

In this post, we will review several recent updates related to pre-hospital medicine. Specifically, we will:
- Review the role of tranexamic acid (TXA) in pre-hospital trauma
- Discuss the use of ketamine in Excited Delirium
- Examine the new Ottawa ROSC bypass protocol and new modifications to the Trauma bypass protocol for pediatric patients
- Explore the Paramedic scope of practice in obstetric emergencies
TXA in Trauma
Basic Pharmacology
TXA is a synthetic derivative of the amino acid lysine. It is an anti-fibrinolytic agent that acts by binding to plasminogen and blocking the interaction of plasminogen with fibrin, thereby preventing dissolution of the fibrin clot.
History of TXA (J Trauma Acute Care Surgery, Napolitano et. al)
TXA has been available for more than 20 years and was first approved by the US Food and Drug Administration (FDA) in 1986 for short-term use (2 to 8 days) as an injection to reduce or prevent bleeding during tooth extraction in hemophilia patients. In November 2009, the FDA approved the oral form of TXA to treat menorrhagia
Summary of the evidence for use of TXA in Trauma:
Two main studies, CRASH-2 and MATTERS, provide the most compelling evidence for the use of TXA in trauma.
CRASH-2 Trial
The CRASH 2 trial is one of the first large studies to show a significant mortality benefit with the early administration of TXA. It was a large pragmatic international randomized placebo-controlled trial of the effects of the early administration of TXA (1 g over 10 minutes intravenously administered, then an intravenous infusion of 1 g over 8 hours) on 28-day hospital mortality, vascular events, and transfusions in adult trauma patients. The trial enrolled > 20 000 patients from 274 hospitals across 40 countries who either had significant bleeding or were at risk of significant bleeding.
Results
- All-cause 28-day mortality was 14.5% in TXA and 16.0% in placebo patients (RR 0.91)
- All-cause mortality reduction was 1.5%, with a NNT of 67 to save one life over 28 days.
- On the basis of the CRASH-2 Trial results, it has been estimated that TXA use could save between 70,000 and 100,000 lives per year worldwide. Considering the mortality benefit and the absence of evidence in the study to suggest a risk of harm, this is a significant result.
- There was no difference in the rate of vascular occlusive events (MI, CVA, PE, or DVT) between the two groups
- Based on the results of the CRASH-2 Trial, TXA was added to the World Health Organization list of essential medicines in March of 2011
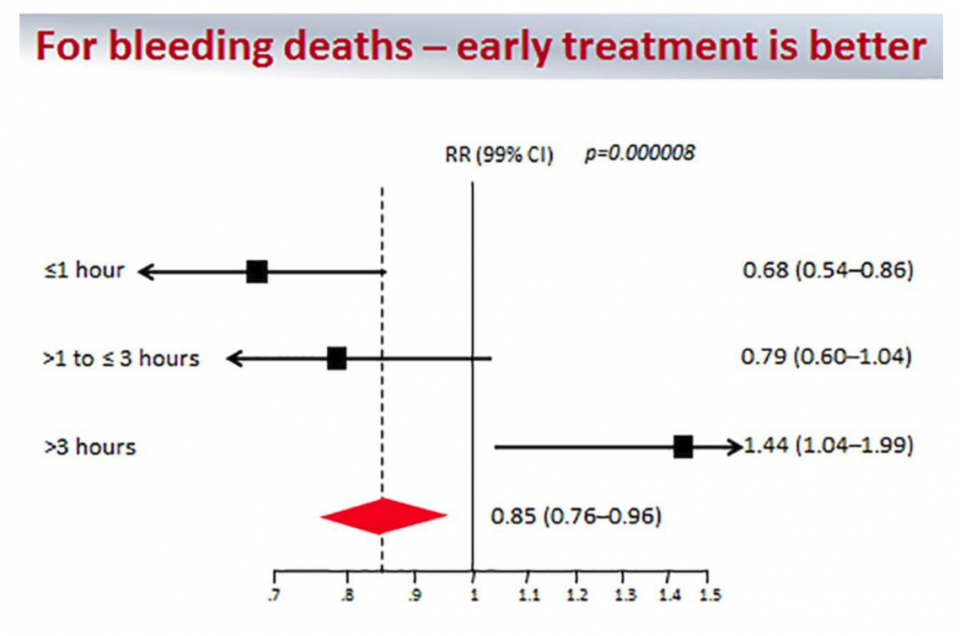
