

Patient experience and patient satisfaction during Emergency Department (ED) encounters has come to the forefront of ED quality improvement initiatives. To highlight the importance and evolution of patient experience during ED care, we seek to:
- Discuss the buzz around the term “patient experience”
- Outline evidence based ways to improve patient experience
- Assess the interaction between provider satisfaction and patient satisfaction
- Consider how we can improve patient experience in the ED
Question: Which of these things is not like the others?
- Early Defibrillation in shockable rhythms
- High Quality CPR
- Mastery of airway skills
- Patient Experience in our ED
Answer: This is a TRICK QUESTION… all of these components are equally important to Emergency Department (ED) care!
PART 1: Background Knowledge − Why Does Patient Experience Matter?
The Excellent Care for All Act
Patients are the consumers of health care and are important stakeholders. Since 2009, Ontario hospitals have been required to measure patient satisfaction in the ED. Measures such as satisfaction with wait times, staff interactions, pain control, and perception of the quality of medical services and communication are recorded for ED visits.(1,2) In 2010, The Excellent Care for All Act (ECFAA) came into legislation. This act was a formal way to put Ontario patients first by strengthening the focus and accountability of hospitals to deliver high quality patient care.(3)
The act required that hospitals:
- Establish quality committees that report on quality-related issues
- Create annual Quality Improvement Plans (QIPs) and make these available to the public
- Link executive compensation to the achievement of targets set out in the QIPs
- Establish a patient relations process to address and improve the patient experience
Domains of Quality
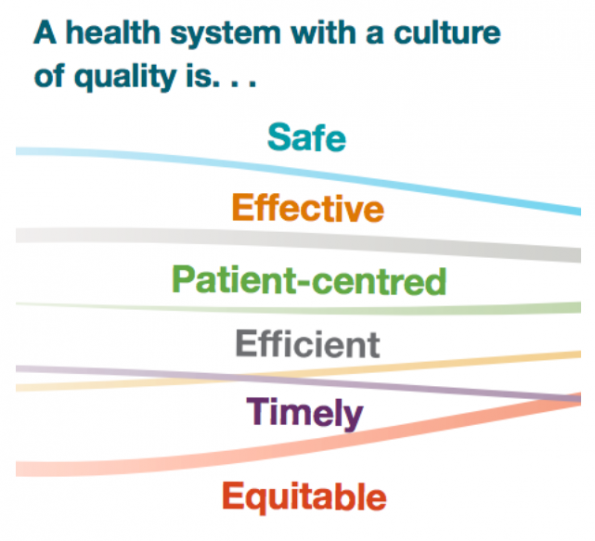
Health-care organizations around the world have been trying to improve the care delivered to patients by targeting different areas of quality. In 2001, The Institute of Medicine published “Crossing the Quality Chasm”, a report that laid out six domains to define a high quality health care system.(4) These six domains are:
- Safety: avoiding harm to patients
- Effectiveness: providing evidence based services
- Patient-centered: care that is responsive and respectful to patient preferences, needs, and values
- Efficient: avoiding waste of equipment and supplies
- Timely: reducing waits and possible harmful delays
- Equitable: providing care that does not vary in quality based on personal characteristics or geographic location
In 2015, Health Quality Ontario also released a report titled “Quality Matters: Realizing the Excellent Care for All Act”, which stated the province of Ontario would also be adopting these six domains of quality to create a provincial quality framework for our health care to achieve better performance.(3)
What do the Domains of Quality mean?
Although the definitions of the domains of quality are broad, they are supposed to provide us with an overall direction in which we need to steer our health care. Our province is prioritizing patient-centeredness as one of the key areas where we need to focus on improving the quality of our care.
If we look locally, the vision statement at The Ottawa Hospital (TOH) is “To provide each patient with world-class care, exceptional service, and compassion we would want for our loved ones.” This vision statement coupled with the fact that the TOH Quality Improvement Plan lists improving patient satisfaction as one of our hospital’s objectives for 2016/2017, certainly emphasizes that patient experience is not only a priority for our province but also our hospital.(5)
…but as front line clinicians, why should WE pursue improvement of patient experience?
Why Pursue Patient Satisfaction?
