
“It feels like they’re just mostly just trying to make me comfortable with being uncomfortable”
My now-husband was always a year ahead of me in training. He was a first-year medical student before I was, a clerk before I was, and every year I would ask him the same question: “So… what’s this year like?” One answer has stayed with me ever since.
“It feels like they’re mostly just trying to make me comfortable with being uncomfortable.”
At the time, it felt like a simple observation. Looking back, it may have been one of the most important lessons of medical training.
That idea became something of a coping mechanism throughout my own journey. Whenever I found myself feeling overwhelmed, uncertain, or out of my depth, I reminded myself that discomfort wasn’t necessarily a sign that something was wrong. It was often the point. Medical training is, in many ways, an exercise in repeatedly placing yourself in situations that are inherently uncomfortable until they become familiar enough that you can function effectively within them.
Medicine demands this of us. We work long hours with little sleep. We have difficult conversations with patients and families. We screen adolescents for eating disorders, tell parents that their child is critically ill, and sit with families after the death of a loved one. None of these experiences should ever become easy, nor should they. But with repetition, supervision, and increasing autonomy, we develop the confidence and emotional capacity to navigate them. The situations remain difficult, but we become better equipped to meet them.
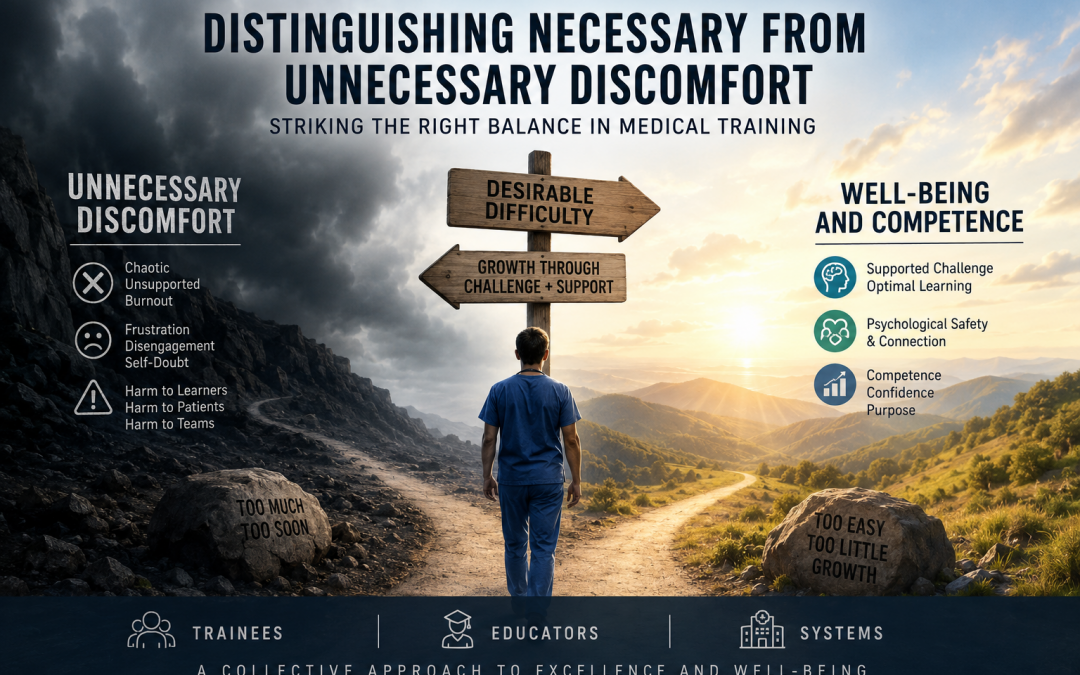
This raises an important question. Which discomforts are truly necessary to develop competent, resilient physicians, and which are simply artifacts of a training system that has been slow to evolve? Put another way, which challenges help trainees grow, and which unnecessarily erode their well-being, strain their personal lives, and threaten career longevity without making them better doctors?
As I was researching this topic, I found myself thinking back to one of the internet’s most famous debates: the 2018 “Yanny versus Laurel” audio clip. It captivated millions because it was remarkable that two people could listen to the exact same recording and come away convinced they had heard entirely different words. It was entertaining at the time, but in hindsight I think it also serves as a useful metaphor. Sometimes two people can be presented with the same experience, the same evidence, or the same facts, yet arrive at completely different conclusions about what they mean.
Medical training is no different. Consider, for example, the experience of two trainees…
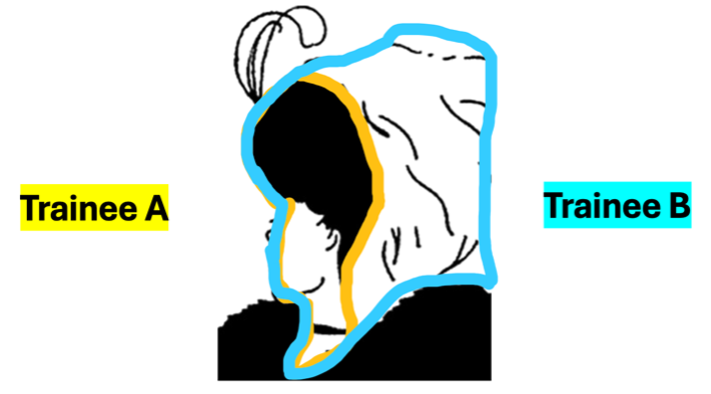
- Trainee A, was told by peers during their internal medicine rotation that “by leaning into tasks perceived as scut work such as calling pharmacies, obtaining outside records, calling a patient’s specialist or primary care doctor” he was “failing to set boundaries and reinforcing problematic norms”
- While the trainee found these experiences contributed to his learning and assisted with patient care, he found it difficult to challenge his peers’ perceptions, stating that “if you disagree with someone who’s trying to set such boundaries, you’re seen as part of a toxic culture and not supporting people in their wellness
- Now let’s contrast this experience with that of Trainee B:
- While in the OR, a surgery staff, recognizing that the case was running long and the trainee in the room likely hadn’t eaten, encouraged the trainee to take the staff’s credit card and buy themselves something to eat
- That staff later received a professionalism complaint that the trainee felt they were “forced to leave the OR, causing them to miss out on a learning opportunity” and “belittled to the point that it was assumed they couldn’t pay for their own lunch”
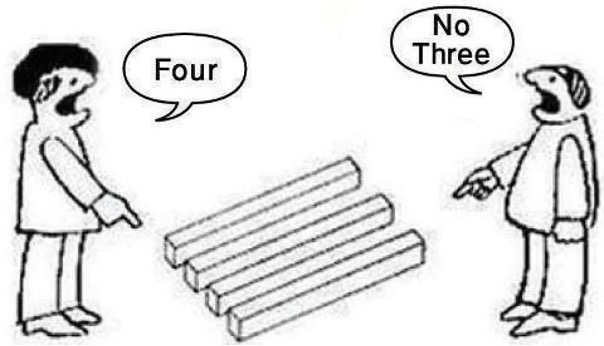
- These cases emphasize how two people can interpret the same thing very differently
- In the first case, we have a trainee trying to do their best for the patient but being called out by their peers for contributing to toxic workplace culture
- In the second, we have a trainee trying to learn and be independent, but misinterpreting a gesture of good will
- Both of these cases can be seen from multiple perspectives
- One perspective is that the trainee is experiencing a valuable learning opportunity and the other is that a learning opportunity is detracting from their wellness

- There are clear evolving tensions between educators and trainees when it comes to the pursuit of competence versus ensuring trainees’ wellness
- Many trainees are advocating for an increased focus on their well-being while many educators feel that this younger generation of trainees are “staying too comfortable”
- In other words, not staying late, not volunteering to take on extra work to help the team, not prepping for their clinics or cases the night before; essentially, they’re not seeking learning opportunities to maximize their competence
- Before we seek to try and navigate these tensions, it’s important that we take a look at what’s led to their development
A Job, or a Calling?

