
When working up your patient, how often do you think of problems related to the hepatic venous system? Have you suppressed those memories of time spent over your cadaver in medical school learning the anatomy? By the end of this, you will all be newly discovered masters of anatomy and have a framework for how to diagnose and treat two rare but life-threatening conditions; splanchnic vein thrombosis and shock liver.
Splanchnic Vein Thrombosis
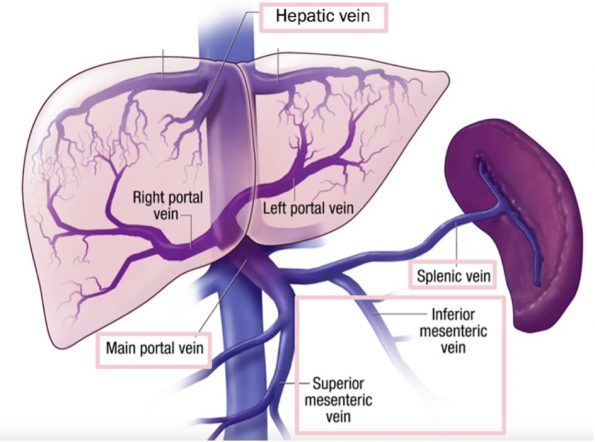
Quick Anatomy Review
There are 4 major veins of interest where clinically significant blood clots can form;
- Splenic
- Mesenteric (inferior and superior)
- Portal (most common), and
- Hepatic (most rare).
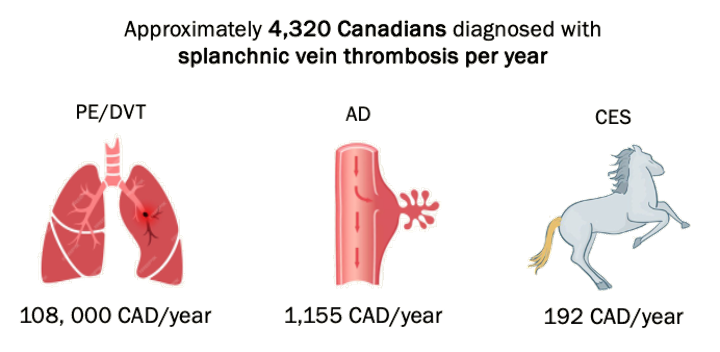
Why you should care about splanchnic vein thrombosis
As emergency medicine physicians we are masters at building differential diagnoses to rule out immediate life-threatening causes for our patient presentations. We are rapid to interrogate the possibility of cauda equina syndrome (CES) in our patients with back pain or to apply Well’s criteria for PE or DVT. We are much less likely however to think about splanchnic vein thrombosis in our abdominal pain patients. Compared to PE/DVT, splanchnic vein thrombosis is 22.5x more likely with 4320 cases diagnosed per year. Therefore we need to start including it in our differential diagnoses.
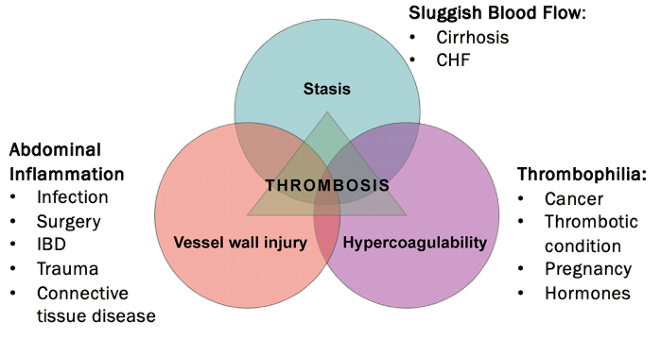
When should you consider it?
- Patients with abdominal pain
- One of Virchow’s triad:
- Stasis: CHF, Cirrhosis
- Endothelial/vessel wall injury: Infection, Surgery, Trauma, IBD, Connective tissue disease
- Hypercoagulability: Cancer, Thrombophilia
- Undifferentiated patient with significant liver enzyme elevation (Thousands Club) *** However caution with Liver enzymes as they may be normal since hepatic artery flow to the liver can compensate for decreased flow in these patients.