From a clinical perspective, patient experience should also be a priority for hospitals. Satisfaction can impact if patients follow prescribed treatments, treatment outcomes, and compliance with follow-up.(6,7) Improving patient satisfaction can also be a risk management technique. Common reasons for legal action against physicians include the need for more explanation and concerns with the standards of care; therefore, having satisfied patients may decrease malpractice suits.(8,9) Finally, there is also a connection between patient satisfaction and employee satisfaction whereby, having satisfied patients can improve staff morale and retention.(6,8)
In 2013, a systemic review by Doyle et al. showed that there is a link between patient experience, clinical safety, and effectiveness across a wide range of disease areas, study designs, settings, populations, and outcome measures.(10) This study helped to justify that patient experience is an important pillar of quality and that focusing on improving patient experience will increase the likelihood of improvements in patient safety and clinical effectiveness.
PART 2: What are Patients Really Looking for?

In 2010, a qualitative review of the patient satisfaction literature over the past 20 years, identified five primary factors of the ED experience that impact patient satisfaction: empathy, timeliness of care (waiting time), technical competence of care providers, information dispensation, and pain management.(8)
(1) Empathy
- “The art of caring”
- Uncaring attitudes are cited in 7-13% of ED complaints(11)
- More important than wait times as a predictor of patient satisfaction – speed does not compensate for rudeness, disrespect, or uncaring attitudes!(8)
(2) Timeliness of Care
- Patients overestimate the urgency of their need for health care; they do not understand the triage system and often perceive patient flow as being unfair.(12,13)
- Perceived waiting time is the most important contributor to patient experience around ED waiting. Higher patient satisfaction is not only associated with shorter waits but also with waits that are shorter than expected.(13,14)
- Examples of initiatives that improve timeliness of care in our ED include the rapid assessment zone and matching our shifts with peak patient volumes.
(3) Technical Competence
- Patients expect technical competence
- This is the bare minimum of what clinicians must provide
- Interestingly, patients have increased satisfaction when ED physicians perform bedside ultrasound.(15)
- This is an area where we can easily use our ultrasound training to impact our patient experience when clinically indicated!
(4) Pain Management
- Pain is a major symptom for which patients seek out emergency care.
- There is a correlation between pain relief and patient satisfaction.(16)
- Advanced pain directives at triage as well as standardized order sets (e.g. a renal colic protocol) help with quick symptom relief.
(5) Information Dispensation
- Information dispensation is correlated with improved patient satisfaction.
- Unexplained and uncertain waits feel longer
- Updates on patient progress and delays correlate with improved patient satisfaction.(12–14,17)
- A local needs assessment of the TOH waiting room patients showed that 91% of patients surveyed said they wanted wait times posted and 78% of patients told us that their satisfaction with their wait would be improved if wait times were posted.(18)
Recommendations:
Overall, what patients want seems pretty simple. They want empathy, timely care, competent physicians, pain relief, and information about their visit. I believe that we have the tools to cater to these issues without making drastic changes to the way we practice, and more importantly, these are components of care that we would all want for our loved ones.
PART 3: Challenges with Patient Experience
Our Reality: High Volume of “Not Sick” Patients
Appropriately, in our EDs we prioritize care for the sickest patients. However, when we find ourselves not taking care of sick patients as often as we think or hope, this leads to cognitive dissonance in our job. Furthermore, we get frustrated with patients presenting with non-urgent complaints who then become frustrated or demanding with their patient experience. Recent data from our ED shows that the percentage of CTAS 1 patients seen at TOH is under 1.5%. In contrast, the majority of our visits are CTAS 2-4. This data highlights the reality of the patient population we treat in our workplace. Although we must be excellent at resuscitation, the majority of our bread and butter patient volume is NOT resuscitation. We are first and foremost generalists who provide care to all types of patients at all times of the day. If we can understand that this is our reality, we can embrace it and not become frustrated with the less acute patients who want a positive experience when they present to our ED.
Forcing Empathy – Scripting
Another area where many clinicians may feel frustrated is the idea of forced or scripted ways to ensure empathy. The area of scripting has shown promise in improving the communication and interpersonal interaction of encounters with patients.(8) However, many find this awkward and cumbersome, which leads to feeling less empathetic towards patients. After all, don’t we all already have empathy for our patients and that is why we became physicians?