After CRASH-2 came the Exploratory Analysis of CRASH-2 which was a subgroup analysis looking at Early versus Late TXA
- The authors specifically examined the effect of TXA treatment on death caused by bleeding, rather than all-cause 28-day mortality
- Of the 3,076 deaths from all causes, 35% were caused by bleeding and the risk of death caused by bleeding was significantly reduced with TXA (4.9% vs. 5.7%; RR, 0.85)
- This subgroup analysis confirmed a significant reduction (19%) in deaths caused by bleeding in the most severe hemorrhagic shock patients who are hypotensive (with SBP of 75 mm Hg or less)
- The results from the CRASH-2 Subgroup analysis indicated that TXA should be given as early as possible to trauma patients who have bleeding. For trauma patients who received TXA > 3 hours after injury TXA was harmful.
The MATTERS study
The MATTERS study was published in 2012 by Morrison and colleagues. This was a retrospective observational study comparing TXA to no TXA in combat casualty patients. There were a total of 896 trauma patients; and 293 received TXA. Trauma patients were identified from UK and US trauma registries and all patients were treated in a surgical hospital in southern Afghanistan. The primary end points were 24 hour, 48 hour, and in-hospital mortality.
The results from the MATTERS study showed that the TXA group had lower unadjusted mortality than the non-TXA group despite being more severely injured. This benefit was greatest in Massive Transfusion patients, where TXA was also independently associated with improved survival and less coagulopathy (OR, 7.228). Thrombotic events were significantly increased in the TXA group for both PE and DVT in the overall cohort and in the Massive Transfusion cohort. However, after correcting for severity of injury, there was no association of TXA use with an increased risk of DVT or PE.
Bottom Line from the MATTERS study:
TXA should be implemented into clinical practice as part of a resuscitation strategy following severe wartime injury and hemorrhage
Lancet, Meta Analysis (2018)
A meta-analysis published in the Lancet in 2018 assessed anti-fibrinolytics in acute, severe bleeding. The investigators obtained data from more than 40,000 patients from two randomized trials of TXA in acute severe bleeding from trauma and PPH.
The primary measure of treatment benefit was absence of death from bleeding. Forty percent of patients had death from bleeding. Most (approximately 63%) occurred within 12 hours of onset and deaths from post-partum hemorrhage peaked 2–3 h after childbirth.