- Cancers especially intra-abdominal (most commonly we think of HCC due to it’s association with cirrhosis and proximity to splanchnic vessels) but any cancer causes hypercoagulability
- Most common thrombotic conditions we think about are Paroxysmal Nocturnal Hemoglobinuria and Myeloproliferative Neoplasms (i.e. Essential Thrombocytosis or Polycythemia Vera)
Diagnosis
For the most part the diagnosis is made on clinical suspicion and imaging findings, but there is some bloodwork that can be useful:
- Bloodwork:
- If resulting in bowel ischemia:
- ↑ WBC
- ↑ Hematocrit
- ↑ Lactate
- ↓ pH
- If underlying cirrhosis:
- ↑ Bili, INR, Cr
- ↓ Platelets
- N/↑ Liver enzymes
- This poses a unique challenge
- Liver perfused 2/3 by portal vein, 1/3 hepatic artery
- ↓ portal vein inflow due to splenic/mesenteric/portal clot is compensated for by normal hepatic arterial inflow
- Therefore, hepatic perfusion remains relatively normal therefore so do liver enzymes
- Most likely to see ↑ liver enzymes in Budd-Chiari
- Liver outflow tract completely blocked, no compensation
- Often quite pronounced, liver enzymes in 1000s
- Always keep Budd-Chiari on “Thousands Club Differential”:
- If resulting in bowel ischemia:
-
-
-
- Toxic Hepatitis (i.e Tylenol overdose)
- Viral Hepatitis (i.e. Hep A/B/C)
- Autoimmune Hepatitis
- Metabolic Disorders (i.e. Hemochromatosis, Wilson’s)
- HELLP Syndrome
- Budd-Chiari Syndrome
- Shock Liver
-
-
Although history helps identify patients in which this disease is more prevalent, it remains a radiologic diagnosis. When choosing between modalities you are faced with two options.
- Abdominal ultrasound with Doppler assessment of splanchnic vessels.
- CT abdo with contrast
Most international guidelines recommend ultrasound as a first-line modality. Assessment of the splanchnic vessels on ultrasound is not always guaranteed when you order a general abdominal or RUQ-focus ultrasound. If you suspect splanchnic vein thrombosis (which you should!) you need to ask for an assessment of the vasculature. CT scan is likely going to be more useful in the ED given we are entertaining a broader differential at the time of imaging. It will also provide you with other valuable information such as the extent of thrombosis, presence of bowel ischemia, and focus of infection (diverticulitis, cholecystitis, pancreatitis, etc.)
You have a CT report confirming splanchnic vein thrombosis, now what?
Your hunch was right or you’ve fallen into the 2% of abdominal CT scans that have the incidental finding of splanchnic vein thrombosis. Now what do you do with it?
Anticoagulation
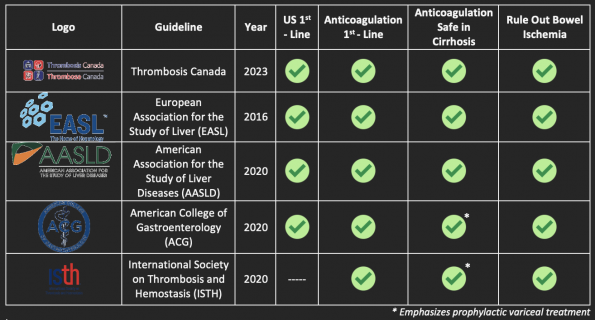
First-line therapy for this condition is anti-coagulation with low-molecular-weight heparin. Caution however before initiating therapy.
- If you remember from above, one of the common risk factors is cirrhosis. This condition has both procoagulant and anticoagulant effects. That being said, it is safe to treat cirrhotic patients with anticoagulants (Valeriani) as anticoagulation reduces the risk of worsening thrombosis and subsequent risk of variceal bleeding.
- This is a complex decision that should include your local Thrombosis expert. The treatment is not immediate and often will be a joint decision with gastroenterology.
- In patients with thrombocytopenia or irregular variceal screening, your local specialists may consider performing an endoscopy to band any varices if present before anticoagulation is initiated.