- One place these tensions have become particularly visible in recent years is in the recurring social media debate over whether medicine is a job or a calling.
- On the surface, many dismiss this debate as uninteresting. There is likely no objectively correct answer, and the relationship each physician has with their work is deeply personal.
- Yet the discussion has revealed a noticeable generational shift, with many younger physicians expressing discomfort, or even outright rejection, of the idea that medicine should be considered a calling.
- Lisa Rosenbaum, a cardiologist at Harvard and National Correspondent for the New England Journal of Medicine, has explored this question extensively.
-
- Through her Not Otherwise Specified podcast, she has interviewed hundreds of trainees and educators, examining how the evolving identity of medicine is shaping professional fulfillment, expectations, and the culture of medical training.
-
“False sanctity in the term ‘calling’ tricks trainees into thinking that work is the most important aspect of their lives. Not only does this diminish many other meaningful aspects of life, but work can be a precarious source of identity”
“Claiming it’s a ‘calling’ as a trainee can be weaponized by taking a group of people that have the least power in a dynamic and also the most standing in the game; because trainees are not established, they don’t have a reputation, they don’t have a career long CV to fall back on, they’re just getting started at this point”
– Rosenbaum, NEJM Podcast: Not Otherwise Specified, 2024
Act 1: Rejection of Medicine as a Calling – Trainee Disillusionment
- So what’s let to this rejection of medicine as a calling by more and more trainees in recent years?
- What factors have contributed to this sense of trainee disillusionment?
Covid-19 Pandemic:
- Of course, the COVID-19 pandemic fundamentally altered the training experience. Many trainees described feeling like “just another warm body”, filling shifts when colleagues became ill, often before the risks of COVID-19 were fully understood.
- They also lost much of the sense of community that has traditionally defined residency. Social distancing meant that friendships and support networks were often confined to the hospital, with few opportunities to connect outside of work.
- As one program director reflected: “Although medical training always meant delayed financial gratification, the pandemic amplified the perceived unfairness: if you were barely making rent, saddled with debt, and scrolling through Instagram pictures of friends’ exotic ‘working from home’ destinations while fielding requests to cover shifts for co-residents out with COVID, why wouldn’t you have questioned the fairness of your working conditions?”
- Although the acute phase of the pandemic has passed, many educators feel that this sense of disillusionment has persisted.
- Those who weathered COVID as senior residents or early staff physicians often encourage a more transactional relationship with medicine among today’s trainees, not out of cynicism, but as a way of protecting them from the sacrifices they themselves experienced.
- The sentiment can sound something like: “I want to treat medicine like a job, so I need you to treat it like a job too, because it helps validate my own decision to do the same.”
- Or, put another way: “If I encourage you to leave when your shift is over, it makes it easier for me to leave when mine is over.”
- Those who weathered COVID as senior residents or early staff physicians often encourage a more transactional relationship with medicine among today’s trainees, not out of cynicism, but as a way of protecting them from the sacrifices they themselves experienced.

“Anti-Workism” Movement
- This shift in thinking did not begin with the pandemic. In a widely read 2019 article for The Atlantic, Derek Thompson described the rise of workism, the belief that work should sit at the center of one’s identity, serving not just as a source of income, but of meaning, purpose, and self-worth. He argued that many people had begun rejecting this idea, viewing work less as a calling and more as one component of a well-rounded life.
- As medical trainees watched these conversations unfold across social media and in popular culture, many naturally began to question whether medicine should occupy such a central place in their own identities.
- Yet the pushback against workism is hardly new.
- Thompson points to John Maynard Keynes’ 1930 essay, Economic Possibilities for our Grandchildren, in which Keynes predicted that technological progress would reduce the workweek to roughly 15 hours, leaving future generations with the equivalent of a five-day weekend.
- Even into the 1960s, commentators anticipated that increasing automation and shorter workweeks would lead people to seek meaning not through their careers, but through leisure, relationships, and personal pursuits.
- Those predictions, of course, never materialized. Productivity increased, but so too did expectations of work. Yet the underlying skepticism toward work as the defining feature of one’s identity has endured.
- Many millennials were encouraged by their Baby Boomer parents to “follow their passion,” only to graduate into unstable job markets carrying substantial educational debt. Instead of finding purpose through meaningful work, many found themselves in jobs that were exhausting, insecure, or disconnected from the ideals they had been promised.
- For many, this led to an uncomfortable realization: work does not necessarily love you back.
- It is therefore not surprising that anti-workism gained traction. It is difficult to remain devoted to a “religion” that appears indifferent to your sacrifices.
- Increasingly, many medical trainees are asking the same question. If medicine does not make them feel valued, included, or supported, why should it define who they are?

Moral Injury
- Another major force driving trainee disillusionment is the growing sense that they are simply unable to care for patients in the way they believe they should. Increasingly, it is not a lack of knowledge or effort that limits good care, but systemic barriers that feel impossible to overcome.
- One way of coping with this reality is to emotionally distance oneself from work by viewing medicine as “just a job.”
- The internal dialogue becomes something like: “I can’t afford to become emotionally invested in every patient, because if I do, it hurts too much when the system prevents me from helping them the way I know they deserve.”
- One way of coping with this reality is to emotionally distance oneself from work by viewing medicine as “just a job.”
- In 2018, Wendy Dean and Simon Talbot introduced the concept of moral injury into the medical literature. Originally used to describe the psychological wounds experienced by soldiers forced to act against their deeply held moral beliefs, the term was adapted to describe what physicians experience when healthcare systems repeatedly prevent them from delivering the care they know their patients need.
- For many clinicians, this concept finally gave language to an experience they had long struggled to articulate. It shifted the conversation away from burnout, a term that often implies an individual deficiency and invites solutions focused on personal resilience: practice more mindfulness, take more vacations, improve your work-life balance. Moral injury, in contrast, recognizes that many physicians are responding normally to abnormal systems.
- Yet even physicians who attempt to address these systemic problems through advocacy can feel unsupported by the institutions they serve.
- Many will remember the case of Kaitlin Stockton, an emergency physician in British Columbia who posted a sign in her emergency department warning patients about prolonged wait times and resource shortages in an effort to be transparent. Rather than being commended for her honesty, she faced threats to her employment and professional standing for speaking publicly about unsafe conditions.
- Stories like these reinforce the perception that physicians are expected to absorb the consequences of a strained healthcare system while remaining silent about its failures.
- Taken together, the pandemic, the broader societal rejection of workism, and the rise of moral injury in response to worsening system pressures help explain why many trainees have become skeptical of the idea that medicine is anything more than a job.
- If medicine is viewed primarily as a job, it naturally follows that there are limits to the discomfort and sacrifice one is willing to tolerate. Protecting one’s own well-being becomes not only understandable, but rational.
- Increasingly, there is a belief that describing medicine as a calling implies a degree of moral nobility that the healthcare system has failed to earn.
- The sacrifices that may once have provided physicians with a profound sense of purpose or vocation are, for many, being replaced by the feeling that they are simply another cog in an overburdened machine.
… but is it the chicken, or the egg?