Overall the results showed that:
- TXA significantly increased overall survival in patients with bleeding (OR 1·20)
- Immediate treatment improved survival by more than 70% (OR 1·72)
- A delay in treatment reduced the treatment benefit
- After 3 hours TXA may be harmful
- Survival benefit decreased by 10% for every 15 min of treatment delay until 3 h, after which there was no benefit
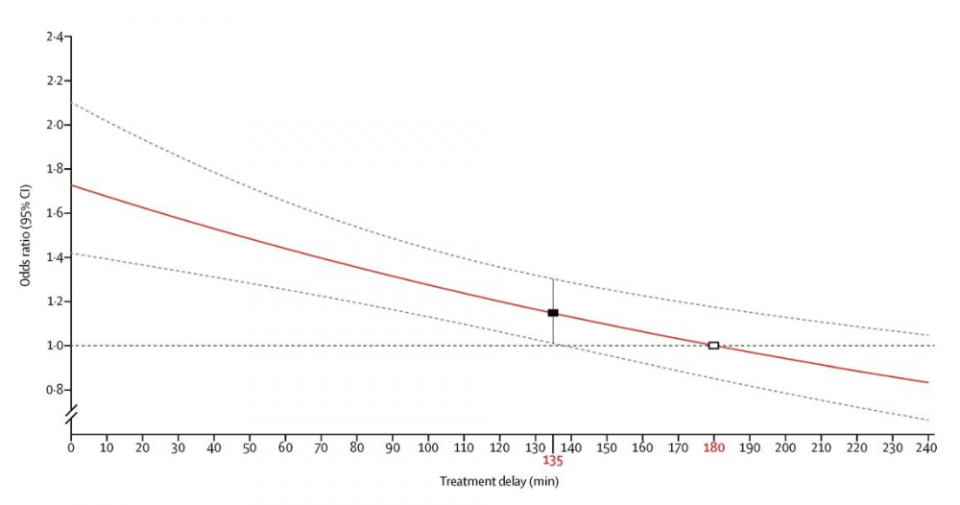
Figure: The red line shows the best fitted model for the association between the protective effect of TXA (odds ratio for not dying from bleeding) and the duration of treatment delay in minutes. The white square shows the timepoint at which the model estimates a null effect of tranexamic acid (a treatment delay of 180 min).
Ongoing Pre-Hospital Studies of TXA:
- STAAMP: Study of TXA during air medical pre-hospital transport: This multicenter trial is enrolling adult trauma patients being transported via air medical services from scene or referring hospital, with SBP <90 mm Hg or heart rate >110 bpm and within 2 hours of injury.
- PATCH (Pre-hospital Antifibrinolytics for Traumatic Coagulopathy & Haemorrhage) study: The PATCH-Trauma study is an international multicenter randomized, double-blind, placebo-controlled trial of pre-hospital TXA treatment for severely injured patients at risk of acute traumatic coagulopathy. The study aims to determine the effects of early TXA administration on survival and recovery of severely injured patients treated within advanced trauma systems in Australia and New Zealand.
- Pre-hospital TXA for TBI: An additional pre-hospital, multicenter, randomized, clinical trial aims to determine the efficacy of two pre-hospital TXA doses in moderate/severe TBI (GCS ≤12) compared to placebo.
Bottom Line for the use of TXA in Trauma
- TXA saves lives in trauma with a maximal benefit when given early.
- The frequency of thrombotic events among trauma patients who receive anti-fibrinolytic agents is not fully known from the clinical trials performed to date.
- In our setting, the use of TXA by paramedics would be especially useful for patients with long transport times to a trauma center such as those in rural areas
- TXA is not yet available to our land paramedics in Ontario but we can expect to see it soon. If approved by the MAC, it will initially only be available for use in Trauma
Ketamine for Excited Delirium
- Excited delirium is a syndrome characterized by delirium, agitation, and hyper-adrenergic autonomic dysfunction. This is a rare condition and the evidence for the use of ketamine in excited delirium is limited to small studies.
- Ketamine is an ideal agent for sedating these patients as it can be given intramuscularly, in a single dose and has an immediate effect.