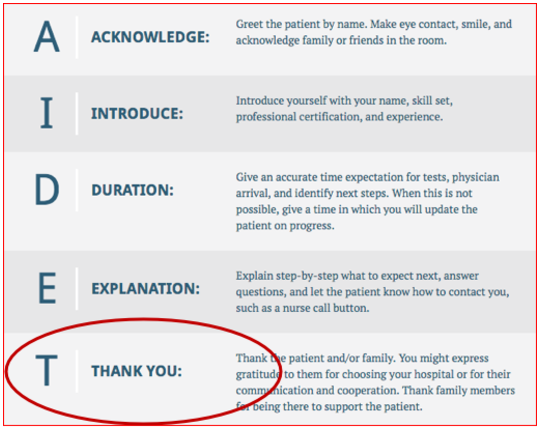
The most common dialogue to convey empathy is AIDET, which stands for acknowledge, introduce, duration, explanation, and thank you.(19) Most Canadian ED Physicians find this model challenging, particularly because of the THANK YOU component that seems to fit more of an American customer service model. Sometimes we just don’t want to thank patients for coming. Being forced to say things that make us feel unnatural can bring us to resent the importance of patient experience.
Measuring Patient Experience
The final complaint clinicians often have with patient experience is the way that it is measured. Though understanding patient perceptions can guide opportunities for improvement, patient satisfaction is often measured using survey techniques and is inherently subjective. Thus, a patient can receive the standard of care but still rate their experience as poor. Furthermore, hospitals use standardized validated questionnaires to measure patient satisfaction and these questions sometimes do not have enough granularity to elucidate what is influencing satisfaction. Finally, hospitals receive survey results monthly, which may not be frequent enough to know if initiatives are directly impacting patient experience. For example, if you were trying to lose weight and wanted to understand if the changes in your diet were making a difference, you would weigh yourself more than 12 times a year because data drives change.
Recommendations:
Firstly, our reality is that many of the patients we treat aren’t high acuity BUT we are experts at providing care for patients with all types of presentations who are sick, injured, and scared, and may have nowhere else to turn. I do not recommend we script our patient encounters or thank patients for every visit, but I do think that we can incorporate parts of AIDET into our daily practice and at least remember to introduce ourselves to patients and explain the next steps in their emergency visit. Finally, patient satisfaction scores are subjective and can be frustrating. When measuring patient satisfaction, perhaps we should consider conducting town hall meetings with patients and other stake-holders actively involved. We should also consider re-thinking the frequency at which we obtain patient experience data.
PART 4: Provider Wellness
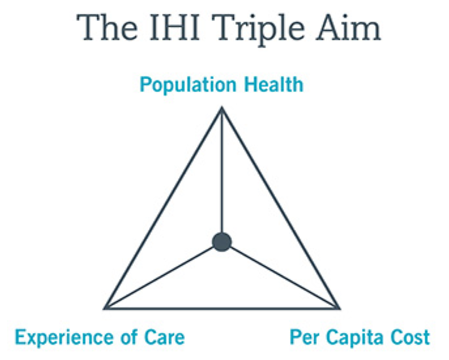
We cannot talk about patient satisfaction without discussing the importance of provider satisfaction. Below is an illustration of the Triple Aim. The Triple Aim is a framework that was initially developed by the Institute for Healthcare Improvement as an approach to optimize health system performance.(2) It was proposed that health institutions needed to pursue these three dimensions of performance to be a high performing organization:
- Improving the health of the population
- Enhancing the patient experience of care
- Reducing costs of health care
However, after the Triple Aim became popular, it became evident that hospitals that had adopted the Triple Aim as their organization’s framework were seeing that the work of clinical staff was becoming increasingly stressful and this was affecting their ability to actually carry out the Triple Aim.(20) From this came the publication of a new concept called the quadruple aim, which incorporates provider wellness.
Society expects more from us as physicians and staff. Patients want their health to better, they want to be seen in a timely fashion, and they want empathy. Unfortunately, this wide gap between social expectations and reality has set the stage for physicians to experience burnout. Burnout is associated with lower patient satisfaction, reduced health outcomes, and it may increase costs to our healthcare system. Burnout threatens the Triple Aim, so ultimately we must care for the provider to achieve patient satisfaction.(20)
A systematic review by Hall et al. (2016) looked at the impact of well-being and burnout on patient safety.(21) Of the studies that evaluated well-being, 16 studies found that poor well-being of staff had a correlation with worse patient safety. Furthermore, of the studies that looked at burnout, 21 studies found that high burnout was associated with worse patient safety. These studies highlighted that burnout does not only impact patient experience but also patient safety such as through medical errors.(21) This review illustrates the need for healthcare organizations to consider improving employee wellness/burnout to create a safer work environment and improve patient safety.
