

As we delve deeper into wellness week, an important consideration many of us often have is the time we have available to us. Our personal and professional lives are often so chaotic, it is easy to find excuses not to make time for wellness. Here, we will examine some select strategies from colleagues and the literature to help make us more efficient in our clinical environment, so that we can more effectively manage workflow and teaching, to enhance our overall wellness. If one is feeling productive and happy at work, this will permeate through the rest of their life as well.
Keeping up to date
While physicians traditionally attend conferences to keep up to date with the literature, we know that these tend to be more for socializing and reconnecting than for the medicine themselves. From an efficiency standpoint, there are likely better options available.
An excellent review discussed strategies for using online resources in Emergency Medicine (1). These include; Really Simple Syndication (RSS) reader, podcast app, compilations of quality resources, social networks such as Twitters and blogs, and custom search engines for resources. In particular, our group have highlighted some of the following as especially high yield:
- Compilations sites:
- EM lit of note: Reviews of some of the latest EM relevant literature
- Life in the Fast Lane: Excellent teaching topics, approaches to conditions, and a well populated ECG bank.
- REBEL-EM: Clinical pearls on educational topics, literature based reviews and excellent myth busting
- Podcasts:
- The Skeptics Guide to Emergency Medicine: educational topics, evidence based reviews and interesting cases, with an very engaging podcast style
- FOAM Cast: Educational topics in short, easy to digest podcast format
Work productivity
Almost everyone has an accessible smart phone with them at all times, rather than only being used for Facebook, these can help to assess frequently used information on clinical shifts.
- Dropbox (Free) – This is suited to include large files such as; teaching presentations, exam cases, conference handouts, published articles, and patient handouts. It can also be assessed from any work Desktop (in addition to own tablets and smartphones).
- Evernote (Free) – Excellent note taking software, with a robust search function and can look for keywords in texts, photos and even handwriting. It can search for notes taken from previous talks or through uploaded PDFs.
- Bugs and Drugs ($14.99) – There are many excellent apps for infectious disease resources, Bugs and Drugs is rather robust. Some others that are fairly high yield: Spectrum (for pediatric infectious disease – Free), Sanford Guide ($29.99/year).
- General medication Apps – Prescribe smart (Free) PediStat ($4.99), PEPID ($299.95/year), ePocrates ($174.99 US/year), UpToDate ($499 US/year with CMA discount)
- Discharge instructions: Some physicians use videos from Sunnybrook, Dr. Mike Evans’s back pain video, while others use handouts from American Family Physician or UptoDate. The incorporation of these handouts or videos allow you to optimize your time at work and help facilitate improved discharge of patients.
Minimize disruptions at work
Emergency physicians are interrupted roughly 9-12 times per hour (or, once every 5 minutes!) (2). Some interruptions are vital to patient care, however, many disrupt workflow and productivity, causing physicians to switch out of existing tasks and leading to errors. In the literature, functionally redesigning the environment, or creating “interruption free zones” and “times” (such as during handovers, medication administration and during procedures) are possible system-wide solutions (3).

However, there are also strategies for your next shift. Some physicians specifically choose a quiet(er) corner to work, and/or claim a computer for the entire shift to prevent logging on and off. Some use portable phones so they are less likely to miss calls and leave the patient’s beside. Grabbing multiple charts at once allows a physician to go from one patient room to another, and minimize non-urgent interruptions as a result of sitting at a desk. Perhaps the most important step in minimizing these interruptions however, is being cognizant of the fact that they exist, and knowing that the vast majority are non-critical.
When faced with an interruption, physicians almost always immediately engage the interruption task (4). Authors suggest alternative strategies such as; rejecting or delaying the interruption, rehearse the original task before switching, and placing cues to facilitate return to the original task.
Teaching efficiency
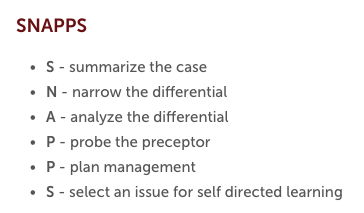
Much has previously been written on effective teaching strategies, so we won’t delve into them too much here, but some particularly useful methods are to; know the trainee, listen more, provide early feedback, expose trainees to cases and invite others to teach (5,6). A recent review had also recommended some utility in alternative teaching models, such as; the ‘one minute preceptor‘, ‘two minute observation’, activated demonstrations, teaching scrips and SNAPPS (7).
Although not well studied, there is likely utility in incorporating FOAMed content into teaching learners (why recreate the wheel, when someone has already done it?). For example, when discussing some potential pregnancy related emergencies, referring to a well done blogpost, and then debriefing with the learner allows a lot of knowledge dissemination, but saves you time. One intrinsic difficulty with this is that it requires you to know what is out there. Talking to some of our physicians, some particularly useful websites or blogposts are great starting points for discussion:
- MDCalc (include decision tools and most relevant articles)
- Learning Radiology (with cases for different level of learners)
- Life in the Fast Lane (large repository of test questions, images, EKGs and clinical cases)
- NEJM procedures (has videos on diverse types of procedures)
- EMOttawa blog (posting reviews on journal club articles, and core grand rounds posts)
- CanadiEM (excellent Canadian content on medical topics, opinions, and tricks for clinical practice).
Conclusions
While there might be an initial trial period in adopting new strategies, they should eventually lead to more efficient workflow, teaching and professional development, leaving us with more free time, and thus contributing to further physician wellness.
References
- Thoma, B., Joshi, N., Trueger, N. S., Chan, T., & Lin, M. (2014). Five Strategies to Effectively Use Online Resources in Emergency Medicine. Annals of Emergency Medicine, 64(4), 392–395. http://doi.org/10.1016/j.annemergmed.2014.05.029
- Chisholm, C. D., Collison, E. K., Nelson, D. R., & Cordell, W. H. (2000). Emergency department workplace interruptions: are emergency physicians “interrupt-driven” and “multitasking”? Academic Emergency Medicine : Official Journal of the Society for Academic Emergency Medicine, 7(11), 1239–1243.
- Anthony, K., Wiencek, C., Bauer, C., Daly, B., & Anthony, M. K. (2010). No interruptions please: impact of a No Interruption Zone on medication safety in intensive care units. Critical Care Nurse, 30(3), 21–29. http://doi.org/10.4037/ccn2010473
- Ratwani, R. M., Fong, A., Puthumana, J. S., & Hettinger, A. Z. (2017). Emergency Physician Use of Cognitive Strategies to Manage Interruptions. Annals of Emergency Medicine, 70(5), 683–687. http://doi.org/10.1016/j.annemergmed.2017.04.036
- Penciner, R. (2007). Clinical teaching in a busy emergency department: strategies for success. CJEM, 4(4), 286–288.
- Bandiera, G., Lee, S., & Tiberius, R. (2005). Creating effective learning in today’s emergency departments: how accomplished teachers get it done. Annals of Emergency Medicine. http://doi.org/10.1097/00001888-198808000-00003
- Green, G. M., & Chen, E. H. (2014). Top 10 ideas to improve your bedside teaching in a busy emergency department. Emergency Medicine Journal. http://doi.org/10.1136/emermed-2014-204211