- Ketamine exerts its actions through interactions with a variety of receptors including blockade of NMDA receptors, nitric oxide synthase inhibition, and interactions with multiple opioid receptors
- It is rapidly absorbed following IM, IV, or IO administration and is highly lipophilic. Onset of action is within minutes and generally lasts from 5–30 minutes
Evidence for use of Ketamine for Excited Delirium in a pre-hospital setting:
- Olives et al. Prehosp Disaster Med. (2016)
- Evaluated the incidence of intubation in patients with clinically significant profound agitation and characterized findings from patients who required intubation
- Patients received 5 mg/kg of IM Ketamine OR 2 mg/kg of IV or IO Ketamine via a prehospital ketamine protocol
- Only 4 pts required intubation in the field, others who required intubation were intubated in the ED (85% of patients)
- Factors associated with ED intubation including night-time arrivals or male gender whereas the dose of ketamine and co-ingestants were not associated with intubation
- Scheppke et al. West J Emerg Med (2014)
- A case series of 52 patients who received IM ketamine for sedation
- Patients received 4 mg/kg of IM Ketamine +/- Midazolam
- The average time to sedation in the ketamine group was 2 minutes
- Average time to ED arrival was 19 minutes and 50 out of 52 patients were adequately sedated on ED arrival
- About half of the patients received midazolam in addition to ketamine
- 3 cases of respiratory depression occurred with 2 patients requiring intubation in the midazolam group
- Burnett AM, et al. Prehosp Emerg Care (2012)
- A Quality Improvement study of 13 patients which found that Ketamine had a quick onset of action (2 mins) and produced moderate to deep sedation in patients receiving IM ketamine 5 mg/kg
- Scaggs et al. Prehospital Emerg Med (2016)
- Published Case Reports demonstrated the safety of ketamine when compared to Midazolam in the pre-hospital setting for the treatment of Excited Delirium.
- Cole et al., Amer J Emerg Med (2017)
- Conducted a prospective observational study of patients receiving 5 mg/kg of IM Ketamine for profound agitation
- Assessed the effectiveness of ketamine as a primary therapy for pre-hospital profound agitation
- 90% of patients had adequate sedation in the pre-hospital setting
- Median time to adequate sedation was 4 minutes and 57% patients were intubated
Bottom Line:
- There is a role for Ketamine in the treatment of pre-hospital excited delirium.
- Ketamine has been approved for use in Excited Delirium and will be available to Ontario Paramedics for this indication by the fall of 2018.
New Ottawa ROSC bypass protocol
- According to the 2015 American Heart Association (AHA) guidelines, coronary angiography is recommended in patients with OHCA with a suspected cardiac cause and STEMI on ECG (class of recommendation I, level of evidence B), and it should be considered in patients after cardiac arrest who present without STE but with a suspected cardiac cause of cardiac arrest (class of recommendation IIa, level of evidence B)
- Please refer to Dr. Simeon Mitchell’s Grand Rounds Summary for more information
- The 2015 ILCOR systematic review addressed whether transport of OHCA patients by EMS directly to a specialist cardiac arrest center improves outcomes
- These studies, reporting on more than 120, 000 patients surviving to hospital discharge, suggest that there is an association with improved survival when patients are transported to specialist cardiac arrest centers
- As per the 2015 ILCOR guidelines: A regionalized approach to OHCA resuscitation that includes the use of cardiac resuscitation centers may be considered (Class IIb, LOE C-LD)
- The ARREST trial was recently published in Resuscitation: Findings from this trial support the feasibility and acceptability of conducting a large-scale randomized controlled trial of expedited transfer to cardiac arrest centers following OHCA
- Early Coronary Angiography and Survival After Out-of-Hospital Cardiac Arrest: Vyas and colleagues used data from the CARES database (Cardiac Arrest Registry to Enhance Survival) and identified adult patients who were admitted to hospitals after successful resuscitation from an OHCA. Results showed that among initial survivors of OHCA with an initial shockable rhythm, they found early coronary angiography was associated with higher odds of survival to discharge and a favorable neurological outcome
- A Danish Study published in 2017 found that immediate admission to an invasive heart center and acute CAG/PCI were associated with improved (30-day) survival in patients with OHCA, whereas distance from site of the event to the invasive heart center was not. Other factors associated with improved survival included bystander CPR, witnessed arrest, and an initial shockable rhythm
- Patel and colleagues in JAMA Cardiology (2016):
- The purpose of this study was to determine if bypassing hospitals without PCI capability, in favor of a PCI-capable center, improves outcomes in patients with out-of-hospital cardiac arrest
- The majority of patients (90.2%), were transported to PCI-capable centers; the emergency responders bypassed non-PCI hospitals in 57.9% of these cases (873 patients). Only 9.8% were transported to non-PCI hospitals
- Patients transported to PCI-capable centers had higher rates of survival to hospital discharge than patients transported to non-PCI centers (33.5% for PCI vs 14.6% for non-PCI). This effect was consistent for short, medium, and long transport times.