- As this shift has accelerated, some educators have become concerned that the pendulum has swung too far. They worry that viewing medicine exclusively as a job, with no sense of vocation or professional calling, risks sacrificing competence and professional growth in the name of wellness.
- For years, these tensions have existed beneath the surface, discussed quietly in hallways and call rooms but rarely examined openly.
- Yet we cannot meaningfully improve medical training, or fulfill our professional responsibility to patients, without first acknowledging that both perspectives arise from legitimate concerns. Only by understanding why trainees have become disillusioned, and why educators worry about the consequences, can we begin to distinguish the discomforts that are necessary for growth from those that are simply unnecessary burdens.
ACT 2: Tough Love – the Educator’s Perspective
“It’s become almost ‘cool’ to view being a doctor or medical training — and the demands that come with it — as a huge slight and unfair”
“But when every ill feeling is labeled as ‘trauma’, distinguishing among harms of varying magnitudes becomes difficult, as does targeting interventions to root problems”
– Rosenbaum, NEJM Podcast: Not Otherwise Specified, 2024
Trauma as a New Form of Social Capital: “Trauma Creep”
- Some educators have observed a shift in what earns social capital among trainees. Rather than being recognized primarily for qualities such as diligence, resilience, or clinical excellence, there is a growing perception that status is increasingly gained through publicly challenging the norms and conditions of medical training.
- This raises an important question: in trying to correct genuine problems within medical education, are we at times losing sight of the forest for the trees?
- To be clear, this is not because educators oppose trainee wellness. Quite the opposite. Most educators are deeply invested in both developing highly competent physicians and ensuring that trainees remain healthy enough to enjoy long, sustainable careers.
- Where some educators perceive tension is in what has been termed trauma creep. Australian psychologist Nick Haslam has described this phenomenon as the progressive expansion of concepts such as trauma and harm, whereby increasingly less severe experiences come to be interpreted through the same lens as genuinely traumatic events.
- The concern is not that trainees experience distress, many unquestionably do, but that if every uncomfortable experience is framed as harmful or morally injurious, we risk losing the ability to distinguish between the discomfort that is essential for learning and the discomfort that reflects a training system in need of reform.
“Experiencing daily racism, for instance, is different from being asked by your patients if you’re old enough to be a doctor. Having to admit a new patient right before end of shift is not a moral injury, and burnout is not the same as depression.
The substantial proportion of trainees who have debilitating mental illness need adequate care, but we cannot help them — much less address our structural inadequacies — if differentiating between serious illness and the inevitable challenges of training is treated as a moral breach.”
– Rosenbaum, Being Well While Doing Well, NEJM, 2024
- Educators such as Lisa Rosenbaum have posed an important question: in our efforts to minimize trainee discomfort, have we inadvertently compromised the development of the skills required to care for others who are suffering?
- As trainee well-being has rightly become a greater priority, and as concepts such as trauma have expanded, many educators describe an increasing challenge in balancing psychological safety with their responsibility to provide honest, constructive feedback and uphold standards of competence.
- Many also acknowledge that the stakes of giving difficult feedback feel higher than they once did. They worry about being perceived as outdated or insensitive, being accused of learner mistreatment, facing professional repercussions, or simply being viewed as someone who does not care about trainee well-being.
- The result, some argue, is a quieter educational environment, where difficult conversations are avoided, standards become harder to enforce consistently, and opportunities for meaningful growth may be lost.

- To be clear, few would argue for a return to the era of retaliatory teaching, public humiliation, or shaming trainees. Medical education has rightly moved away from these harmful practices.
- Yet many educators worry that, in correcting those excesses, we may be drifting toward the opposite end of the spectrum.
- Some have described this as the “dove phenomenon”: an educational culture that increasingly prioritizes emotional safety over challenge, avoids conflict, hesitates to deliver critical feedback, fears professionalism complaints, and develops a progressively lower tolerance for learner discomfort.
- The concern is not that trainees should suffer unnecessarily, but that growth often requires experiences that are uncomfortable without being harmful. If all discomfort is viewed as something to eliminate, some of the very experiences that foster resilience, clinical judgment, and professional identity may also disappear.
- This distinction extends well beyond medicine. In a conversation with journalist Ezra Klein, adolescent psychologist Lisa Damour observed that our culture has increasingly come to equate being mentally healthy with feeling good, calm, or relaxed. Yet emotional well-being does not mean the absence of difficult emotions. In many circumstances, anxiety, discomfort, grief, and uncertainty are normal and appropriate responses to challenging situations.

- Learning anything, whether it is playing the piano, mastering a new language, or becoming a physician, is inherently uncomfortable. Struggle is not evidence that learning has failed; it is often evidence that learning is taking place. Yet increasingly, this necessary discomfort is at times conflated with threats to wellness.
- As I reflected on these tensions, I found myself drawing an unexpected parallel. Perhaps it is because I am about to become a first-time parent and am already acutely aware of how much I have to learn, but the relationship between trainees and educators increasingly reminds me of that between teenagers and their parents – I suspect most of us can sympathize, at least to some degree, with the parent of a teenager.
- A parent’s goal is not simply to keep their teenager happy. It is to help them become a capable, independent adult. Those two goals often align, but sometimes they are in conflict.
- From the parent’s perspective, giving their teenager responsibility, setting boundaries, allowing them to experience failure, and trusting them to navigate uncomfortable situations are all acts of preparation. They are attempts to build the judgment and resilience needed to navigate an unpredictable world.
- Yet the teenager may experience those very same actions quite differently: as controlling, dismissive, unsupportive, or disconnected from what they believe they need in the moment.
- Neither perspective is entirely wrong. They are simply rooted in different time horizons. One is focused on immediate well-being; the other is focused on long-term growth. Perhaps the relationship between trainees and educators is more similar than either side would like to admit.
- To be clear, I am not suggesting that trainees are children. Rather, I think there are important parallels in the relationships themselves.
- Like parents, educators are deeply invested in who their trainees ultimately become. Their responsibility extends beyond ensuring that learners are happy today; it is to prepare them to become thoughtful, capable, and compassionate physicians tomorrow.
- This places educators in a difficult position. On one hand, they want to foster psychological safety, support trainee well-being, and avoid unnecessary hardship. On the other, they have a professional obligation to challenge learners, provide honest feedback, and create experiences that develop the competence required for independent practice. Balancing those goals is rarely straightforward.
- As we’ve already discussed, medicine is inherently uncomfortable. It involves physical fatigue, uncertainty, impossible decisions, emotionally charged conversations, and caring for people who are frightened, vulnerable, and sometimes direct that fear toward those trying to help them.
- The challenge, then, is not how to eliminate discomfort, but how to distinguish between the discomfort that is intrinsic to becoming a physician and the discomfort that reflects shortcomings of the training system.
- As the culture of medicine continues to shift, and as trainees become understandably less willing to tolerate unnecessary sacrifice, how should we set expectations around discomfort?
- More importantly, has the pendulum swung so far toward protecting trainee wellness that we have unintentionally deemphasized the pursuit of excellence? Or is that a false dichotomy altogether?
ACT 3: “OK, Boomer” – Kids These Days
- At this point, it would be easy to conclude that today’s trainees are simply less resilient than those who came before them. But after reviewing the literature, I don’t think the evidence supports that conclusion.
- It is worth remembering that nearly every generation has criticized the one that follows it. Complaints that younger people are less respectful, less hardworking, or less resilient are hardly unique to medicine.
- In fact, writings expressing these sentiments date back as early as 624 BC, illustrating just how enduring this pattern has been throughout history.
