

Hypothermia results in slightly over one hundred deaths per year in Canada; typically as a result of primary hypothermia, frostbite and other cold exposure injuries (Toronto Public Health, 2014). In the United States, this is estimated at 1500 deaths annually (Baumgartner 2008). Both are likely underestimates of the scope of illness, as it only represents patients brought to a hospital, identified as hypothermic and where this was listed as the cause of death. A chart review of hypothermia cases in Finland over a ten year period showed the most common mechanism of hypothermia was cold water immersion (48%), cold environment exposure (39%), or submersion (13%) (Silfvast 2003).
In part one of a two-part series, we seek to review the scope and principles of hypothermia, how to appropriately measure temperature, discuss rewarming methods and review the current existing guidelines and evidence around hypothermia management.
Physiology
- Hypothermia is defined by a core temp< 35oC
- Primary hypothermia = body cannot match environmental stress
- Secondary hypothermia = medical condition (eg. anorexia, hypoadrenalism)
- The normal response to cold is to increase metabolic rate, muscle tone, shiver, and peripheral vasoconstriction. For mild cold exposures, this is adequate. However, behavioural responses (eg. seeking shelter or clothing) are our most effective methods. (Danzl 2012)
- Shivering (Bristow 1988, Tikuisis 1999)
- 32-35 °C: shivering increases with decreases in skin temperature or core temperature to 32°C
- 30-32 °C: shivering decreases
- <30 °C: shivering ceases
- Should be noted that variation in the onset or absence of shivering is seen, so should not be taken as absolute
- Metabolic rate (Wood 1991)
- <32 °C: metabolic rate slows
- 28 °C: oxygen consumption and pulse rate are about 50% of that of normothermia. Oxygen use decreases by about 6% per 1 °C drop.
- 18 °C: the brain can tolerate cardiac arrest up to 10x as long
- Rescue collapse is defined as a cardiac arrest that is related to the extrication and transport of a patient with deep hypothermia (stage HT III). Rescue collapse has been attributed to circulatory collapse due to hypovolemia, cardiac arrhythmias triggered by interventions, afterdrop, and further cooling.
- Afterdrop is defined as continued core cooling after rescue. It is thought that ongoing heat loss (conductive loss from warm core to cool extremities, and convective loss to blood as flow is increased to the extremities and cool peripheral blood returns centrally). It is further theorized that moving extremities can result in more blood return, and more afterdrop – this is part of the reason for avoiding excessive movement of a cold patient. There is controversy on its clinical significance, or if it even exists. (Giesbrecht 1992, Romet 1988, Baumgartner 1992, Vassallo 2011)
Staging of Hypothermia
- Method: staging is based on core temperature
- Absence of shivering is suggestive of temperature < 30 oC, but can be variable and is not reliable enough for assessment
- AHA classification (Truhlar 2015): based on core temperature, using 30 oC cutoff for severe. This is when the likelihood of VF is much higher. Mild (>34 C), moderate (30- 34 C), and severe (<30)
- Swiss system (Vanden Hoek 2010) – Developed to help rescuers estimate core temperature clinically. ERC and WMS prefer the Swiss system, as it includes clinical criteria. It is important to note that there may be variability in clinical presentations:
- HT I: clear consciousness with shivering: 35 to 32C – mild
- HT II: impaired consciousness without shivering: 32 to 28C – moderate
- HT III: unconscious: 28 to 24C – severe
- HT IV: apparent death: <24C – profound
- HT V: death due to irreversible hypothermia: < 13.7C – irreversible? (has since been recover from a case 9 C)
Core temperature measurement
- Body temperature varies by site, perfusion state, and environmental temperature
- Core temperature is a more accurate reflection of the temperature of the heart and body physiology.
- Core temperature is a requirement for staging based on temperature.