- This study provides evidence to support the theory that patients experiencing an out-of-hospital cardiac arrest have better outcomes when transported to a PCI-capable hospital, even if this means bypassing non–PCI capable facilities.
Bottom Line:
There is good evidence to suggest that transporting OHCA patients by EMS directly to a specialist cardiac arrest center is associated with improved outcomes. The Ottawa ROSC bypass protocol (presented below) goes into effect on May 16, 2018.
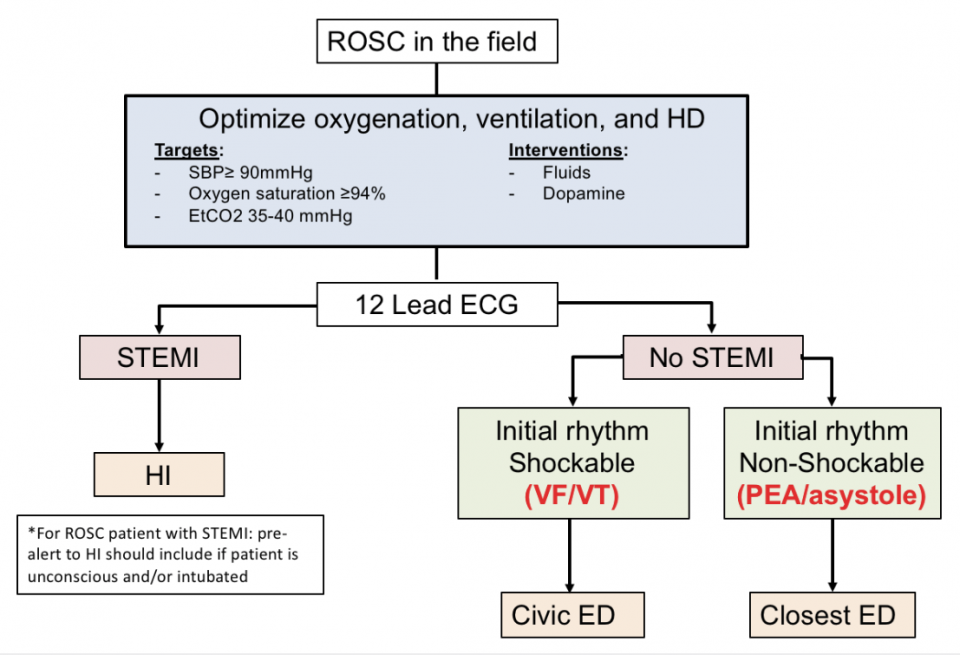
Exclusions to the ROSC bypass include
- Age < 18 yrs
- Expected transport time > 30 mins
- ABCs are not optimized
- Traumatic arrest
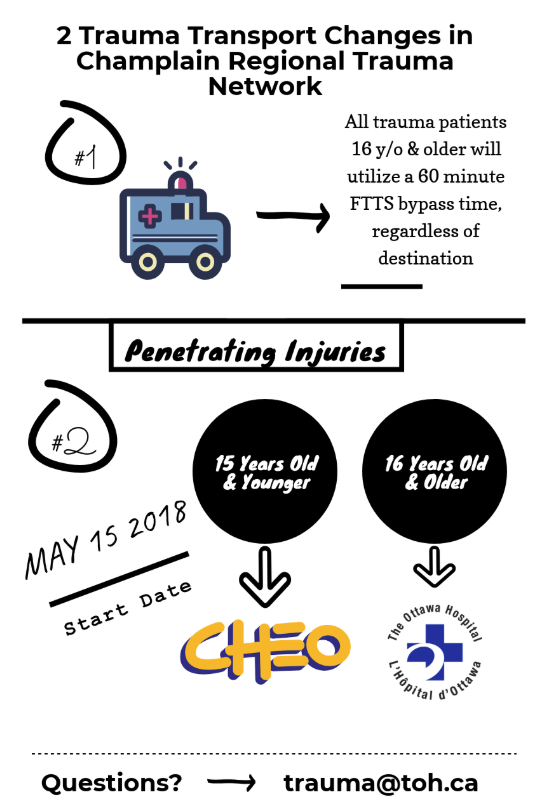
New Ottawa Pediatric Trauma bypass protocol
- The new Ottawa pediatric trauma bypass protocol goes into effect on May 15, 2018.
