

The demographics in Canada are changing, with individuals becoming increasingly more obese. In 2014 over 40% of Canadians self-identified as being overweight or obese and this number is rising. Dr. Brittany Ellis brings us through a review of the differences in anatomy and physiology of the bariatric patient and how we can more effectively resuscitate the trauma patient on our next shift.
How are patterns of injury in the obese different to healthy weight individuals?
Safety restraints in vehicles were designed using a test dummy who is 76.2kg and 173cm tall with a BMI of 25.5. Individuals with obesity have been shown to wear seat belts less, and when they do wear them, they often do so incorrectly. New test dummies have been created with a BMI of 35, however to date there are no research outcomes, nor impact on seatbelt design.
In motor vehicle collisions, individuals with obesity have been shown to have:
- Increased hip excursion
- Increased lower extremity injury
- Increased incidence of rib fractures, pulmonary contusions
- Increased pelvic fractures
- Decreased risk of head injury
Overall, obese individuals tend to have a decreased injury severity index, however continue to have a higher risk of mortality. This raises the question of why, and whether there is anything that can be done in their management and resuscitation that can reduce mortality in this group.
How are people with obesity physiologically different to healthy weight individuals?
Airway
Individuals with obesity have increased soft tissue in their pharyngeal walls, uvula, tonsils, pillars, tongue and eryepiglottic folds . They also have a higher incidence of diabetes which leads to joint glycosylation and stiffness, including stiffness of the mandible, cervical spine and atlanto-occipital joints. Despite this, obesity does not specifically predict difficulty in intubation, it does however predict difficulty in bag-mask ventilation.
One should remember to consider typical factors for difficult intubation; increased neck circumference, high Mallampati score and shortened thyromental distance are predictive. When full airway assessment is not possible, as is often the case in obese trauma patients due to altered level of consciousness and cervical spine collars, obesity may be considered a surrogate of these indicators of difficult intubation.
Breathing
As expected obesity affects breathing overall including the small airways. Damage is multifactorial, whereby pro-inflammatory adipokines lead to airway remodelling and surfactant dysfunction. Continual collapse and reopening of small airways leads to lasting damage. Even with weight loss total lung capacity does not return to baseline.
Overall, these patients tend to have a VQ mismatch with a widened aA gradient, as damaged small airways leads to impaired gas exchange. This leads to a baseline hypoxemia, which is primarily compensated for by increasing respiratory rate preferentially to tidal volume. Increasing respiratory rate is more effort – work of breathing is between 30 and 400 % higher in morbidly obese individuals. As a result of these changes, obese patients have increased oxygen consumption and increased CO2 production.
Increased abdominal and thoracic loading lead to a diminished tidal volume due to poor compliance and impaired diaphragm movement. Overall, on exhalation the chest collapses and the diaphragm remains high resulting in a diminished functional reserve capacity (FRC) which soon approaches the residual volume. As this happens FRC falls so low that it is within closing capacity of the small airways, leading to further airway collapse and VQ mismatch.
Although the vital capacity, total lung capacity (TLC), and FRC may be maintained in mild obesity, they can be reduced by up to 30% in morbidly obese patients and up to 50% in severely obese patients. All of these changes are made worse when the patient is supine.
Airway collapse leads to atelectatic lungs and increase risk of barotrauma due to airway pressures required to open distal airways.
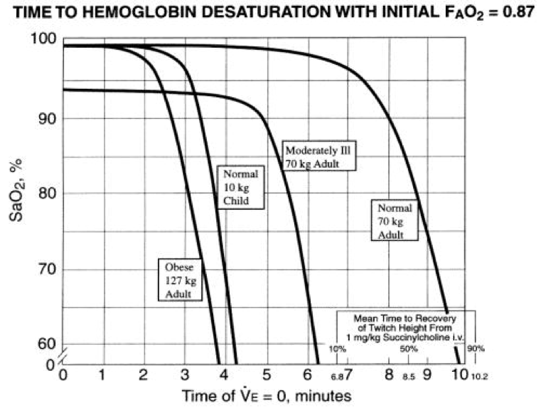
It also means that obese patients cannot tolerate even small insults to their respiratory systems such as effusions, contusions, chest wall injuries and pneumothoraces often seen in trauma patients. Subsequently, these changes lead to a more rapid desaturation during apneic periods, even in the setting of preoxygenation.