- Complicated paradox of risk of clotting and bleeding in cirrhosis has prompted further studies into whether there’s evidence for prophylactic anticoagulation against splanchnic vein thrombosis in cirrhotic
- Villa et al., 2021, randomized control trial:
- Prophylaxis with heparin in patients with cirrhosis reduced the risk of occurrence of portal vein thrombosis
- In turn, resulted in reduced risk of hepatic decompensation and mortality
- More data needed before widely implemented
- Currently not standard of practice in Canada and not supported by our GI or Thrombosis colleagues
- Ageno et al., 2022, prospective cohort study:
- DOACs are safe treatment alternative to warfarin for long-term management of splanchnic vein thrombosis
- TOH Thrombosis cautions against discharging asymptomatic patients or patients whose pain you’ve controlled in the ED with outpatient Thrombosis follow up on a DOAC
- Reasons are multifactorial:
- DOACs are not initial management
- Heparin is preferred to see how patients evolve, whether they will need surgery/scopes
- Often require multi-disciplinary approach
- Discussions between GI and Thrombosis, best done as an inpatient
- Risk of complications such as bowel ischemia
- Can occur despite treatment
- Require period of monitoring
- DOACs are not initial management
- Reasons are multifactorial:
- Prophylaxis with heparin in patients with cirrhosis reduced the risk of occurrence of portal vein thrombosis
- Anticoagulation does have specific benefits:
- Prevents clot propagation
- Restores venous patency
- Decompresses congested bowel and/or liver
- Coagulopathy and Clotting in Cirrhosis:
- Cirrhosis is one of the biggest risk factors for the development of splanchnic vein thrombosis
- Cirrhosis impacts both procoagulant and anti-coagulant factors
- Serves as an independent risk factor for both clotting and bleeding
- Considering this fine balance, studies have looked into the safety of anticoagulation for splanchnic vein thrombosis in cirrhotic patients
- Valeriani et al., 2021, systemic review and meta-analysis:
- In cirrhotic and non-cirrhotic patients, anticoagulation improves the rate of vein recanalization, reduces risk of thrombus progression and paradoxically actually decreases overall rates of major bleeding (especially in cirrhotics)
- Treating splanchnic vein thrombosis prevents worsening of portal hypertension
- Patients less at risk of variceal bleeding in the future
- International guidelines support that anticoagulation is safe in cirrhosis and in patients with complications from portal hypertension
- Treating splanchnic vein thrombosis prevents worsening of portal hypertension
- In cirrhotic and non-cirrhotic patients, anticoagulation improves the rate of vein recanalization, reduces risk of thrombus progression and paradoxically actually decreases overall rates of major bleeding (especially in cirrhotics)
Hunt for ischemia
You also need to be on the lookout for patients who may be suffering from bowel ischemia. This is most often a complication associated with mesenteric vein thrombosis as these veins directly drain the bowel. However, it can be a complication with any splanchnic vein thrombosis. Be on the lookout for:
-
- Persistence of severe abdominal pain
- Peritonitis or pain out of proportion (spectrum of presentation)
- Rectal bleeding
- Fever
- Ascites
- MOD
- ↑ WBC, ↑ lactate, ↓ pH
- More at risk for bowel ischemia when clot is larger and more occlusive
- Early treatment of thrombi with anticoagulation is our best defense against the development of bowel ischemia
In these patients, on top of involving thrombosis, you want to urgently consult general surgery.