- The adult hospitals in our region have more experience with ED thoracotomy which these patients may require. Taking these factors into consideration, new changes were made to the trauma bypass protocol. We hope that these new changes will improve patient outcomes.
Paramedics’ Scope of Practice in Obstetric Emergencies
- In the fall of 2017, all paramedics in Ontario received Out Of Hospital (OOH) emergency childbirth skills training
- This training session included a didactic portion followed by observed simulated scenarios
- This is a brief overview of the paramedic’s scope of practice in managing OOH childbirth emergencies.
- All Ontario paramedics carry a basic obstetrics kit in their ambulance which includes: PPE (gloves and gown), cord clamps, extra blankets, NRP equipment
Precipitous Birth
- Typically, the paramedics will load & go after the birth of the baby and avoid delaying transport
- However, as per the new ALS medical directive, if signs of placental separation occur then paramedics will deliver the placenta before transporting the patient to the hospital
Immediate Post-Partum Care
- Paramedics have received training in how to care for the birthing patient and the newborn baby as per the 2017 NRP guidelines
Care of the Birthing patient
- Massage the uterus (external massage) to help minimize bleeding
- Check the fundus and monitor vaginal bleeding every 5 minutes for the first 15 minutes
- Monitor patient vitals
- Encourage the patient to void (empty bladder) prior to transport
Shoulder Dystocia
- Shoulder dystocia is an intrapartum complication that can have serious risks to the baby and the mother
- Paramedics in Ontario are trained to perform different maneuvers for shoulder dystocia
- This means that if the paramedics bring a patient to the Emergency Department, know that they have already spent some time on scene and tried different maneuvers. Call for help and call Obstetrics ASAP
Breech Presentations
- If known breech and birth is not imminent→ transport to the hospital immediately as per BLS Load and Go Standard
- New ALS Medical Directive: If the head of the baby does not deliver within 3 minutes of the birth of the umbilicus, the paramedics may attempt Mauriceau Smellie Veit Maneuver
- The birthing patient is at an increased risk of post-partum hemorrhage after a breech delivery
Twin Deliveries
- Paramedics can assist in normal, uncomplicated twin deliveries
- There can be a 20 to 30 minute delay before the birth of the second baby
- BLS Load and Go urgent transport depends on the distance to the hospital and if delivery of the 2nd twin is imminent
- If placenta(e) deliver prior to Load and Go, paramedics may perform external uterine massage after the delivery of placenta to encourage contractions and minimize bleeding
- The birthing patient is at an increased risk of post-partum hemorrhage after a twin delivery
Cord Prolapse
- Cord prolapse occurs in 0.1% to 0.6% of all births and the risk is higher with breech presentations
- Cord prolapse → Load and Go → C-section
- If birth is imminent, then the goal is to birth the baby within 4 mins due to cord compression
- As per the new ALS Medical Directive for Cord Prolapse:
- The paramedics may obtain consent and manually elevate the presenting fetal part up and off the cord
- The paramedics are not allowed or trained to do any internal exams
- When this patient presents to the ED, we cannot assume that there is no internal cord prolapse
Post Partum Hemorrhage (PPH)
- PPH is defined as more than 500 mL of blood loss after a spontaneous vaginal delivery (SVD) and more than 1 L after a C-Section
- Primary PPH: within 24 hours of birth
- Secondary PPH: occurs from 24 hours to 6 weeks post-partum
- Occurs in <6% of all births
- Major cause of morbidity and mortality
- Paramedic Management of PPH:
- The paramedics are not allowed to do bimanual compression of the uterus
- They do not carry oxytocin or Tranexamic acid (TXA)
- As per the new ALS Medical Directive: external uterine massage and external bimanual compression may be performed once the placenta has been delivered
- These skills will reduce blood loss and associated complications of PPH
References
- Burnett AM, Salzman JG, Griffith KR, Kroeger B, Frascone RJ. The emergency department experience with prehospital ketamine: a case series of 13 patients. Prehosp Emerg Care. 2012 Oct-Dec;16(4):553-9.