- Experimental psychologist John Protzko and colleagues popularized this phenomenon in 2019, describing it as the “Kids These Days” Fallacy. It refers to the remarkably persistent belief that younger generations are somehow declining, becoming less respectful, less motivated, less intelligent, or less resilient than those before them.
- What’s striking is that this phenomenon transcends cultures, historical eras, and domains of life. The complaints are remarkably consistent, whether they concern education, manners, work ethic, technology, or medicine itself.
- Even more remarkable is that these beliefs persist despite evidence to the contrary. Studies have shown that people continue to perceive younger generations as declining, even when presented with data demonstrating that no such decline exists.
- In other words, before we conclude that today’s trainees are fundamentally different, we should be cautious. History suggests that every generation believes the next one has lost something essential, and history also suggests that they are usually wrong.
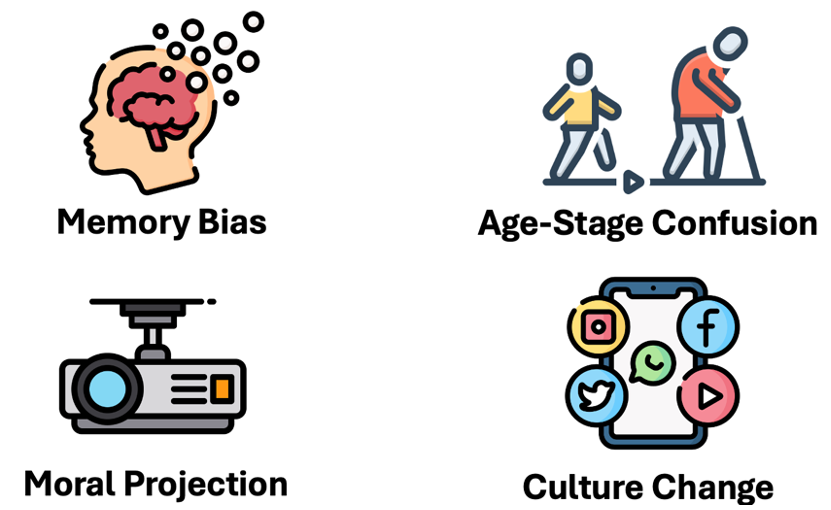
There are several well-described psychological mechanisms that help explain why the “Kids These Days” Fallacy is so persistent.
- Memory bias. We tend to remember our own generation more favorably than it actually was, conveniently forgetting the immaturity, poor judgment, and questionable decisions of our youth. In many ways, we project our current selves backward in time, remembering ourselves as more disciplined, responsible, and resilient than we truly were.
- Age-stage confusion. Differences that are really a function of age and life stage are often mistaken for evidence of generational decline. Being inexperienced, emotionally reactive, idealistic, or less comfortable with uncertainty are common features of youth, not necessarily signs that an entire generation has fundamentally different values. Young people often behave much the way young people always have.
- Moral projection. As we age, our priorities and values naturally evolve. Yet we often assume that because we would not behave a certain way today, younger people who do must possess inferior values. This ignores the fact that our own perspectives have changed over time.
- Cultural change. Every generation develops its own language, norms, technologies, and social expectations. These changes can feel unfamiliar or even threatening to older generations because they challenge established cultural norms and reduce the sense of authority that comes with experience. It is easy to mistake difference for deterioration.
- Taken together, these biases remind us that our perceptions of younger generations are not always objective. Before concluding that today’s trainees are uniquely entitled, fragile, or unwilling to tolerate discomfort, we should first consider whether we may be observing a phenomenon that has repeated itself for centuries.
Romanticiziation of the Past
- In many ways, we have a tendency to romanticize the past. We remember not only our own experiences more fondly than they were, but often an entire era as somehow better than the present.
- Interestingly, this tendency appears to be strongest in the domains in which we ourselves excel. Someone who loves reading may be convinced that “everyone used to read more.” Someone passionate about music may insist that music “used to be better.” We often mistake our own experiences and interests for those of an entire generation.
- Medicine is no exception. Many of us cling to the belief that the way we trained produced better physicians, often without recognizing how much nostalgia and cognitive bias may be shaping that conclusion.
- More importantly, there are compelling reasons why we should not simply preserve the training model we inherited.
- Modern medical residency is often traced back to William Stewart Halsted at Johns Hopkins Hospital, whose training model fundamentally shaped postgraduate medical education.
- Halsted developed much of this system while struggling with cocaine addiction, later compounded by morphine dependence after attempts to treat his addiction.
- His philosophy demanded total commitment to the hospital. Residents quite literally resided in the hospital, working extraordinary hours with little opportunity for sleep, family life, or personal identity outside of medicine.
- Thankfully, residency has evolved substantially since then. Residents no longer live in the hospital, duty hour restrictions exist in many jurisdictions, and post-call recovery has become an accepted part of training.
- Yet it is worth pausing to reflect on the origins of the system we inherited. The fact that our training model still bears recognizable features of one that was conceived under conditions so extreme that its architect required powerful stimulants simply to sustain it should give us reason to continually question whether tradition alone is sufficient justification for preserving it.

- There is little debate that meaningful problems exist within our current training environments, and the data support this.
- According to the 2025 Canadian Medical Association National Physician Health Survey, 58% of Canadian residents and fellows screened positive for depression on the PHQ-9.
- Other studies have shown that medical students begin training with mental health comparable to that of their non-medical peers. Yet within the first weeks of medical school, even before clinical rotations or meaningful patient contact, measures of depression, anxiety, and psychological distress begin to diverge. In other words, the deterioration in well-being starts long before trainees are exposed to many of the clinical stressors we often assume are responsible.
- Taken together, these findings make one thing abundantly clear: many aspects of medical training genuinely do need to change.
- Up to this point, however, much of this discussion has been framed as though wellness and competence exist in opposition, as though every gain in one must inevitably come at the expense of the other.
- Increasingly, medical educators are challenging that assumption. Rather than viewing wellness and excellence as competing priorities, an emerging body of work suggests this may be a false dichotomy altogether.
- Do and colleagues argue that physician well-being and competence are not competing goals, but mutually reinforcing ones.
- They contend that there is little evidence to support the long-held belief that suffering, exhaustion, or self-sacrifice are necessary ingredients for producing excellent physicians. Instead, they suggest this perceived trade-off reflects a historical culture within medicine that equated toughness with competence and endurance with professionalism.
- In contrast, the contemporary evidence overwhelmingly supports the opposite conclusion: improving trainee and physician well-being improves competence.
- This relationship has been demonstrated across a wide range of outcomes, including improved patient outcomes, higher-quality care, better clinical performance, greater empathy, stronger communication skills, and more resilient healthcare systems.
- Even relatively simple educational interventions support this principle. For example, pass/fail grading has consistently been associated with improvements in student well-being without compromising academic performance.
- Conversely, excessive work hours, sleep deprivation, psychological distress, and fatigue are all associated with increased rates of medical error and poorer clinical performance.
- Taken together, the evidence is remarkably consistent: prioritizing well-being enhances, rather than detracts from, physician competence.
- The benefits extend well beyond the individual learner. Physicians and trainees who feel supported and valued are more likely to remain in the profession, engage meaningfully in their work, and contribute positively to their teams.
- These effects ripple outward, improving retention, reducing turnover, strengthening workforce stability, increasing organizational efficiency, and ultimately enhancing continuity of patient care.
- For these reasons, Do and colleagues argue that supporting physician well-being is not simply a moral obligation. It is also a strategic investment in the future of the healthcare system.