- Additionally, probes must be properly calibrated and low temperature-sensing
Primary options: Esophageal, Rectal, Bladder, Tympanic membrane (epitympanic). Not acceptable: Oral, temporal, infrared cutaneous, aural (Vanden Hoek 2010, Zafren 2015)
- Esophageal
- If intubated or comatose
- Advance to lower 1/3 (~24cm below larynx)
- Most reliable and accurate, but can be falsely elevated by heated air or gastric lavage
- Rectal
- Reasonable option if not intubated, or if esophageal or tympanic not available
- Advance to 15cm
- Can lag behind true core temperature up to 1 hour
- May be falsely elevated during colonic lavage
- ERC and WMS de-emphasizes it
- Bladder
- Reasonable option if not intubated, or if esophageal or tympanic not available
- Unique catheter with temperature probe
- Can lag behind true core temperature up to 1 hour, less reliable, ERC de-emphasizes it
- May be falsely elevated during bladder or peritoneal lavage
- ERC and WMS de-emphasizes it
- Tympanic membrane (epitympanic)
- Must be in contact with TM
- Theoretically reflects brain temperature, but need good access/contact
- Probably as accurate as esophageal, but logistical challenges make it hard to use
- When cardiac output is low, the epitympanic temperature is lower than core temperature
Rewarming Methods
- There is minimal data regarding a target rate of rewarming, and there are no specific recommendations
- Typical rates seen in literature with minimally invasive methods are 0.5-2.5 °C/hr , with higher rates in children. Typical rates with ECMO are 6-9 °C/hr. (Brown 2012)
- Suggested:
- Without cardiac arrest –> target normothermia (>35 °C)
- With cardiac arrest + ROSC –> targetted temperature management (32-36 °C, as per local protocols)
- A meta-analysis by Saczkowski et al. suggested that a slower rate of ECLS rewarming (6.0 °C/hr vs 7.8 °C/hr) may be independently associated with improved neurologic outcome.
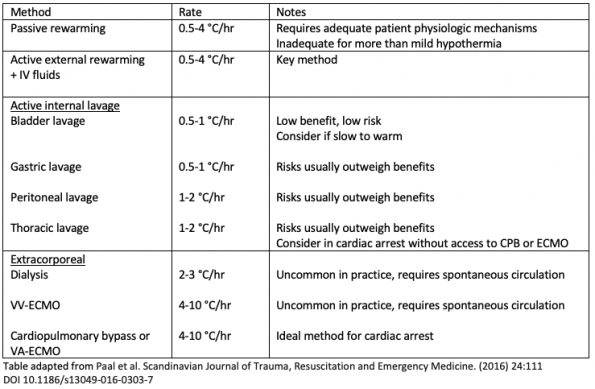
Passive rewarming
- Blankets, removing dry clothes
- Shivering and increased metabolic rate can generate about 1-3°C/hr (Brown 2012)
Active external rewarming
- Warmed blankets, warm packs, forced-air heating (eg. BAIR hugger), fluid heating blankets (eg. Blanketrol), distal limb rewarming
- Whole-body bath/shower increases return of cold blood, and is NOT recommended (Zafren 2015)
- Most of these methods are insufficient on their own, and should be used as a bundle. Forced air heating and fluid heating blankets are the most effective of these measures. (Brown 2012)
- Rewarming rate is about 0.5-4 °C /hr (Paal 2016)
- Key baseline method in all hypothermia. Enough on its own for the majority of cases, unless the patient is in cardiac arrest or has insufficient perfusion.
Active internal rewarming
- Heated humidified oxygen, warm IV fluids, body cavity lavage (bladder, gastric, colon, peritoneal, or thoracic)
- Heated oxygen and IV fluids are often included with active external rewarming methods as “minimally invasive rewarming”
- Intravenous fluids should be warmed (38 to 42°C)
- Very slow rewarming rate, but there is a benefit to not adding cool fluids
- Recommended by AHA and ERC (Truhlar 2015, Vanden Hoek 2010, Zafren 2015)
- Gastric/Colonic/Bladder lavage
- Usually seen in conjunction with other methods, without seeing a significant increase in rewarming rates
- Minimal heat transfer dependent on conduction
- Not recommended as they introduce complications and delay appropriate care in severe hypothermia or arrested patients (ie. ECMO) (Brown 2012)
- Bladder lavage can be considered, as the risk profile is minimal
- Peritoneal lavage – rate 1-2 °C/hr, poor outcomes, higher complications rates, not recommended (Paal 2016)
- Thoracic lavage
- According to case reports, thoracic lavage has cases of ROSC within 2 hours (Plaisier 2005). This is based on a small review of observational data (14 patients), despite reviewing articles 1966-2003. There is clearly publication bias, and the data should be interpreted as such.