Disposition
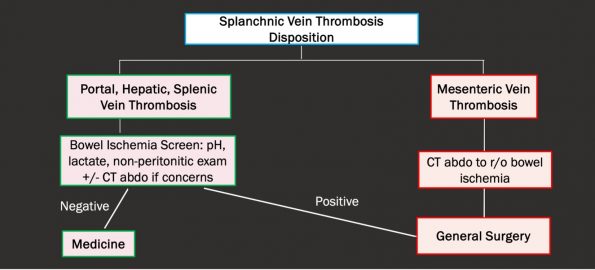
- First, discuss the case with thrombosis
- Decisions will be made on a case-by-case basis but rarely will a patient be sent home with outpatient thrombosis F/U
- For a portal, hepatic or splenic vein thrombus, as long as you’ve done your due diligence to consider bowel ischemia (screening bloodwork, clinical exam, CT abdo only absolutely necessary if concerns) and this screen is negative, these patients can be admitted to medicine
- Different approaches are required for mesenteric vein thrombosis given their higher risk of bowel ischemia
- If not already diagnosed on CT, patients with mesenteric vein thrombosis should undergo a CT abdo to r/o bowel ischemia
- Regardless of whether there’s bowel ischemia or not, a Gen Sx consult in the ED is very reasonable given their predisposition to developing bowel ischemia
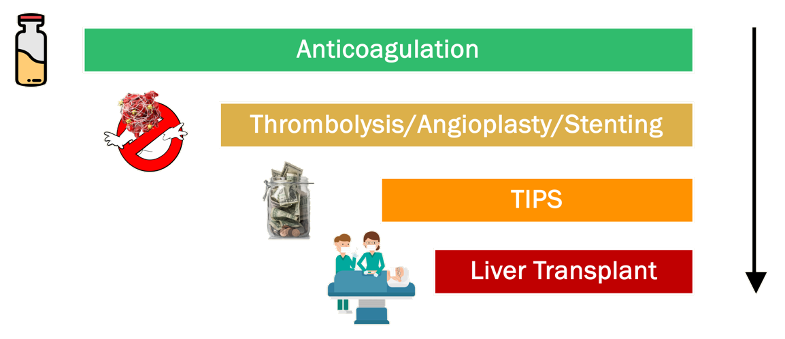
- Here is the management escalation recommendation based on guidelines in the treatment of splanchnic vein thrombi
- Anticoagulation is always first line
- If anticoagulation is unsuccessful, patients may be considered for thrombolysis or balloon angioplasty or stenting
- Most commonly you’ll see thrombolysis done, performed at TOH by IR
- If thrombolysis not working or is not possible, then we would escalate to a TIPS procedure (Transjugular intrahepatic portosystemic shunt) which involves forming a connection between the portal vein to the hepatic vein to decompress the liver
- This procedure is also done by IR at most centers, including TOH
- Sometimes these patients still progress and will need to go to Toronto for a liver transplant
- Hepatic vein thrombus is when you’re more likely to see patients progressing through this algorithm and are at the highest rates of needing management escalation above anticoagulation
- For us in the ED, really the only management decision we are making is to anticoagulate or not and we often have thrombosis to help us with this decision
- We need to recognize when anticoagulation alone may not work and to involve other consultants as early as needed and counsel our patients on what to expect
Summary by major organizations
Ischemic Hepatitis – “Shock Liver”
What is it?
This clinical condition results from hepatocellular injury as a result of decreased forward perfusion to the liver. This can be secondary to low flow states from injury to vascular supply, congested vasculature, or, relevant to this post, decreased perfusion secondary to a thrombus.
Since the liver has high metabolic activity blood flow is critical to function. At any point, approximately 25% of your cardiac output is directed to the liver. Therefore, any small disturbance in supply can lead to injury. Despite the liver’s vulnerability to injury, it is often sacrificed during periods of systemic stress. Our sympathetic nervous system shunts blood flow away from our abdominal organs during acute stressors in order to provide increased perfusion to the brain, heart and lungs.
As a result, many of our acutely ill patients will have some element of ischemic hepatitis. It is estimated that 2-10% of ICU patients will present for admission/later develop this condition.
Ischemic Hepatitis ≠ Acute Liver Failure
It is important to make the distinction that ischemic hepatitis is different from acute liver failure. As such, presentation and investigations will be different and holds important management differences.