- A forthcoming paper by Ottawa’s own Dr. Ahn introduces the concept of desirable difficulty, offering a framework for reconciling wellness and competence.
- The premise is simple: an educator’s role is not to eliminate difficulty in pursuit of comfort or likability, but to intentionally create learning experiences at the optimal challenge point; difficult enough to promote growth, but not so overwhelming that they lead to frustration or disengagement.
- Ahn and colleagues argue that psychological safety and desirable difficulty are complementary, not competing, conditions. Challenge without support can feel threatening, while support without challenge limits learning.
- The goal, therefore, is not to eliminate discomfort, but to distinguish between the discomfort that helps trainees grow and the discomfort that serves no educational purpose.
Zone of Proximal Development
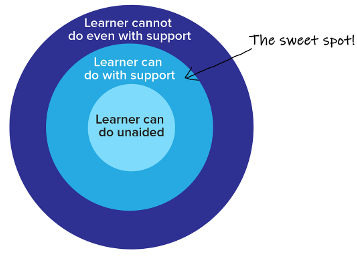
- Dr. Ahn also highlights the importance of teaching within the Zone of Proximal Development (ZPD), the range of tasks a trainee cannot yet perform independently but can accomplish with guidance from a more experienced physician.
- This is the space just beyond a learner’s comfort zone, where challenge is balanced with support and meaningful learning occurs.
- A classic example is a junior resident managing overnight consults with ready access to a senior resident or fellow. The challenge promotes growth, while the supervision provides psychological safety.
- That same situation, however, becomes unnecessary discomfort when appropriate supervision is unavailable, leaving a junior learner to manage critically ill patients beyond their level of training alone.
Act 4: Lights, Camera, ACTION! Where do we go from here?
- If wellness and competence are not competing goals, then the question becomes: what practical steps can trainees, educators, and healthcare systems take to create learning environments that promote both?
- Rebuilding trust will require humility, connection, and a shared commitment from everyone involved. As Dr. Ahn writes:
- Rebuilding trust will require humility, connection, and a shared commitment from everyone involved. As Dr. Ahn writes:
“Learning is not a solo endeavor, care is not delivered in isolation, and professional identity is shaped in and through relationships with others.” Improving medical education will require a collective, rather than an individual, approach.
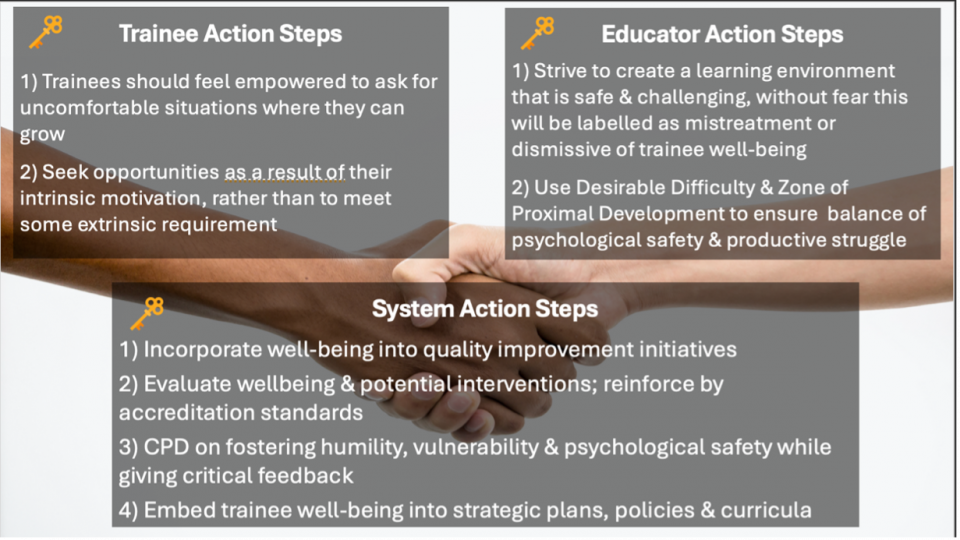
For Trainees
- Just as good parents allow their children to struggle at a level that is developmentally appropriate, good educators do the same for their learners. The goal is not to make training comfortable, but to provide the right amount of challenge with the right amount of support.
- It is also important to recognize that many of the cultural shifts occurring in medical education are not unique to medicine. Similar changes are occurring throughout education and parenting, reflecting broader changes in how society thinks about learning, motivation, and personal growth.
- For example, educational philosophy has shifted away from simple praise such as “Great job” or “I’m proud of you.” Instead, there is greater emphasis on continuous improvement and intrinsic motivation, asking questions like, “What will you do next?” or “Are you proud of what you’ve accomplished?”
- Decades of educational research suggest that intrinsic motivation is a far more powerful driver of deep learning, resilience, and long-term performance than external validation alone.
- It is also important to recognize that many of the cultural shifts occurring in medical education are not unique to medicine. Similar changes are occurring throughout education and parenting, reflecting broader changes in how society thinks about learning, motivation, and personal growth.
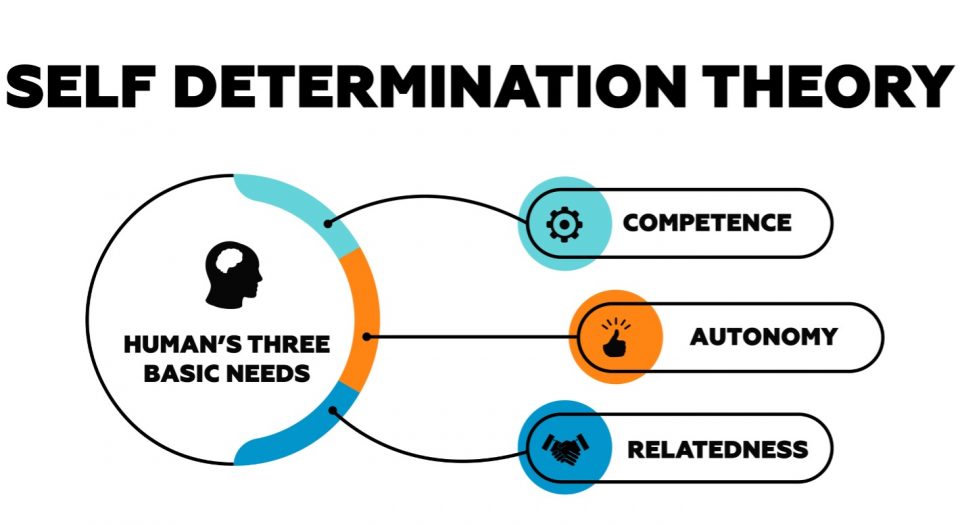
- A useful framework from vocational psychology is Self-Determination Theory, which proposes that three psychological needs underpin motivation and well-being:
- Competence: “I can do this, and I’m getting better.”
- Autonomy: “I choose to do this.”
- Relatedness: “I feel supported and connected.”
- Educational approaches that foster intrinsic motivation strengthen all three of these domains, promoting both well-being and deeper learning.
For Educators
- We often describe the educator-learner relationship as that of a coach and an athlete. The challenge in emergency medicine, however, is that we may only have a single shift to establish trust before asking learners to step into their Zone of Proximal Development and experience desirable difficulty.
- That makes it especially important to be explicit about why we challenge trainees.