How can we be well in our increasingly stressful jobs?
Our ED is busier than ever and, according to hospital data, getting busier each year. Unfortunately, sometimes this leads us to feeling like we are not making progress in our jobs.(22) When we arrive to our shift with 25 patients waiting to be seen in the waiting room and leave with the same number of patients in the waiting room, we experience job frustration. There is no easy answer to how we can make our jobs more joyful. This needs to be tackled from many different angles. There are individual and interpersonal as well as departmental and organizational things that can be done to improve provider wellness.
For relevant reading, check out this article on PTSD in Emergency Physicians
Individual Ways to Influence Joy at Work
- Make an effort to connect with patients; this is why many of us pursued medicine in the first place
- Respect your colleagues and recognize their hard work
- Practice gratitude
-
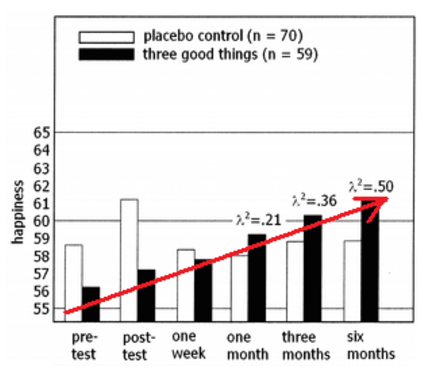
- In a study by Seligman et al., participants did a gratitude exercise where they wrote down three good things each day for one week. Findings from the study showed that, after one week, participants were 2% happier than before. In follow-up tests, their happiness kept on increasing. Participants enjoyed the exercise so much, that they kept on doing it on their own once the study ended.(23)
Organizational Ways to Influence Joy at Work
- Make provider wellness a priority
-
- E.g. Alcoa
- When Paul O’Neil became the CEO of Alcoa, he announced that his sole priority for the company was to increase worker satisfaction, and in turn, safety. The boardroom was shocked that O’Neil only listed the one priority, but O’Neil understood that satisfaction and sense of safety was a major concern for his workers and that without a feeling of safety, his company would not achieve success. Every day he made each worker come in and do an internal gut-check, which included three questions:
- Am I treated with dignity and respect?
- Do I have the things I need so I can make a contribution that gives meaning to my life?
- Am I recognized and thanked for what I do?
- Each question needed to be answered affirmatively every day by each worker.(24)
- O’Neil felt that if you could not answer yes to each of these questions, the full potential of the company could be compromised.(24) Over O’Neil’s 13 years as CEO, productivity soared as accident rates decreased from roughly one per week per plant to some plants going years without an accident. Alcoa’s annual income also grew 500%.(24)
- When Paul O’Neil became the CEO of Alcoa, he announced that his sole priority for the company was to increase worker satisfaction, and in turn, safety. The boardroom was shocked that O’Neil only listed the one priority, but O’Neil understood that satisfaction and sense of safety was a major concern for his workers and that without a feeling of safety, his company would not achieve success. Every day he made each worker come in and do an internal gut-check, which included three questions:
- E.g. Alcoa
- Look for innovative ways to increase provider wellness
-
- E.g. Windsor Regional Hospital instituted an unlimited vacation policy for non-unionized employees in 2014.
- Employees could take as much vacation as they wanted but it still needed to be approved by their supervisor and when they took vacation, they had to cover for one another.
- Their CEO believes that employees greatly appreciated this policy and that by covering vacation for each other, employees created a culture of support and teamwork. Furthermore, the CEO felt that when people were not on vacation that they were giving 110%.(25)
- E.g. Windsor Regional Hospital instituted an unlimited vacation policy for non-unionized employees in 2014.
Recommendations:
Provider wellness and burnout impacts patient experience and safety. The ED environment can make it difficult to achieve progress in our daily work. We must continue to pursue innovative individual and organizational strategies that make provider wellness a priority.
PART 5: Optimizing Patient Experience in the ED
When developing how we can optimize patient experience in our ED, looking to other centers can give us ideas and indications of what is possible.