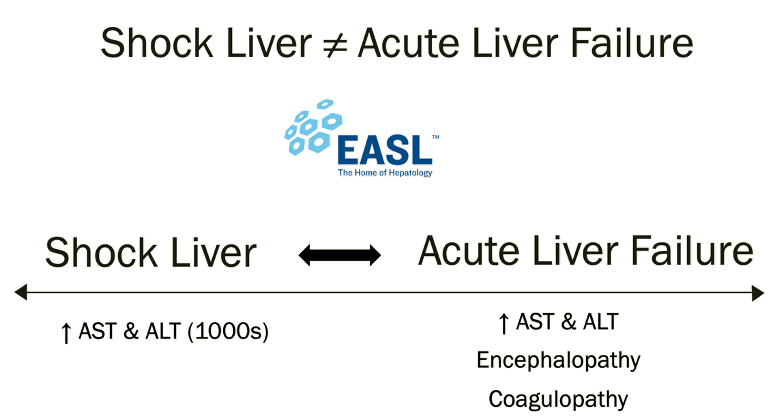
- Shock liver is NOT the same as acute liver failure
- These two clinical entities exist on a spectrum
- The EASL guidelines describe shock liver as simply elevated transaminases
- AST & ALT in the 1000’s
- If this shock liver state progresses to encephalopathy, coagulopathy, therefore once there is true liver dysfunction, we call this Acute Liver Failure
- In reality, as I’m sure many of you have seen, it’s not black and white, many of these pts are intubated so clinically assessing encephalopathy can be a challenge and serum ammonia level is not always helpful
- Coagulopathy is roughly when INR>1.5 but many of our critically ill patients are anticoagulated, have liver dysfunction at baseline
- Therefore you may frequently hear patients in the ICU referred to as having shock liver and when you look at their coags they are elevated – in this case it’s assumed that their liver function itself is normal and the elevated coags are due to other causes and not acute failure
- Acute liver failure is the end point that many types of liver insults can lead to, ischemic hepatitis is only one of those causes
Management
- No specific treatment for shock liver
- Usually self-limited in the absence of ongoing liver perfusion disturbance
- Goals are to treat underlying causes of hemodynamic instability (i.e. infection, hemorrhage ionotropes for cardiogenic cause) and restore cardiac output and ensure adequate perfusion
- For this, Norepi is very often your first-line pressor in these patients as they often have distributive/vasoplegic shock
- Also want to avoid aggressive diuresis
- No specific treatment for reducing reperfusion injury to the liver
- Mortality rate 25%
- Higher if concomitant cirrhosis
- More likely to develop acute liver failure
- Evidence for NAC in Shock Liver?
- NAC is a potent antioxidant
- Several RCTs support use of NAC in non-acetaminophen related acute liver failure
- Theory that NAC may help prevention of acute liver failure in patients with shock liver
- Limited evidence for this (mainly case reports)
- Expert, Dr. Ariel Hendin, ICU Staff:
- Recommends use of NAC for acute liver failure, regardless of the cause as there’s evidence that it improves mortality
- Currently not enough evidence for use of NAC in preventing the development of ischemic hepatitis in high-risk patients or in preventing ischemic hepatitis from developing into acute liver failure
- Agrees it’s practically not our role in ED to be giving NAC to any patients outside tylenol overdose, this can be left to our ICU colleagues
- NAC is a potent antioxidant
- Higher if concomitant cirrhosis
We have identified that states of unstable hemodynamics will precipitate this condition. Therefore, our goal directed therapy is to address their hemodynamics and underlying pathology causing it wether it is sepsis, cardiogenic shock or other. Quick plug also for using PoCUS to determine cause of undifferentiated shock.
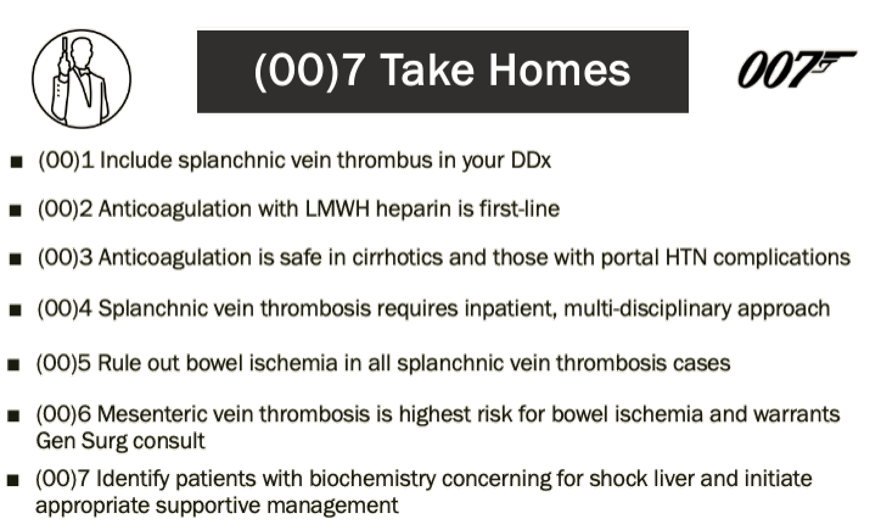
TL:DR
We’ve summarized the pertinent information in splanchnic vein thrombosis and ischemic hepatitis and you are now ready to take this information with you to your next shift.
