- Grade 2 Hepatic Encephalopathy (so all patients with disorientation and asterixis) should have an ICU consult for close neuromonitoring
- Grade 3 Hepatic Encephalopathy (so all patients with gross disorientation) should be considered for intubation. Intubation in these patients provides airway protection from aspiration, helps manage ICP, and helps facilitate other interventions such as dialysis.
- Grade 4 Hepatic Encephalopathy (so patients who are comatose) should be treated as having increased ICP.
Additionally, in their most recent 2023 Guidelines on ALF, the American College of Gastroenterology recommends that Dialysis be considered for patients with Hepatic Encephalopathy Grade 2 or above in the absence of other indications for Dialysis, given the benefit in treating hyperammonemia and reducing neurologic complications.
Therapies typically associated with hepatic encephalopathy in cirrhotic patients such as Rifaximin and Lactulose have not been shown to be of benefit.12
Cardiovascular
Patients in Acute Liver Failure present with comparable hemodynamics to patients with sepsis, with severe systemic vasodilation, high cardiac output and often hypovolemia in the setting of vomiting. As such, resuscitation should take similar principles with liberal fluid resuscitation and pressors where required. As with most forms of shock that we see in the ED, norepinephrine is the first line pressor, followed by vasopressin. Literature supporting MAP targets for these patients are variable; however, given the frequent underlying increased ICP, targeting a MAP of 70-80 may be beneficial.
Finally, although most evidence for this practice is extrapolated from research in Sepsis, patients with pressor refractory shock should receive a dose of Hydrocortisone given close to 50% have underlying adrenal insufficiency. 12
Hematologic
Coagulopathy in ALF is complex and not fully understood. While biochemically these patients are quite deranged, most patients are actually in a state of rebalanced hemostasis. Despite the frequently extreme elevation of the INR, INR is not an accurate predictor of bleeding risk in ALF. Additionally, clinically significant bleeding is actually uncommon in patients with ALF, accounting for less than 5% of deaths.
As such, there is no role for empirically treating coagulopathy derangements, in fact, this has been associated with increased harm. Guidelines across the board are very clear on this. If the patient is actively bleeding or undergoing an invasive procedure such as ICP monitoring, 4-Factor PCC and Fibrinogen should the first line. 12
Immune Function
Patients with ALF are in a state of multifactorial immunoparesis, in part due to decreased protection against gut bacteria, decreased immune complement secretion and decreased function of existing immune cells, to name a few.
Although the numbers vary, approximately 30% of patients with ALF had a superimposed bacterial illness. Unfortunately, these patients are also less likely to develop typical signs of infection such as fever or leukocytosis. 12
The effects of prophylactic antibiotics in this population has been studied in a large retrospective cohort report from Karvellas et al. The study reviewed 1,551 patients to examine the effects of prophylactic antimicrobials and development of blood stream infection. The results showed that antimicrobial prophylaxis did not reduce the rate of bloodstream infection or 21-day mortality. 10
So where does this leave us? Well, this was not an ED specific study and as such, does not necessarily apply to the ED management of undifferentiated patients but it’s important to recognize that the existing literature does not support this practice.
All patients should at minimum undergo a septic workup. Clear foci of infection should be treated with broad spectrum antibiotics but otherwise patients patients with ALF should not be given prophylactic abx in the ED.
Summary
NAC for Acute Liver Failure
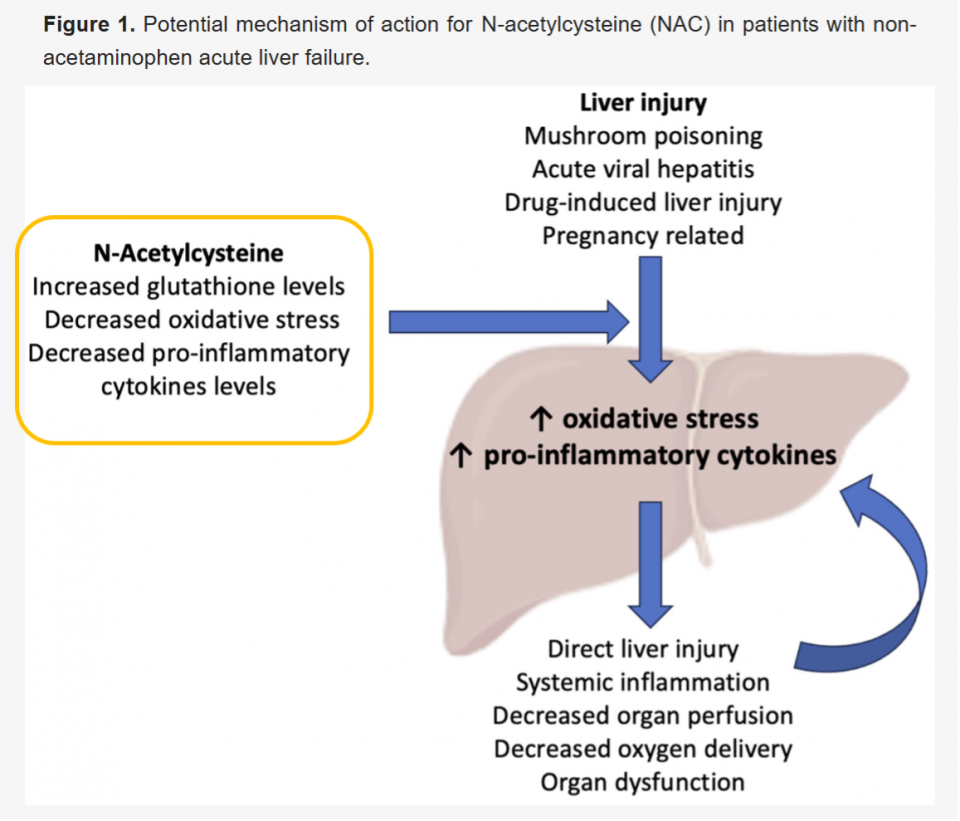
Source: The Use and Potential Benefits of N-Acetylcysteine in Non-Acetaminophen Acute Liver Failure: An Etiology-Based Review
N-acetylcysteine (NAC) has long been used as an antidote for acetaminophen or APAP overdose. Its pathophysiology is centered around the accumulation (NAPQI), which is normally metabolized by glutathione.