Patient Engagement
In addition to focusing on improving patient experience, there has been an increasing push toward increasing patient engagement to improve quality and safety in healthcare organizations.(26) Patients may not have medical knowledge but they are users of our health care system and can provide a unique perspective on how we can improve care.(27) The idea behind patient engagement is more than patient-centered care, but actually having patients involved in the co-design of care, including participating in improvement projects.(27)
In 2010, Kingston General Hospital made a commitment “to ensure the voice and perspectives of patients [were] at the table for every decision that ha[d] a material impact on patients and families.” This commitment came about when KGH was facing significant financial issues, high infection rates, low public confidence, and poor staff morale. At this time, they recruited a new CEO and placed at least one patient adviser on every hospital working group and committee focused on patient safety and quality initiatives. Now, in part due to using this strategy, budgets are balanced, operating efficiencies have been achieved, and patient safety and quality of care has been improved. The CEO credits much of this improvement over a short period of time to patient engagement!(28)
Involving Patients in their Care
In 2010, an ICU nurse at Armstrong Institute at John Hopkins experienced having a family member in hospital. During this time, she felt helpless while the nurses would care for her loved one. After returning to work, she wondered if the families who watched her take care of their loved ones would also want to get involved. Gradually, she engaged family members to become more involved in patient care. This mindset eventually resulted in the development of a Family Involvement Menu (see below), which was a laminated sheet that gave family members options for how they could help care for their hospitalized loved one. Not only did this Family Involvement Menu get families involved in care but it also helped with quality of care and freed up nurses to do other tasks!(29)
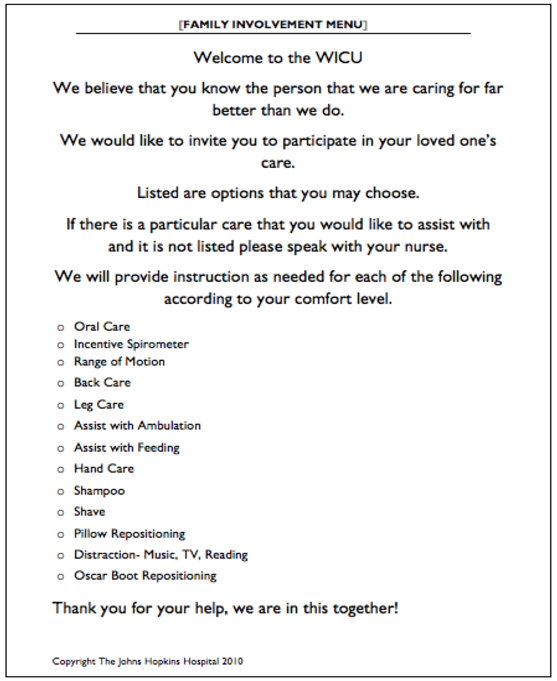
Like the ICU, the Emergency Department is a fast-paced environment and our nurses are extremely busy. Perhaps patient and family involvement menus could help families feel engaged and also manage our nursing workload? Consider what a Family Involvement Menu could look like in the Emergency Department; we could give families and caregivers a list of things they could help us with such as walking their family members to the bathroom, providing their family members with bed pans, and getting their family food or blankets.
Recommendations
Involving patients in the co-design of care processes may improve quality outcomes. Consider involving patients in the design, implementation, and evaluation of ED quality initiatives. Patients and Family members may be a resource. Consider involving patients and family members in providing basic needs for our patients in the ED.
Conclusion
Overall, the buzz around patient experience is only going to get louder. Improving patient experience can be challenging but it’s also important… so let’s embrace it and try to do it well! I hope that when my father, my mother, or I become a patient one day that we are treated in an empathetic, efficient, and informed way. I don’t want to feel ignorant to what is going on around me and I’m sure neither would you or your family. Dr. Jack Kitts, the CEO of The Ottawa Hospital, often says that “Patients come to us at their worse, so we need to be at our best.”
References
- Association OH. Leading Practices in Emergency Department Patient Experience Prepared for the Ontario Hospital Association by InfoFinders. 2011.
- Experience OP, Strategy M. Ontario Patient Experience Measurement Strategy. 2016;
- Health Quality Ontario. Quality Matters: Realizing Excellent Care for All. 2015;1–24. Available from: http://www.hqontario.ca/portals/0/Documents/pr/realizing-excellent-care-for-all-en.pdf
- Crossing the Quality Chasm. 2000. p. 23–56.
- Health Quality Ontario. Quality improvement plan (QIP): Guidance document for Ontario’s health care organizations. 2015;(November):1–21.