- Dr. Jim Yang recommends setting expectations at the beginning of the shift, echoing advice he learned from Dr. Jason Frank during residency. He tells learners:
“My job as your teacher is to identify and fill gaps in your knowledge. To do that, I’m going to ask questions and challenge your thinking. I’m doing this to help you learn, not to make you feel bad for not knowing something. If I don’t challenge you, I haven’t done my job as an educator.”
- Dr. Doran Drew offers a similar approach to feedback, building on advice from Dr. Eric Clark. Rather than labeling the learner, he makes feedback action-oriented and forward-looking. A simple framework is: “To take things to the next level, next time I’d like you to…”
- When more difficult feedback is required, Dr. Drew recommends focusing on behaviours rather than the individual. For example:
“I’d like to talk about that case. I’m concerned that, if I hadn’t been there, the patient’s care may have been unsafe. I suspect there’s a knowledge gap here, which surprised me. Can you walk me through your thinking?”
- Small changes in language like these help communicate that challenge and support are not competing priorities. They reinforce that asking difficult questions and providing honest feedback are acts of investment in a trainee’s growth, not judgments of their worth.
For Medical Schools, Residency Programs, and Healthcare Systems
- The responsibility for creating healthy learning environments does not rest solely with trainees and educators. The institutions that shape medical education also play a critical role.
- As we’ve explored throughout this discussion, opinions differ on whether our current systems overemphasize wellness or fail to support it adequately. The reality is that most institutions are trying to balance two equally important responsibilities: supporting trainees while maintaining the standards required to produce excellent physicians.
- The challenge, then, is not choosing between wellness and competence, but designing systems that intentionally promote both.
- One issue that illustrates this tension particularly well is the increasingly debated question of when it is appropriate for trainees to call in sick to work.
- A 2025 study from Ottawa led by Lorenzo Madrazo examined illness presenteeism, the tendency for physicians and trainees to come to work despite being physically or psychologically unwell because of professional, cultural, or systemic pressures.
- The findings were striking: between 80% and 90% of physicians and trainees reported working while sick, with little evidence that this behavior has meaningfully declined since the pandemic.
- Illness presenteeism is associated with important downstream consequences, including poorer physician mental health, an increased likelihood of future prolonged sick leave, and higher rates of medical error.
- In other words, there is clear evidence that many physicians still come to work when they should not.
- At the same time, anecdotally, many educators perceive the opposite problem: that sick calls have become more common since the pandemic, with some questioning whether “sick days” are always being used for illness.
- Neither extreme serves medicine well. Working while genuinely ill is harmful to physicians, patients, and healthcare systems. Equally, unnecessary absenteeism places additional strain on colleagues and the healthcare system.
- Perhaps these observations are not as contradictory as they first appear. It may be that some of the perceived increase in sick calls simply reflects physicians feeling more comfortable staying home when they are legitimately unwell, a cultural shift that is both expected and appropriate after the pandemic.
Expert Opinion: Dr. Melanie Lewis
- Author of the recent false dichotomy publication, a practicing pediatrician and Chief Wellness Officer at the University of Alberta reflects that:
“Since Covid I think folks realize that is ok and professional NOT to come to work sick. I think more sick calls demonstrates we are starting to interrogate our “superhero/super human” constructs.
During the pandemic, we were told NOT to come to work with Covid, that it was irresponsible, unprofessional and dangerous to patients.
We developed back up call schedules, redundancy on in-patient and ED teams, and this is one of the positive legacy pieces coming out of Covid”
- One possible explanation comes from a common principle in organizational psychology: in most organizations, the vast majority of people want to do good work, act professionally, and follow established norms, while a much smaller minority will consistently test the boundaries of any system.
- The implication is an important one. Institutions should design policies for the majority, not the outliers.
- Most trainees come to work because they genuinely want to learn, be challenged, and provide excellent patient care. They should not be subjected to policies built around the small minority who may misuse the system.
- At the same time, programs must recognize that every system will occasionally be exploited. The solution is not to respond with blanket restrictions, but to identify and address outliers individually while preserving a culture of trust for everyone else.
Summary
Mastery
- Just as improving well-being can enhance competence, the reverse is also true: increasing competence is a powerful contributor to well-being.
- Well-being is deeply connected to mastery. Feeling capable, confident, and effective in one’s work provides meaning, purpose, and professional satisfaction.
Expert Perspective: Lisa Rosenbaum
- Dr. Rosenbaum argues that educators have a responsibility to create opportunities for trainees to undergo the transformation from novice to competent physician. As she puts it, “As educators, we owe it to trainees to place them in more circumstances that allow for these transformations into competent doctors.”
- She also emphasizes that competence is itself a cornerstone of well-being. If a trainee finishes residency without feeling prepared for independent practice, they are unlikely to thrive as a physician.
- More broadly, she reminds us that human beings are wired to seek purpose. If trainees lose sight of the idea that the sacrifices of residency are in service of becoming an excellent physician, then one of the most important sources of professional fulfillment is lost.
Expert Perspective: Adam Szulewski
- Dr. Szulewski, an emergency physician in Kingston and host of the KeyLIME podcast, echoes the importance of nuance. As he notes, “The world is full of echo chambers, and medicine is no exception.”
- Rather than viewing this debate as trainees versus educators, or wellness versus competence, he encourages us to recognize that there are legitimate perspectives on both sides.
Closing Thoughts
- So, as a final thought, I invite you to consider where you see yourself in this conversation.
- Whether you are a trainee, an educator, or someone who works alongside learners every day, I hope this discussion has encouraged you to reflect on your own assumptions and to better understand the perspectives of those on the other side.
- Because perhaps the goal of medical education is not to eliminate discomfort, nor to glorify it. It is to distinguish the discomfort that helps us become better physicians from the discomfort that serves no educational purpose.
References
- Adashi EY, O’Mahony DP, Gruppuso PA. The National Physician Shortage: Disconcerting HRSA and AAMC Reports. J Gen Intern Med. Published online May 6, 2025. doi:10.1007/s11606-025-09575-7
- Ahn E, Caverzagie KJ, Damodaran A, Huwendiek S, Lomis K, Marty AP, Turner D, Turner T, Atkinson A; on behalf of the International Competency-Based Education (ICBE) Collaborators. No Environment, No Education: Honoring the Clinical Learning Environment as the Engine of Competency-Based Education – A Call to Action. In Progress.