- Reasonable, but high risk, alternative rewarming technique when ECMO or cardiopulmonary bypass is not available
- Rate 1-2 °C/hr (Paal 2016)
- Higher complication rates than typical rewarming scenarios (Danzl 2012, Taylor 2008)
- Complications were mostly pulmonary, bleeding, or related to severe hypothermia
Extracorporeal rewarming
- Heating outside of the body
- Without a pump – dialysis, VV-ECMO
- With a pump – VA-ECMO, Cardiopulmonary bypass (CPB)
- Extracorporeal Life-Support
- Extracorporeal life support (ECLS) is the supplementation or replacement of cardiopulmonary function. This is achieved through the use of machines (eg. heart-lung machine) for removal of blood, gas exchange, rewarming, and return of blood with pump function to maintain perfusion. Unlike other rewarming methods, ECLS can provide rapid rewarming even if there is cardiac arrest.
- Includes CPB and VA-ECMO methods
- Both methods require advanced procedures and equipment, anticoagulation (heparin), and a dedicated perfusionist providing direct care
- Cardiopulmonary bypass typically refers to a heart/lung machine used in the operating room.
- VA-ECMO is similar in providing cardiac and respiratory support, but is a simplified version without a venous reserve. Extrathoracic cannulation is used, typically femoral-femoral or femoral-jugular. Catheters are smaller, only partial anticoagulation is needed, and the system can be used for days rather than hours.
- ECMO is starting to supplant CPB based on better outcomes evidence in avoiding late cardiovascular collapse (Ruttman 2007, Mazur 2019)
- Indications:
- Hemodynamic instability (e.g. systolic blood pressure <90 mmHg, ventricular rhythms)
- Cardiac arrest or non-perfusing rhythms
- Core temperature < 28°C
- Efficacy
- A recent analysis of 44 observational studies and 40 case reports by Saczkowski et al. 2018, comprising 658 patients with accidental hypothermia treated with ECLS, revealed an overall survival rate with a good neurologic outcome of 40.3%
- Overall survival with good neurologic outcome among patients treated with ECLS is about 40.3%, based on a meta-analysis of observational data (Saczkowski et al., 2018). This is compared with roughly 10% survival without (Silfvast 2003), yielding an NNT of 3.
- Prior estimates were about 47-63%, which is probably an overestimate based on the nature of observational data. (Brown, 2012)
- Traditionally, CPB has been used for rewarming in low-perfusion states. However, overall survival is better with modern ECMO techniques (Ruttman 2007, Mazur 2019).
Resuscitation in Hypothermia
- The optimal hemodynamics and circulation for adequate perfusion in severe hypothermia (<28 °C) is not clear, as the brain can tolerate much lower perfusion states for a strikingly long time. (Lexow K 1991, Forti 2019)
- How long to check for a pulse? – 60 sec
- Non-perfusing rhythm (VF, VT, asystole) vs. Perfusing rhythm (PEA)
- Arterial lines are helpful for pulse and hemodynamic monitoring in real-time
- End-tidal CO2 may be helpful as a data point for the effectiveness of perfusion
Contrasting the Hypothermia guidelines
There are two major resuscitation guidelines (AHA and ERC), as well as the WMS society guidelines. The strength of evidence and/or recommendation is presented here as reported by the authors, or has been estimated where the authors did not report it.
On CPR:
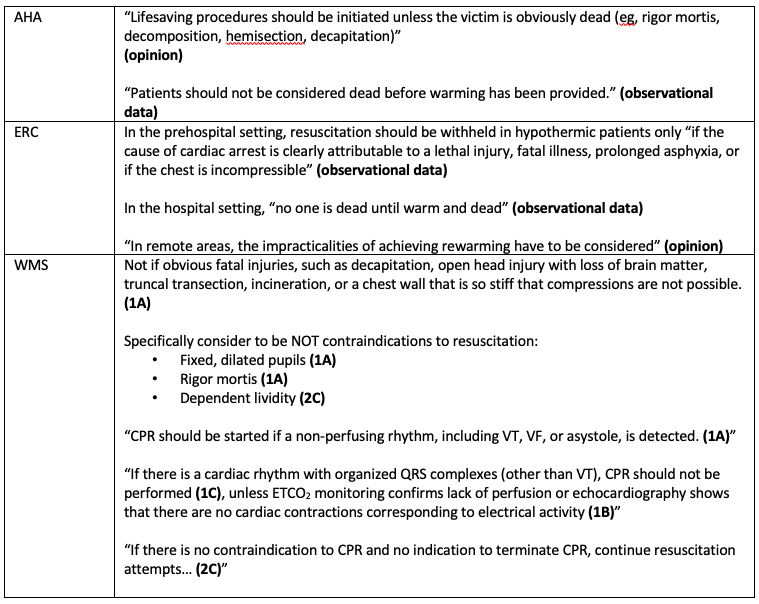
- Deciding when attempts are futile is challenging
- Classic signs of death are unreliable. AHA includes rigor mortis as a marker of obvious death, but this is not specific to hypothermia and is not reliable. Do not rely on pupils, rigor mortis, or dependent lividity as markers of obvious death.