Toxic APAP doses deplete glutathione causing NAPQI to accumulate and cause liver injury. NAC restores glutathione, acting as a specific antidote for APAP overdose.
NAC also acts as a free-radial scavenger and has been shown to decrease oxidative stress.
These mechanisms have been hypothesized to be beneficial for patients with non-APAP ALF which makes sense, because ALF is a state of oxidative stress with a significant associated immune response. At a patient level however, the benefit is not as clear.13

Research supporting NAC for non-APAP Acute Liver Failure has evolved over the past 15 years.
- Interest began in 2009 with the landmark trial by Lee et al. The trial was a prospective, double-blind, multicenter trial randomized 173 adults with non-APAP ALF to IV NAC (72-hour infusion) vs. placebo. The trial showed that NAC improves transplant free survival in patients with low grade hepatic encephalopathy.
- Critically, this was a secondary outcome and no benefit for overall survival was shown. 14
- NAC made its way into the American Association for the Study of Liver Disease Guidelines in 2011.3
- Several mechanistic studies in 2013 that showed plausible benefits whereby NAC reduces IL-17, bilirubin and ALT.13
- That same year; however, Squires et al. published a pediatric RCT that showed no benefit and arguably worse outcomes in children.11
- In 2017, the American Gastroenterology Association and the European Association for the Study of the Liver published opposing recommendations with the Americans making no recommendations about NAC and the Europeans recommending for the use of NAC.154
- In 2020, a Cochrane review by Siu et al. showed that despite rising use of NAC, the evidence was inconclusive and that both RCTs had high risk of bias.16
- NAC made its way into the American College of GI and the American GI association guidelines, again based on the potential for TFS in early coma grades.12315
- Most recently, in a 2024 Lancet Review by Maiwall et al, NAC has been described as the drug of choice for ALF.5
What do all these trials and guidelines amount to? Well essentially NAC is now widely recommended for non-APAP Acute Liver Failure despite a lack of high quality data. This is Largely due to favorable safety profile and lack of available alternatives, in a disease with mortality rates approaching 30%. It’s also relatively inexpensive with an approximate cost of 83$/day with our current dosing regimen.
NAC Dosing for non-APAP vs APAP ALF:
- When it comes to dosing, the regime used for non-APAP ALF in the Landmark RCT differs slightly from the current recommended Ontario Poison Control regimen:
- Dosing from the Landmark RCT by Lee et al. in 2009:14
- Initial loading dose of 150 mg/kg/h of NAC over 1 hour, followed by 12.5 mg/kg/h for 4 hours, then continuous infusions of 6.25 mg/kg NAC for the remaining 67 hours.
- Ontario Poison Control 1-Bag method for APAP toxicity:17
- Step 1: Loading dose of 150mg/kg over one hour
- Step 2: Maintenance dose of 15mg/kg/h for a minimum of 12h and until all Stopping Criteria are met
- Dosing from the Landmark RCT by Lee et al. in 2009:14
- Expert consensus is that you should use your center’s APAP NAC protocol to reduce likelihood of administration errors and for ease of use.
Etiology Specific Management
Acetaminophen Associated Toxicity17
We will not be covering the breadth of APAP toxicity but I would be remiss to not mention it as it is the number one cause of Acute Liver Failure in North America. Instead, we will be covering a few pitfalls in the management of APAP toxicity in the setting of ALF:
- Pitfall #1: Mis-applying the Rumack-Matthew nomogram to chronic overdoses, staggered overdoses, repeat supra-therapeutic ingestions and ingestions presenting outside of the 24h window. These patients may have APAP levels below the cutoff but carry risk of acute liver injury.