- Barger LK, Weaver MD, Sullivan JP, et al. Impact of work schedules of senior resident physicians on patient and resident physician safety. BMJ Med. 2023;2(1):e000320. doi:10.1136/bmjmed-2022-000320
- Bennett-Weston A, Keshtkar L, Jones M, et al. Interventions to promote medical student well-being: an overview of systematic reviews. BMJ Open. 2024;14(5):e082910. doi:10.1136/bmjopen-2023-082910
- Bonem EM, Fedesco HN, Zissimopoulos AN. What you do is less important than how you do it: the effects of learning environment on student outcomes. Learn Environ Res. 2020;23(1):27-44. doi:10.1007/s10984-019-09289-8
- Brazeau C, Shanafelt T, Durning S, et al. Distress Among Matriculating Medical Students Relative to the General Population. Acad Med. 2014;89(11):1520–1525. doi:10.1097/ACM.0000000000000482
- Canadian Medical Association. From pressure to progress: Results from the CMA’s 2025 National Physician Health Survey. CMA. Published October 14, 2025. Accessed January 26, 2026. https://www.cma.ca/latest-stories/pressure-progress-results-cmas-2025-national-physician-health-survey
- Chen TP. Young Doctors Want Work-Life Balance. Older Doctors Say That’s Not the Job. WSJ. Accessed April 25, 2025. https://www.wsj.com/lifestyle/careers/young-doctors-want-work-life-balance-older-doctors-say-thats-not-the-job-6cb37d48
- Chen T. Young doctors want work-life balance. Older doctors say that’s not the job. Wall Street Journal. November 3, 2024. Accessed January 30, 2026. https://www.wsj.com/lifestyle/careers/young-doctors-want-work-life-balance-older-doctors-say-thats-not-the-job-6cb37d48
- Coverdale JH. Virtues-Based Advice for Beginning Medical Students. Acad Psychiatry. 2007;31(5):354-357. doi:10.1176/appi.ap.31.5.354
- Do V, Lewis M, Goldstein C, Sonnenberg LK. Fostering a Health-Promoting Learning Environment in Medical Education: Adapting the Okanagan Charter for Administrators and Medical Educators. Acad Med. 2023;98(6):672-679. doi:10.1097/ACM.0000000000005159
- Do V, Lewis M, Li H. Advancing the well-being of staff physicians in Canada. CMAJ. 2025;197(39):E1316–E1317. doi:10.1503/cmaj.250852
- Do V, Lewis M, Li H. Wellbeing vs competency? Debunking the false dichotomy in medical education. Acad Med.Published online December 6, 2025. doi:10.1093/acamed/wvaf081
- Dyrbye LN, Massie FS, Eacker A, et al. Relationship Between Burnout and Professional Conduct and Attitudes Among US Medical Students. JAMA. 2010;304(11):1173-1180.
- Dyrbye LN, Thomas MR, Shanafelt TD. Systematic review of depression, anxiety, and other indicators of psychological distress among US and Canadian medical students. Acad Med. 2006;81(4):354-373.
- Dyrbye LN, West CP, Satele D, et al. Burnout among U.S. medical students, residents, and early career physicians relative to the general U.S. population. Acad Med. 2014;89(3):443-451. doi:10.1097/ACM.0000000000000134
- Dyrbye L, Shanafelt T. A narrative review on burnout experienced by medical students and residents. Med Educ.2016;50(1):132-149. doi:10.1111/medu.12927
- Dyrbye L, Meyers D, Ripp J, Dalal N, Bird S, Sen S. A pragmatic approach for organizations to measure health care professional wellbeing. Perspectives | Expert Voices in Health & Health Care, NAM | 2018
- Edmondson AC, Kerrissey MJ. What people get wrong about psychological safety. Harv Bus Rev. May–Jun 2025:52–59.
- Fahrenkopf AM, Sectish TC, Barger LK, et al. Rates of Medical Errors Among Depressed and Burnt Out Residents: Prospective Cohort Study. BMJ. 2008;336:488-491.
- Frank J, Snell L, Sherbino J. CanMEDS 2015 Physician Competency Framework. Published online 2015. Accessed July 31, 2025. https://canmeds.royalcollege.ca/en/framework
- Gladwell M. Offensive Play: How different are dogfighting and football? The New Yorker. October 11, 2009. Accessed January 15, 2026. https://www.newyorker.com/magazine/2009/10/19/offensive-play
- Harry E, Sinsky C, Dyrbye LN, et al. Physician Task Load and the Risk of Burnout Among US Physicians in a National Survey. Jt Comm J Qual Patient Saf. 2021;47(2):76-85. doi:10.1016/j.jcjq.2020.09.011
- Hauer KE, Chang A, van Schaik SM, et al. Evaluation of a Longitudinal Medical Student Coaching Program. Teach Learn Med. 2023;35(5):550-564. doi:10.1080/10401334.2022.2111570
- Hearn JH, Stocker CJ. Mindfulness practice correlates with reduced exam-induced stress and improved exam performance in preclinical medical students. BMC Psychol. 2022;10:41. doi:10.1186/s40359-022-00754-3
- Iyer AA, Hayes C, Chang BS, et al. Should Medical School Grading Be Tiered or Pass/Fail? A Scoping Review of Conceptual Arguments and Empirical Data. Acad Med. 2025;100(8):975. doi:10.1097/ACM.0000000000006085
- Jain PG, McBride ME, Caliendo A, Eppich W. Effects of Longitudinal Coaching on Relationships and Feedback Processes in Pediatric Subspecialty Fellowships. J Grad Med Educ. 2022;14(4):458-465. doi:10.4300/JGME-D-21-00936.1
- Klein E. Why This Psychologist Is Hopeful About Teen Mental Health. The Ezra Klein Show. New York Times; May 23, 2023. Podcast. Accessed [insert access date]. https://www.nytimes.com/interactive/2023/05/23/opinion/ezra-klein-podcast-lisa-damour.html
- Kumagai AK. Discomfort, Doubt, and the Edge of Learning. Acad Med. 2022;97(5):649. doi:10.1097/ACM.0000000000004588
- Lampe LC, Muller-Hilke B. Mindfulness-based intervention helps preclinical medical students to contain stress, maintain mindfulness and improve academic success. BMC Med Educ. 2021;21(1):145. doi:10.1186/s12909-021-02578-y
- Lee N, Appelbaum N, Amendola M, Dodson K, Kaplan B. Improving resident well-being and clinical learning environment through academic initiatives. J Surg Res. 2017;215:6-11. doi:10.1016/j.jss.2017.02.054
- Madrazo L, Choo-Foo J, Yu W, LaDonna KA, Domecq MC, Humphrey-Murto S. Going to work sick: a scoping review of illness presenteeism among physicians and medical trainees. Med Educ. 2025;59(5):469–483. doi:10.1111/medu.15538
- Mata DA, Ramos MA, Bansal N, et al. Prevalence of Depression and Depressive Symptoms Among Resident Physicians: A Systematic Review and Meta-analysis. JAMA. 2015;314(22):2373–2383. doi:10.1001/jama.2015.15845
- Mete M, Goldman C, Shanafelt T, Marchalik D. Impact of leadership behaviour on physician well-being, burnout, professional fulfilment and intent to leave: a multicentre cross-sectional survey study. BMJ Open. 2022;12(6):e057554. doi:10.1136/bmjopen-2021-057554
- Milestones by Specialty. Accessed July 31, 2025. https://www.acgme.org/milestones/milestones-by-specialty/
- National Academies of Sciences, Engineering, and Medicine. Taking Action Against Clinician Burnout: A Systems Approach to Professional Well-Being. National Academies Press; 2019. Accessed July 31, 2025. http://www.ncbi.nlm.nih.gov/books/NBK552618/
- National Plan for Health Workforce Well-Being – NAM. Accessed July 31, 2025. https://nam.edu/publications/national-plan-for-health-workforce-well-being/
- Nelson A, Eliasz KL. Desirable difficulty: theory and application of intentionally challenging learning. Med Educ.2023;57(2):123-130. doi:10.1111/medu.14916
- Oliver D. David Oliver: Moral distress in hospital doctors. BMJ. 2018;360:k1333. doi:https://doi.org/10.1136/bmj.k1333
- Protzko J, Schooler JW. Kids these days: Why the youth of today seem lacking. Sci Adv. 2019;5(10):eaav5916. doi:10.1126/sciadv.aav5916
- Rajendran L. Balancing service and education for the medical trainee. Can Med Educ J. 2022;13(3):75-76. doi:10.36834/cmej.74236
- Ramani S, Post SE, Könings K, Mann K, Katz JT, van der Vleuten C. “It’s just not the culture”: a qualitative study exploring residents’ perceptions of the impact of institutional culture on feedback. Teach Learn Med. 2017;29(2):153–161. doi:10.1080/10401334.2016.1244014
- Ripp J, Shanafelt T. The Health Care Chief Wellness Officer: What the Role Is and Is Not. Acad Med. 2020;95(9):1354-1358. doi:10.1097/ACM.0000000000003433
- Rosenbaum L. Beyond moral injury—can we reclaim agency, belief, and joy in medicine? N Engl J Med.2024;390(10):951–956
- Rosenbaum L. Being well while doing well—distinguishing necessary from unnecessary discomfort in training. N Engl J Med. 2024;390(6):568–574.