- Consider practicalities in remote environments
- When in doubt, “No one is dead until warm and dead”
Defibrillation

- Atrial dysrhythmias are well tolerated and resolved with warming (Rankin 1984)
- Various practices are supported by guidelines, with limited evidence for all of them:
- Regular ACLS (per AHA)
- Shock x3, then wait until >30°C before attempting again per standard ACLS (per ERC)
- Shock x1, then wait until 1-2°C warmer (per WMS)
- Evidence comes from,
- animal studies (Ujhelyi 2001) showing increase in occurrence of VF below 30 °C, and in recurrence after defibrillation
- case reports which typically have successful shocks when warmed to >30 °C
- expert opinion
- Prolonged VF states have been described, with subsequent full recovery and good neurologic outcome
Drugs: use of vasoactive and antiarrhythmics
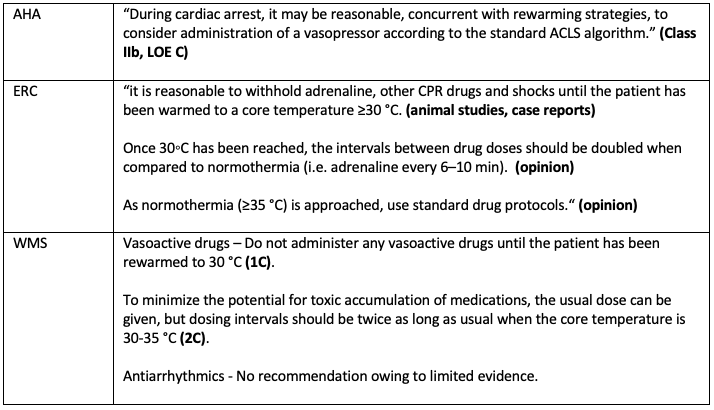
- The concern with standard ACLS drug regimens is that:
- the hypothermic heart may be unresponsive to cardioactive drugs
- drug metabolism is slowed with the temperature and pH change, leading to potentially accumulation of toxic plasma concentrations
- epinephrine may precipitate VF
- Lack of human evidence and a relatively small number of animal investigations
- Wira 2008 did a systematic review of animal studies performed. No head to head human studies, only case reports. Obviously very heterogeneous data, varying quality of studies, and not even the same animals. Looked at anti-dysrhythmics and vasopressors. Across studies there was improved ROSC in induced hypothermic animals given epinephrine or vasopressin (but all subsequently died or were euthanized). They did not see any benefit with amiodarone. Important limitations are that they did not follow usual ACLS (eg. drugs before shock in VF, atypical dosing, induced VF) and animals aren’t people.
- Various practices are supported by guidelines, with minimal evidence
- Regular ACLS (per AHA)
- Withhold epinephrine until >30°C, then double the interval between doses until >35°C (per ERC and WMS)
Airway and Procedures
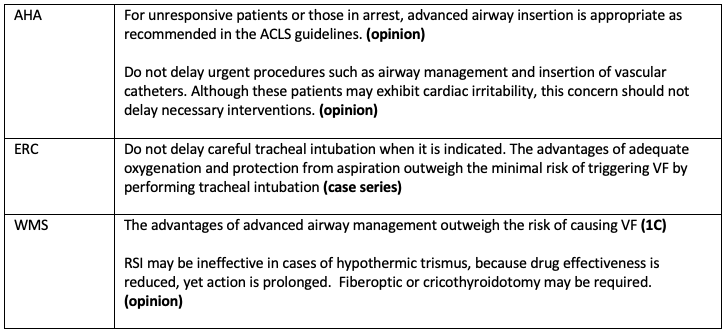
- Why intubate in severe hypothermia?
- The most common cause of death is pulmonary edema
- Reduced oxygen unloading – theoretic benefit from added oxygen
- Cold/frozen tissues can be difficult to ventilate without an advanced airway
- Cold-induced trismus is a thing
- The concern for intubation and invasive procedures is that the mechanical stimulation may precipitate a VF arrest, converting a potentially perfusing rhythm into a non-perfusing one.