The time to apneic desaturation in an obese patient is significantly shorter than an otherwise healthy adult, or even one that is ill. The steep drop in regards to desaturation in the obese occurs at 96-97%, meaning pre-intubation management is exceptionally important.
Circulation
Obese patients have a number of significant differences in their circulatory system. They have a larger circulating volume, which may often predispose them to being under fluid resuscitated. Using a circulating volume estimate of 40-50cc/kg is more accurate for obese populations than the traditional 70cc/kg.
Individuals with obesity also have a number of risk factors for cardiovascular disease which increases their risk of conditions such as atrial fibrillation and heart failure leading to pulmonary edema – all of which are poorly tolerated given their compromised respiratory state at baseline.
The increased intra-abdominal pressure created by their adiposity, much like in pregnancy, can lead to decreased venous return through veno-caval obstruction, and effective hypovolemic shock.
Changes in obese patients have a significant impact, not only on the physiology, but also on assessment and treatment of circulatory issues:
- Phsycial exam impaired by adipose tissue, including abdominal exam and assessment of pelvis and long bones.
- POCUS FAST exam is more difficult as fat is a good attenuator of US waves.
- This is further hindered by potentially altered internal anatomy such as increased perinephric fat which can lead to incorrect diagnosis of free fluid.
- There have been studies to actually assess sensitivity of FAST exam on over-weight/obese patients – and although we all anticipate the sensitivity to be diminished, it would be still be worth-while to appreciate how confident, or not, we can be in our assessment.
Obese trauma patients have an increased risk of shock. In 2012, Nelson and colleagues performed a retrospective cohort analysis using a single centre trauma database in Europe to assess fluid resuscitation of trauma patients:
- Obese trauma patients are at significantly increased risk of persistent acidosis and mortality secondary to persistent shock and multi organ failure.
- Obese patients received significantly less fluid resuscitation than both normal and underweight groups. In fact, once corrected for circulating volume, this was on average 55% lower in the obese (xix).
In 2013 in Resuscitation, Heffner and colleagues published a retrospective cohort study of emergency intubations performed in a large, urban emergency department. Their aim was to identify risk factors for peri-intubation arrest. They found that obesity was an independent risk factor for perintubation arrest.
Imaging
Performing and interpreting images in patients with obesity can also be more difficult than health weight individuals:
- Xrays are often under penetrated due to the amount of adipose tissue they must traverse.
- In particular, elevated diaphragms and inferior lung collapse can make CXRs very difficult to interpret.
- US is technically more challenging due to adipose depth as well as pannus folds.
- CT scanner and the table are weight and diameter limited.
- At the Ottawa Civic Hospital in the Emergency Department the current weight limit 225kg, and diameter 70cm.
- The diameter is most often the limiting factor.
- CT head and thorax are often possible as long as the patient can get their arms above their heads and does not exceed weight limits.
- Unfortunately the abdomen and pelvis is sometime not possible due to abdominal girth.
How can we improve management and resuscitation of obese trauma patients?
Preparation
- Team preparation for safe and efficient patient transfers and assessment.
- Appointed RN/MD for access with appropriate back-up options available (Long arterial lines, long triple lumen central venous catheters, long-intraosseous access devices).
- Hoist and slings
- Bariatric stretcher/bed
- Airway equipment
- Pre-call appropriate services
Airway
Preoxygenation & Apneic Oxygenation
- Sitting patients up when possible increases apneic time to desaturation by an additional 52s in obese patients with BMI>35 when compared to supine position.
- Reverse Trendelenburg at 30 degrees likely increases apneic time to desaturation, but further studies are needed
- Preoxygenation with non-invasive ventilation increases apneic time to desaturation by:
- 37s when 7.5cm H2O CPAP used in morbidly obese.