- All patients with elevated transaminases deemed to be due to an APAP ingestion should be started on NAC.
- Pitfall #2: Delaying NAC while awaiting an APAP level. NAC is maximally beneficial within 8 hours of ingestion, although there is still benefit in delayed ingestions.
- If you have reason to suspect a toxic APAP ingestion, NAC should be administered prior to a level returning.
- Pitfall #3: Beware of Massive ingestions, typically defined as being >500mg/kg. These patients present atypically, usually with coma and lactic acidosis prior to rise in transaminases.
- Discussion with Poison Control is particularly important for these patients some patients may benefit from dialysis and fomepizole, with potentially higher doses of NAC for dialysis as NAC can be dialyzed off.
Budd-Chiari Syndrome 7
- Another cause of Acute Liver Failure that we can promptly diagnose in the ED is Budd-Chiari Syndrome.
- As a reminder, Budd-Chiari Syndrome is a group of disorders that cause hepatic outflow tract obstruction. This is divided into primary budd-chiari syndrome, caused by hepatic vein thrombosis and secondary budd-chiari syndrome, caused by venous obstruction by malignant tumours.
- Risk factors for primary Budd-Chiari Syndrome include any part of Virchow’s triad.
- As we have discussed previously both Doppler U/S or CT can be used to diagnose this condition, although again, I would favour CT.
- Management should be performed in conjunction with Thrombosis and GI. First line treatment is with Low Molecular Weight Heparin.
Amatoxin Poisoning 18
- Amatoxin poisoning is a well-established cause of acute liver failure. The most common source of amatoxin comes from the Amanita genera, but the Galerina and Lepiota species have also been described as causing ALF. As most people gathering mushrooms will have thought that they were eating an edible species, a history of mushroom ingestion in the setting of ALF should be enough to proceed with treatment.
- The primary mechanism of toxicity of Amatoxin is via inhibition of RNA polymerase, leading to decreased protein synthesis and therefore hepatocellular necrosis. Amatoxin also has enterohepatic circulation, leading to repeated insults on the liver.
- A key feature of amatoxin toxicity is delayed onset GI symptoms, typically greater than 6h after ingestion. This distinguishes it from other forms of mushroom poisoning. This is followed by a latent period during which the patient may be asymptomatic but transaminases continue to rise. Acute Liver Failure typically develops after 48h and is characterized by all the biochemical and physiologic derangements we have previously discussed.
- Management:
- Call Poison Control
- Decontamination
- Often too late for Gastric Lavage due to delayed presentation
- Worth giving a dose of charcoal given the enterohepatic circulation
- Adjunct Therapies
- IV Penicillin G: Blocks Hepatic re-uptake of amatoxin
References
- Bernal W, Wendon J. Acute liver failure. N Engl J Med. 2013;369:2525–34.
- Stravitz RT, Lee WM. Acute liver failure. Lancet. 2019;394:869–81.
- Lee WM, Stravitz RT, Larson AM. AASLD Position Paper: Acute Liver Failure. Hepatology. 2012;55:965–7.
- European Association for the Study of the Liver. EASL Clinical Practical Guidelines. J Hepatol. 2017;66:1047–81.
- Maiwall R, Bajaj JS. Acute liver failure: current understanding. Lancet Gastroenterol Hepatol. 2024;9:123–40.
- Montrief T, Koyfman A, Long B. Acute liver failure: a review for emergency physicians. Am J Emerg Med. 2020;38:1915–24.
- O’Grady JG, Schalm SW, Williams R. Acute liver failure: redefining the syndromes. Lancet. 1993;342:273–5.
- Westbrook RH, Dusheiko G, Williamson C. Pregnancy and liver disease. J Hepatol. 2016;64:933–45.
- Tapper EB, Sengupta N, Bonder A. The 1000s club. Clin Gastroenterol Hepatol. 2023;21:e123–e132.
- Karvellas CJ, et al. Antimicrobial prophylaxis in ALF. Hepatology. 2016;63:1251–9.
- Squires RH et al. Pediatric NAC RCT. Hepatology. 2013;57:1542–9.
- American College of Gastroenterology. ACG Clinical Guideline: Acute Liver Failure. Am J Gastroenterol. 2023;118:1128–1153.
- Nabi T, Nabi S, Rafiq N. NAC in non‑APAP ALF. Saudi J Gastroenterol. 2013;19:199–203.
- Lee WM et al. NAC RCT. Gastroenterology. 2009;137:856–64.
- AGA Clinical Practice Update. Gastroenterology. 2017.
- Siu J et al. NAC for non‑APAP ALF. Cochrane Database Syst Rev. 2020.
- Ontario Poison Centre NAC protocol.
- Enjalbert F et al. Amatoxin poisoning. Toxicon. 2002;40:911–20.