References
Ageno W, Beyer Westendorf J, Contino L, Bucherini E, Sartori MT, Senzolo M, Grandone E, Santoro R, Carrier M, Delluc A, De Stefano V, Pomero F, Donadini MP, Tosetto A, Becattini C, Martinelli I, Nardo B, Bertoletti L, Di Nisio M, Lazo-Langner A, Schenone A, Riva N. Rivaroxaban for the treatment of noncirrhotic splanchnic vein thrombosis: an interventional prospective cohort study. Blood Adv. 2022 Jun 28;6(12):3569-3578.
Ageno W, Squizzato A, Togna A, Magistrali F, Mangini M, Fugazzola C, Dentali F. Incidental diagnosis of a deep vein thrombosis in consecutive patients undergoing a computed tomography scan of the abdomen: a retrospective cohort study. J Thromb Haemost. 2012 Jan;10(1):158-60.
Candeloro M, Valeriani E, Monreal M, Ageno W, Riva N, Schulman S, Bang SM, Mellado M, Díaz-Peromingo JA, Moisés J, Díaz-Brasero AM, Garcia-Pagan JC, Perez-Campuzano V, Senzolo M, De Gottardi A, Di Nisio M. Clinical course and treatment of incidentally detected splanchnic vein thrombosis: an individual patient data meta-analysis. J Thromb Haemost. 2023 Jun;21(6):1592-1600.
Cherukuri R, Haskal ZJ, Naji A, Shaked A. Percutaneous thrombolysis and stent placement for the treatment of portal vein thrombosis after liver transplantation: long-term follow-up. Transplantation. 1998 Apr 27;65(8):1124-6.
Ciobanu AO, Gherasim L. Ischemic Hepatitis – Intercorrelated Pathology. Maedica (Bucur). 2018 Mar;13(1):5-11. PMID: 29868133; PMCID: PMC5972787.
Delgado MG, Seijo S, Yepes I, Achécar L, Catalina MV, García-Criado A, Abraldes JG, de la Peña J, Bañares R, Albillos A, Bosch J, García-Pagán JC. Efficacy and safety of anticoagulation on patients with cirrhosis and portal vein thrombosis. Clin Gastroenterol Hepatol. 2012 Jul;10(7):776-83.
Dong S, Qi H, Li Y, Men P, Alifu M, Zhang Y, Li Y, Zhao R. A systematic review and meta-analysis of anticoagulation therapy for portal vein thrombosis in patients with cirrhosis: to treat or not to treat? Hepatol Int. 2021 Dec;15(6):1356-1375.
Eisenhut M. Ischemic hepatitis and collateral damage to the liver in severe viral respiratory tract infections. Am J Pathol. 2006 Sep;169(3):1100; author reply 1100.
Fuhrmann V, Jäger B, Zubkova A, Drolz A. Hypoxic hepatitis – epidemiology, pathophysiology and clinical management. Wien Klin Wochenschr. 2010 Mar;122(5-6):129-39.
Guerrero A, Campo LD, Piscaglia F, Scheiner B, Han G, Violi F, Ferreira CN, Téllez L, Reiberger T, Basili S, Zamora J, Albillos A; Baveno Cooperation: an EASL consortium. Anticoagulation improves survival in patients with cirrhosis and portal vein thrombosis: The IMPORTAL competing-risk meta-analysis. J Hepatol. 2023 Jul;79(1):69-78
Hanafy AS, Abd-Elsalam S, Dawoud MM. Randomized controlled trial of rivaroxaban versus warfarin in the management of acute non-neoplastic portal vein thrombosis. Vascul Pharmacol. 2019 Feb;113:86-91. Epub 2018 Jun 7.
Henrion J. Hypoxic hepatitis. Liver Int. 2012 Aug;32(7):1039-52.
Lightsey JM, Rockey DC. Current concepts in ischemic hepatitis. Curr Opin Gastroenterol. 2017 May;33(3):158-163.
Loffredo L, Pastori D, Farcomeni A, Violi F. Effects of Anticoagulants in Patients With Cirrhosis and Portal Vein Thrombosis: A Systematic Review and Meta-analysis. Gastroenterology. 2017 Aug;153(2):480-487.e1. doi: 10.1053/j.gastro.2017.04.042. Epub 2017 May 4.