- 61s when 10cm H2O CPAP in obese patients
- Apneic oxygenation further extends time to desaturation:
- 5L NP in obese patients increases apneic time to desaturation by over 1.5 minutes and results in a higher overall minimum SpO2
- THRIVE trial demonstrated a median apneic time to desaturation in difficult airway patients (50% obese) of 14 minutes, and no patient experienced desaturation of less than 90%
- Current research surrounding the role of apneic NIV to prolong desaturation in healthy weight individuals is promising, however has not been studied in obese populations
Positioning
- Placing patients in a ramped position, whereby the external auditory canal is in line with the sternal notch, improves larygoscopic views in the obese when compared to the traditional sniffing position
- Adjuncts for positioning which will be of use in the ED include:
- Troop pillow (or similar) to ramp the patient
- Body straps to prevent patient sliding
- Bariatric stretcher (ideally with foot down capabilities)
- Stool for the person intubating
LMA is recommended by the Anesthesia Society of America as the primary rescue device – as it is ‘obese resistant”. Outside the OR the LMA was found to have an overall success rate of 91% in the obese, with 98% of obese patients being successfully intubated, and 86% of morbidly obese patients.
- see Dr. Lauren Lacroix’s post regarding the physiologically difficult airway for more information on airway challenges.
Breathing
Regardless of whether the obese patient is intubated or not, positioning continues to be of utmost importance for maintenance of airway patency and improved ventilation.
- If possible, maintain in a seated position with the feet down to allow the abdomen to hang– the closer to 90’ the back can be, the better as this allows improved ventilation to the otherwise atelectatic bases.
- If ramped positioning was used for intubation this should be maintained at the very least.
- If the patient is on spinal precautions, the bed should be maintained in a minimum of 30’ reverse Trendelenburg and the patient strapped as required.
- For patients in respiratory distress CPAP and NIV strategies should remain first line, assuming no contra-indications exist.
- And for ventilated patients initial settings should be set to ideal body weight, and adjusted according to airway pressures (5-7ml/kg).
Circulation
Assessment of circulation in the obese can be difficult.
- Early arterial line insertion, or central line insertion improves ease of access and ability to monitor markers of perfusion. Assistance will be needed for ideal positioning of the patient and their tissue, and US guidance should be used due to the lack of anatomical landmarks.
- Failing insertion of PIV or CVC lines, intraosseus cannula continue to have an established role in gaining access in obese patients, even within the Emergency department. This includes alternative sites such as the distal tibia, proximal humerus and sternum (pending appropriate equipment). The yellow, 45mm EasyIO needle should be at hand.
- The obese patient should be positioned to offload the abdomen if possible, preferably by sitting them up with the legs down. Not only does this allow for increased diaphragm excursion and decreased IAP to improve ventilation, it may also allow for increased venous return and preload, improving hemodynamics.
- Always (always, always) – resuscitate before you intubate. If required temporize patients on NIV prior to intubation.
References
[1] Statistics Canada, CANSIM, table 105-0501 and Catalogue no. 82-221-X. Last modified: 2016-03-07. Accessed on 7 March 2017 at http://www.statcan.gc.ca/tables-tableaux/sum-som/l01/cst01/health81a-eng.htm
[1] Schlundt D, Briggs N, Miller S, et al. (2007). BMI and seatbelt use. Obesity. 15(11): 2541-5.
[1] Jehle D, Doshi C, Karahianis J, et al. (2014). Obesity and seatbelt use: a fatal relationship. Amer J Emer Med. 32:756-60.
[1] Arbabi S, Wahl W, Hemmila M, et al. (2003). The Cushion Effect. J Trauma. 54: 1090-93.
[1] Kent R, Forman J, Bostrom O. (2010). Is there really a “cushion effect”?: A biomechanical investigation of crash injury mechanisms in the obese. Obesity. 18:749-753.
[1] Maheshwari R, Mack C, Kaufman R, et al. (2009). Severity of injury and outcomes among obese trauma patients with fractures of the femur and tibia: A crash injury research and engineering network study (CIREN). J Orthop Trauma. 23(9): 634-639.
[1] Boulanger BR, Milzman D, Mitchell K, Rodriguez A. (1992). Body habitus as a predictor of injury pattern after blunt trauma. J Trauma. 33:228–232
[1] Tagliaferri F, Compagnone C, Yoganandan N, Gennarelli TA (2009). Traumatic brain injury after frontal crashes: relationship with body mass index. J Trauma. 66:727–729.
[1] Wang S, Bednarski B, Patel S, et al. (2003). Increased depth of subcutaneous fat is protective against abdominal injuries in motor vehicle collisions. 47th Annual Proceedings – Association for the Advancement of Automotive Medicine. 545 – 559.