- All guidelines support intervention when there is an indication, as the risk of triggering arrhythmias is outweighed by the need for intervention. Do not delay when indicated.
Stay tuned for part 2 !
References
- Baumgartner EA, Belson M, Rubin C, Patel M. Hypothermia and other cold-related morbidity emergency department visits: United States, 1995-2004. Wilderness Environ Med 2008;19:233-7.
- Silfvast T, Pettilä V. Outcome from severe accidental hypothermia in Southern Finland — a 10-year review. Resuscitation 2003;59:285-90.
- Danzl DF. Accidental hypothermia. In: Auerbach PS, ed. Wilderness medicine. 6th ed. Philadelphia: Mosby, 2012:116-42.
- Toronto Public Health. Health Impacts of Cold Weather. Technical Report. June 2014
- Bristow GK, Giesbrecht GG. Contribution of exercise and shivering to recovery from induced hypothermia (31.2 degrees C) in one subject. Aviat Space Environ Med 1988;59(6):549–52.
- Tikuisis P, Giesbrecht GG. Prediction of shivering heat production from core and mean skin temperatures. Eur J Appl Physiol Occup Physiol 1999;79(3):221–9.
- Wood S. Interactions between hypoxia and hypothermia. Annu Rev Physiol1991;53:71–85.
- Giesbrecht GG, Bristow GK. A second postcooling afterdrop: more evidence for a convective mechanism. J Appl Physiol 1992;73(4):1253–8.
- Romet TT. Mechanism of afterdrop after cold water immersion. J Appl Physiol 1988;65(4):1535–8.
- Vassallo S, Kathleen A. Chapter 15: Thermoregulatory principles, in Goldfrank’s Toxicologic Emergencies, Nelson et al., 9th Ed, 2011, The McGraw-Hill Companies.
- Truhlar A, Deakin CD, Soar J, et al. European resuscitation council guidelines for resuscitation 2015: section 4. Cardiac arrest in special circumstances. Resuscitation 2015;95:148–201.
- Zafren K, Giesbrecht GG, Danzl DF, et al. Wilderness Medical Society practice guidelines for the out-of-hospital evaluation and treatment of accidental hypothermia: 2014 update. Wilderness Environ Med 2014;25(4 Suppl):S66–85.
- Vanden Hoek TL, Morrison LJ, Shuster M, et al. Part 12: cardiac arrest in special situations: 2010 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Circulation 2010;122(18 Suppl 3):S829–61.
- Plaisier BR. Thoracic lavage in accidental hypothermia with cardiac arrest — report of a case and review of the literature. Resuscitation 2005;66:99-104.
- Taylor EE, Carroll JP, Lovitt MA, et al. Active intravascular rewarming for hypothermia associated with traumatic injury: early experience with a new technique. Proc (Bayl Univ Med Cent) 2008;21:120-6.
- Saczkowski et al. (2018) Prediction and risk stratification of survival in accidental hypothermia requiring extracorporeal life support: An individual patient data metaanalysis. Resuscitation 127 (2018) 51–57.
- Ruttmann E, Weissenbacher A, Ulmer H, et al. Prolonged extracorporeal membrane oxygenation-assisted support provides improved survival in hypothermic patients with cardiocirculatory arrest. J Thorac Cardiovasc Surg 2007;134:594- 600.
- Lexow K. Severe accidental hypothermia: survival after 6 hours 30 minutes of cardiopulmonary resuscitation. Arctic Med Res 1991;50:Suppl 6:112-4.
- Rankin AC, Rae AP. Cardiac arrhythmias during rewarming of patients with accidental hypothermia. Br Med J (Clin Res Ed) 1984;289(6449):874–7.
- Ujhelyi MR, Sims JJ, Dubin SA, Vender J, Miller AW. Defibrillation energy requirements and electrical heterogeneity during total body hypothermia. CritCare Med 2001;29:1006–11.
- Kornberger E, Schwarz B, Lindner KH, Mair P. Forced air surface rewarming in patients with severe accidental hypothermia. Resuscitation 1999;41:105-11.
- Dobson JA, BurgessJJ. Resuscitation of severe hypothermia by extracorporeal rewarming in a child. J Trauma. 1996;40:483–485.
- von SegesserLK, GarciaE, TurinaM. Perfusion without systemic heparinization for rewarming in accidental hypothermia. Ann ThoracSurg. 1991;52:560–561.