- Boudreaux ED, Cruz BL, Baumann BM. The Use of Performance Improvement Methods to Enhance Emergency Department Patient Satisfaction in the United States: A Critical Review of the Literature and Suggestions for Future Research. Acad Emerg Med. 2006;13(7):795–802.
- Krishel S, Baraff LJ. Effect of emergency department information on patient satisfaction. Ann Emerg Med [Internet]. 1993;22(3):568–72.
- Welch SJ. Twenty Years of Patient Satisfaction Research Applied to the Emergency Department: A Qualitative Review. Am J Med Qual. 2010;25(1):64–72.
- Vincent C, Phillips A, Young M. Why do people sue doctors? A study of patients and relatives taking legal action. Lancet. 1994;343(8913):1609–13.
- Doyle C, Lennox L, Bell D. A systematic review of evidence on the links between patient experience and clinical safety and effectiveness. BMJ Open. 2013;3(1):e001570.
- Emergency department complaints one year analysis. Ann Emerg Med. 1987;16: 857-861.
- Boudreaux ED, O’Hea EL. Patient satisfaction in the Emergency Department: A review of the literature and implications for practice. J Emerg Med. 2004 Jan;26(1):13–26.
- Thompson DA, Yarnold PR, Williams DR, Adams SL. Effects of actual waiting time, perceived waiting time, information delivery, and expressive quality on patient satisfaction in the Emergency Department. Ann Emerg Med. 1996 Dec;28(6):657–65.
- Dickson D, Ford R, Laval B. Managing Real and Virtual Waits in Hospitality and Service Organizations. Cornell Hotel Restaur Adm Q. 2005;46(1):52–68.
- Durston W, Carl ML, Guerra W. Patient satisfaction and diagnostic accuracy with ultrasound by emergency physicians. Am J Emerg Med. 1999;17(7):642–6.
- Yanuka M. Soffer D, Halpern P. An interventional study to improve the quality of analgesia in the emergency deparment. CJEM. 2008; 10 (5):435-439.
- Thompson DA, Yarnold PR, Adams SL, Spacone AB. How accurate are waiting time perceptions of patients in the emergency department? Ann Emerg Med. 1996;28(6):652–6.
- Calder-Sprackman S, Kwok E, Bradley R, Landreville J, Calder L. (2016, June). What do patients want when it comes to publishing ED wait times? A Mixed -Methods Needs Assessment. Poster session presented at the Annual Canadian Association of Emergency Medicine Conference. Quebec, Qc.
- Struder Group. AIDET Patient Communication. Retrieved May 10, 2016 from: https://www.studergroup.com/aidet
- Bodenheimer T, Sinsky C. From Triple to Quadruple Aim Care of the Patient. Ann Fam Med. 2014;12 (6): 573–6.
- Hall LH, Johnson J, Watt I, Tsipa A, O’Connor DB. Healthcare staff wellbeing, burnout, and patient safety: A systematic review. PLoS One. 2016;11(7):1–12.
- The power of small wins [Internet]. Vol. 19, Human Resource Management International Digest. 2011. Available from: http://www.emeraldinsight.com/doi/10.1108/hrmid.2011.04419gaa.015
- Seligman MEP, Steen TA, Park N, Peterson C. Positive Psychology Progress: Empirical Validation of Interventions. Am Psychol. 2005;60(5):410–21.
- Kolesar PJ. Vision, Values, Milestones: Paul O’Neill Starts Total Quality at Alcoa. Calif Manage Rev. 1993;35(3):133–65.
- CBC News. Windsor Regional Hospital’s unlimited vacation called a success. Sept 29, 2014.
- Coulter A. Patient Engagement—What Works? J Ambul Care Manage. 2012;35(2):80–9.
- Bate P, Robert G. Experience-based design: from redesigning the system around the patient to co-designing services with the patient. Qual Saf Heal Care. 2006;15(5):307–10.
- Baker GR, Fancott C, Judd M, OConnor P. Expanding patient engagement in quality improvement and health system redesign: Three Canadian case studies. Healthc Manag Forum. 2016;29(5):176–82.
- 29. Wyskiel RM, Chang BH, Alday AA, Thompson DA, Rosen MA, Dietz AS, et al. Towards Expanding the Acute Care Team: Learning How to Involve Families in Care Processes. Fam Syst Heal. 2015;33(3):242–9.