- Rosenbaum L. On calling—from privileged professionals to cogs of capitalism? N Engl J Med. 2024;390(5):471–476
- Rosenbaum L. What do trainees want? The rise of house staff unions. N Engl J Med. 2024;390(3):279–285.
- Rosenbaum L, host. Building Up Without Breaking Down [podcast episode]. Not Otherwise Specified. NEJM Group; March 20, 2024. Accessed January 12, 2026. https://not-otherwise-specified-podcast.nejm.org/e/building-up-without-breaking-down/
- Rosenbaum L, host. Injured, Not Sidelined [podcast episode]. Not Otherwise Specified. NEJM Group; May 8, 2024. Accessed January 13, 2026. https://not-otherwise-specified-podcast.nejm.org/e/injured-not-sidelined/
- Rosenbaum L, host. Revolutionary Rumblings [podcast episode]. Not Otherwise Specified. NEJM Group; January 31, 2024. Accessed January 10, 2026. https://not-otherwise-specified-podcast.nejm.org/e/revolutionary-rumblings/
- Rosenbaum L, host. Tough Love [podcast episode]. Not Otherwise Specified. NEJM Group; February 14, 2024. Accessed January 12, 2026. https://not-otherwise-specified-podcast.nejm.org/e/tough-love/
- Rosenbaum L, host. Walking the Dog [podcast episode]. Not Otherwise Specified. NEJM Group; April 24, 2024. Accessed January 11, 2026. https://not-otherwise-specified-podcast.nejm.org/e/walking-the-dog/
- Rosenbaum L, host. Why We Work [podcast episode]. Not Otherwise Specified. NEJM Group; July 2, 2024. Accessed January 10, 2026. https://www.nejm.org/doi/full/10.1056/NEJMp2400689/
- Royal College of Physicians and Surgeons of Canada. Summer Rewind #1 [podcast episode]. KeyLIME+; 2024. Accessed November 12, 2025a. https://keylimepodcast.libsyn.com/summer-rewind-1
- Schutt A, Chretien KC, Woodruff JN, et al. National Survey of Wellness Programs in U.S. and Canadian Medical Schools. Acad Med. 2021;96(5):728. doi:10.1097/ACM.0000000000003953
- Shanafelt TD. Finding Meaning, Balance, and Personal Satisfaction in the Practice of Oncology. J Support Oncol.2005;3(2):157-164.
- Shanafelt TD. Physician Well-being 2.0: Where Are We and Where Are We Going? Mayo Clin Proc. 2021;96(10):2682-2693. doi:10.1016/j.mayocp.2021.06.005
- Shanafelt TD, Balch CM, Bechamps G, et al. Burnout and medical errors among American surgeons. Ann Surg.2010;251(6):995-1000. doi:10.1097/SLA.0b013e3181bfdab3
- Shanafelt TD, Noseworthy J. Effective Leadership and Physician Wellbeing: Nine organizational strategies to promote engagement and reduce burnout. Mayo Clin Proc. 2017;92(1):129-146.
- Shanafelt TD, West CP, Sinsky C, et al. Changes in Burnout and Satisfaction With Work-Life Integration in Physicians and the General US Working Population Between 2011 and 2017. Mayo Clin Proc. 2019;94(9):1681-1694. doi:10.1016/j.mayocp.2018.10.023
- Sinskey JL, Margolis RD, Vinson AE. The Wicked Problem of Physician Well-Being. Anesthesiol Clin. 2022;40(2):213-223. doi:10.1016/j.anclin.2022.01.001
- Slavin SJ, Schindler DL, Chibnall JT. Medical Student Mental Health 3.0: Improving Student Wellness Through Curricular Changes. Acad Med. 2014;89(4):573-577. doi:10.1097/ACM.0000000000000166
- Stergiopoulos E, Fragoso L, Meeks LM. Cultural Barriers to Help-Seeking in Medical Education. JAMA Intern Med.2021;181(2):155-156. doi:10.1001/jamainternmed.2020.7567
- Talbot SG, Dean W. Physicians aren’t ‘burning out.’ They’re suffering from moral injury. STAT News. Published July 26, 2018. Accessed January 27, 2026. https://www.statnews.com/2018/07/26/physicians-not-burning-out-they-are-suffering-moral-injury/
- Tawfik DS, Shanafelt TD, Dyrbye LN, et al. Personal and Professional Factors Associated With Work-Life Integration Among US Physicians. JAMA Netw Open. 2021;4(5):e2111575. doi:10.1001/jamanetworkopen.2021.11575
- Thompson D. Workism Is Making Americans Miserable. The Atlantic. February 24, 2019. Accessed January 30, 2026. https://www.theatlantic.com/ideas/archive/2019/02/religion-workism-making-americans-miserable/583441/
- Vogel L. Medical leaders propose appointing wellness officers to address physician burnout. CMAJ. 2019;191(9):E267. doi:10.1503/cmaj.109-5719
- Warchol J, Merritt C. Wicked problem: Allowing the “necessary discomfort” back into residency training: Is it time? In: International Conference on Residency Education; 2024.
- Wallack MK, Chao L. Resident Work Hours: The Evolution of a Revolution. Arch Surg. 2001;136(12):1426-1432. doi:10.1001/archsurg.136.12.1426
- Wasson LT, Cusmano A, Meli L, et al. Association between learning environment interventions and medical student well-being: a systematic review. JAMA. 2016;316(21):2237-2252. doi:10.1001/jama.2016.17573
- West CP, Dyrbye LN, Shanafelt TD. Physician burnout: contributors, consequences and solutions. J Intern Med.2018;283(6):516-529. doi:10.1111/joim.12752
- West CP, Shanafelt TD, Kolars JC. Quality of Life, Burnout, Education Debt, and Medical Knowledge Among Internal Medicine Residents. JAMA. 2011;306(9):952-960.
- West CP, Tan AD, Habermann TM, Sloan JA, Shanafelt TD. Association of Resident Fatigue and Distress with Perceived Medial Errors. JAMA. 2009;302(12):1294-1300.
- Wisener K, Driessen E, Tan A, Cuncic C, Eva K. From constructive to critical and everywhere in between: education leaders’ decision-making related to harsh feedback from learners about their teachers. Adv Health Sci Educ Theory Pract.2025;30(2):497–513. doi:10.1007/s10459-024-10367-7
- Yerkes RM, Dodson JD. The Relation of Strength of Stimulus to Rapidity of Habit Formation. J Comp Neurol Psychol.1908;18:459-482. doi:10.1002/cne.920180503
- Zeglin A, McCarthy M, Nedorost S, Dell M, Logio L. Psychological distress in the era of psychological safety. J Gen Intern Med. 2025;40(1):38–40. doi:10.1007/s11606-024-08893-6
- Zimmermann C, Strohmaier S, Herkner H, Niederkrotenthaler T, Schernhammer E. Suicide rates among physicians compared with the general population in studies from 20 countries: gender stratified systematic review and meta-analysis. BMJ. 2024;386:e078964. doi:10.1136/bmj-2023-078964