[1] Aceto P, Perilli V, Modesti C et al. (2013). Airway management in obese patients. Surgery for obesity and related diseases. 9:809-15.
[1] El-Sohl A, Sikka P, Bozkanat E, et al. (2001). Morbid Obesity in the medical ICU. Chest. 120(6):1989-97.
[1] Langeron O, Masso E, Huraux C, et al. (2000). Prediction of difficult mask ventilation. Anesthesiology. 92(5):1229-1236.
[1] Brodsky J, Lemmens H, Brock-Utne, et al. (2002). Morbid Obesity and Tracheal Intubation. Anesth Analg. 94:732-6.
[1] Gonzalez H, Minville V, Delanoue K, et al. (2008). The Importance of Increased Neck Circumference to Intubation Difficulties in the Obese Patient. Anest Analg. 106:1132-6.
[1] Mashour GA, Kheterpal S, Vanaharam V, et al. (2008). The extended Mallampati score and a diagnosis of dia- betes mellitus are predictors of difficult laryngos- copy in the morbidly obese. Anesth Analg 107(6):1919–23.
[1] Benumof JL, Dagg R, Benumof R. (1997). Critical haemoglobin desaturation will occur before return to an unparalyzed state following 1 mg/kg intravenous succinylcholine. Anesthesiology. 87:979-982.
[1] Farmery A, Roe P. (1996). A model to describe the rate of oxyhemoglobin desaturation during apnoea. B J Anaes. 76: 284-291.
[1] Shashaty M, Stapleton R. (2014). Physiological and Management Implications of Obesity in Critical Illness. Ann Am Thorac Soc. 11(8):1286–1297.
[1] Nelson J, Billeter A, Seifert B, et al. (2012). Obese trauma patients are at increased risk of early hypovolemix shock: a retrospective cohort analysis of 1084 severely injured patients. Critical Care. 16: R77.
[1] Winfield R, Delano M, Lottenberg L, et al (2010). Traditional resuscitative practices fail to resolve metabolic acidosis in morbidly obese patients following severe blunt trauma. J Trauma. 68(2):317-30.
[1] Heffner A, Swords D, Neale M, Jones A. (2013). Incidence and factors associated with cardiac arrest complicating emergency airway management. Resuscitation. 84:1500-4.
[1] Altermatt F, Munoz H, Delfino A, Cortinez L. (2005). Preoxygenation in the obese patient: effects of positioning on tolerance to apnea. Br J Anaes. 95(5):706-9.
[1] Boyce J, Ness T, Castroman P & Gleysteen J. (2003). A Preliminary Study of the Optimal Anesthesia Positioning for the Morbidly Obese Patient. Obesity Surgery. 13:4-9.
[1] Cressey D, Berthoud M, Reilly C. (2001). Effectiveness of continuous positive pressure to enhance pre-oxygenation in morbidly obese women. Anaesthesia. 56(7): 680-684.
[1] Gander S, Frascarolo P, Suter M, et al. (2005) Positive End-Expiratory Pressure During Induction of General Anesthesia Increases Duration of Non-hypoxic Apnea in Morbidly Obese Patients. Anesth Analg. 100: 580-4.
[1] Ramachandran SK, Cosnowski A, Shanks A, et al. Apneic oxygenation during prolonged laryngoscopy in obese patients: a randomized, controlled trial of nasal oxygen administration. J Clin Anesth. 2010;22(3):164-168
[1] Patel A & Nouraei S (2015). Transnasal Humidified Rapid-Insufflation Ventilatory Exchange (THRIVE): a physiological method of increasing apnoea time in patients with difficult airways. Anesthesia. 70: 323-329.
[1] Grant S, Khan F, Keijzers et al. (2016). Ventilator-assisted pre-oxygenation: protocol for combining non-invasive ventilation and apnoeic oxygenation using a portable ventilator. Emergency Medicine Australasia. 28:67-72
[1] Collins J, Lemmens H, Brodsky J, et al. (2004). Laryngoscopy and morbid obesity: a comparison of the “sniff” and “ramped” positions. Obesity Surgery. 14:1171-5.
[1] Kim J, Mort T. (2010). The Role of the LMA in Emergency Airway Management of the Obese Patient Outside of the OR. Anesthesiology Annual Meeting. Abstract.