- Farstad M, AndersenKS, KollerME, GrongK, Segadal L, HusbyP. Rewarming from accidental hypothermia by extracorporeal circulation. A retrospective study. Eur J Cardiothorac Surg. 2001;20:58–64.
- Locher T, Walpoth B. Differential diagnosis of circulatory failure in hypothermic hypothermic avalanche victims: retrospective analysis of 32 avalanche accidents. Praxis 1996;85:1275-82. (In German.)
- Gilbert M, Busund R, Skagseth A, Nilsen PÅ, Solbø JP. Resuscitation from accidental hypothermia of 13.7 degrees C with circulatory arrest. Lancet 2000;355: 375-6.
- Darocha T, Kosin´ski S, Jarosz A, Drwila R. Extracorporeal Rewarming From Accidental Hypothermia of
- Patient With Suspected Trauma. Medicine, Volume 94, Number 27, July 2015
- Brown D, Brugger H, Boyd J, Paal P. Accidental Hypothermia, 2012, New England Journal of Emergency Medicine, 367;20.
- Forti A, Brugnaro P, Rauch S, Crucitti M, Brugger H, Cipollotti G, Strapazzon G. Hypothermic Cardiac Arrest With Full Neurologic Recovery After Approximately Nine Hours of Cardiopulmonary Resuscitation: Management and Possible Complications. Annals of Emergency Medicine Volume 73, no. 1 : January 2019.
- Paal et al. Scandinavian Journal of Trauma, Resuscitation and Emergency Medicine (2016) 24:111 DOI 10.1186/s13049-016-0303-7
- Meyer M, Pelurson N, Khabiri E, Siegenthaler N, Walpoth BH. Sequela-free long-term survival of a 65-year-old woman after 8 h and 40 min of cardiac arrest from deep accidental hypothermia. J Thorac Cardiovasc Surg. 2014;147(1):e1–2. doi:10.1016/j.jtcvs.2013.08.085.
- Nordberg P, Ivert T, Dalen M, Forsberg S, Hedman A. Surviving two hours of ventricular fibrillation in accidental hypothermia. Prehosp Emerg Care. 2014; 18(3):446–9. doi:10.3109/10903127.2014.891066
- Kosinski S, Darocha T, Jarosz A, Migiel L, Zelias A, Marcinkowski W, et al. The longest persisting ventricular fibrillation with an excellent outcome – 6 h 45min cardiac arrest. Resuscitation. 2016;105:e21–2. doi:10.1016/j. 2016.05.022.
- Althaus U, Aeberhard P, Schüpbach P, Nachbur BH, Mühlemann W. Management of profound accidental hypothermia with cardiorespiratory arrest. Ann Surg. 1982;195(4):492–5.
- Boue Y, Payen JF, Torres JP, Blancher M, Bouzat P. Full neurologic recovery after prolonged avalanche burial and cardiac arrest. High Alt Med Biol. 2014;15(4):522–3. doi:10.1089/ham.2014.1082.
- Putzer G, Braun P, Zimmermann A, et al. LUCAS compared to manual cardiopulmonary resuscitation is more effective during helicopter rescue – a prospective, randomized, cross-over manikin study. Am J Emerg Med 2013;31:384–9.51
- Mazur P, Kosiński S, Podsiadło P, Jarosz A, Przybylski R, Litiwnowicz R, Piątek J, Konstanty-Kalandyk J, Gałązkowski R, Darocha T. Extracorporeal membrane oxygenation for accidental deep hypothermia—current challenges and future perspectives. Ann Cardiothorac Surg 2019;8(1):137-142. doi: 10.21037/acs.2018.10.12
- Bolte RG, Black PG, Bowers RS, Thorne JK, Corneli HM. The use of extracorporeal rewarming in a child submerged for 66 minutes. JAMA 1988;260:377-9.
- Romlin BS, Winberg H, Janson M, Nilsson B, Björk K, Jeppsson A, et al. Excellent outcome With Extracorporeal Membrane Oxygenation after accidental profound hypothermia (13.8° C) and drowning. Crit Care Med. 2015;43:e521–5. doi:10.1097/CCM.0000000000001283.
- Locher T. Walpoth BH: [Differential diagnosis of circulatory failure in hypothermic avalanche victims: retrospective analysis of 32 avalanche accidents]. Praxis (Bern 1994). 1996;85(41):1275–82.


Hello,
Just wondering what the local (Ottawa) guidelines for AED use if there are no signs of circulation on hypothermic patients pre EMS arriving.
Thank you