Mohamed MF, Wadhavkar N, Elfanagely Y, Marino D, Beran A, Abdallah M, Promrat K. Etiologies and Outcomes of Transaminase Elevation > 1000 IU/L: A Systematic Review and Meta-Analysis. Dig Dis Sci. 2023 Jul;68(7):2843-2852.
Naymagon L, Tremblay D, Zubizarreta N, Moshier E, Troy K, Schiano T, Mascarenhas J. The efficacy and safety of direct oral anticoagulants in noncirrhotic portal vein thrombosis. Blood Adv. 2020 Feb 25;4(4):655-666. doi: 10.1182/bloodadvances.2019001310. PMID: 32078681; PMCID: PMC7042983.
Seeto RK, Fenn B, Rockey DC. Ischemic hepatitis: clinical presentation and pathogenesis. Am J Med. 2000 Aug 1;109(2):109-13.
Sogaard KK, Astrup LB, Vilstrup H, Gronbaek H. Portal vein thrombosis; risk factors, clinical presentation and treatment. BMC Gastroenterol. 2007 Aug 15;7:34.
Tapper EB, Sengupta N, Bonder A. The Incidence and Outcomes of Ischemic Hepatitis: A Systematic Review with Meta-analysis. Am J Med. 2015 Dec;128(12):1314-21.
Valeriani E, Riva N, Di Nisio M, Ageno W. Splanchnic Vein Thrombosis: Current Perspectives. Vasc Health Risk Manag. 2019 Oct 22;15:449-461.
Valeriani E, Di Nisio M, Riva N, Cohen O, Garcia-Pagan JC, Magaz M, Porreca E, Ageno W. Anticoagulant therapy for splanchnic vein thrombosis: a systematic review and meta-analysis. Blood. 2021 Mar 4;137(9):1233-1240.
Villa E, Cammà C, Marietta M, Luongo M, Critelli R, Colopi S, Tata C, Zecchini R, Gitto S, Petta S, Lei B, Bernabucci V, Vukotic R, De Maria N, Schepis F, Karampatou A, Caporali C, Simoni L, Del Buono M,
Waseem N, Chen PH. Hypoxic Hepatitis: A Review and Clinical Update. J Clin Transl Hepatol. 2016 Sep 28;4(3):263-268.
Yang XL, Cheng TO, Chen CR. Successful treatment by percutaneous balloon angioplasty of Budd-Chiari syndrome caused by membranous obstruction of inferior vena cava: 8-year follow-up study. J Am Coll Cardiol. 1996 Dec;28(7):1720-4.
Zambotto B, Turola E, Fornaciari G, Schianchi S, Ferrari A, Valla D. Enoxaparin prevents portal vein thrombosis and liver decompensation in patients with advanced cirrhosis. Gastroenterology. 2012 Nov;143(5):1253-1260.e4.
Guidelines:
AASLD Guidelines:https://journals.lww.com/hep/fulltext/2021/01000/vascular_liver_disorders,_portal_vein_thrombosis,.26.aspx
ACG Guidelines:https://journals.lww.com/ajg/fulltext/2020/01000/acg_clinical_guideline__disorders_of_the_hepatic.9.aspx
European Association for the Study of the Liver: EASL Clinical Practice Guidelines: Vascular diseases of the liver. J Hepatol. 2016 Jan;64(1):179-202.
European Association for the Study of the Liver. Clinical practice guidelines panel; Wendon, J; Panel members; Cordoba J, Dhawan A, Larsen FS, Manns M, Samuel D, Simpson KJ, Yaron I; EASL Governing Board representative; Bernardi M. EASL Clinical Practical Guidelines on the management of acute (fulminant) liver failure. J Hepatol. 2017 May;66(5):1047-1081.
International Society of Thrombosis and Hematology: Di Nisio M, Valeriani E, Riva N, Schulman S, Beyer-Westendorf J, Ageno W. Anticoagulant therapy for splanchnic vein thrombosis: ISTH SSC Subcommittee Control of Anticoagulation. J Thromb Haemost. 2020 Jul;18(7):1562-1568.
Kwo PY, Cohen SM, Lim JK. ACG Clinical Guideline: Evaluation of Abnormal Liver Chemistries. Am J Gastroenterol. 2017 Jan;112(1):18-35.
Thrombosis Canada: https://thrombosiscanada.ca/wp-uploads/uploads/2021/11/44.-Portal-Vein-Thrombosis_14November2021.pdf