- Cole JB, Klein LR, Nystrom PC, Moore JC, Driver BE, Fryza BJ, Harrington J, Ho JD. A prospective study of ketamine as primary therapy for prehospital profound agitation. Am J Emerg Med. 2018 May;36(5):789-796.
- Gayet-Ageron A, Prieto-Merino D, Ker K, Shakur H, Ageron FX, Roberts I; Antifibrinolytic Trials Collaboration. Effect of treatment delay on the effectiveness and safety of antifibrinolytics in acute severe haemorrhage: a meta-analysis of individual patient-level data from 40 138 bleeding patients. Lancet. 2018 Jan 13;391(10116):125-132.
- Lee TR, Hwang SY, Cha WC, Shin TG, Sim MS, Jo IJ, Song KJ, Rhee JE, Jeong YK. Role of coronary angiography for out-of-hospital cardiac arrest survivors according to postreturn of spontaneous circulation on an electrocardiogram. Medicine (Baltimore). 2017 Feb;96(7):e6123.
- Linder LM, Ross CA, Weant KA. Ketamine for the Acute Management of Excited Delirium and Agitation in the Prehospital Setting. Pharmacotherapy. 2018 Jan;38(1):139-151.
- Mannucci PM, Levi M. Prevention and treatment of major blood loss. N Engl J Med. 2007 May 31;356(22):2301-11.
- Morrison JJ, Dubose JJ, Rasmussen TE, Midwinter MJ. Military Application of Tranexamic Acid in Trauma Emergency Resuscitation (MATTERs) Study. Arch Surg. 2012 Feb;147(2):113-9.
- Napolitano LM. Prehospital tranexamic acid: what is the current evidence? Trauma Surg Acute Care Open. 2017 Jan 13;2(1):e000056.
- Olives TD, Nystrom PC, Cole JB, Dodd KW, Ho JD. Intubation of Profoundly Agitated Patients Treated with Prehospital Ketamine. Prehosp Disaster Med. 2016 Dec;31(6):593-602.
- Patel N, Patel NJ, Macon CJ, Thakkar B, Desai M, Rengifo-Moreno P, Alfonso CE, Myerburg RJ, Bhatt DL, Cohen MG. Trends and Outcomes of Coronary Angiography and Percutaneous Coronary Intervention After Out-of-Hospital Cardiac Arrest Associated With Ventricular Fibrillation or Pulseless Ventricular Tachycardia. JAMA Cardiol. 2016 Nov 1;1(8):890-899.
- Patterson T, Perkins GD, Joseph J, Wilson K, Van Dyck L, Robertson S, Nguyen H, McConkey H, Whitbread M, Fothergill R, Nevett J, Dalby M, Rakhit R, MacCarthy P, Perera D, Nolan JP, Redwood SR. A Randomised tRial of Expedited transfer to a cardiac arrest centre for non-ST elevation ventricular fibrillation out-of-hospital cardiac arrest: The ARREST pilot randomised trial. Resuscitation. 2017 Jun;115:185-191.
- Roberts I, Shakur H, Afolabi A, Brohi K, Coats T, Dewan Y, Gando S, Guyatt G, Hunt BJ, Morales C, Perel P, Prieto-Merino D, Woolley T. The importance of early treatment with tranexamic acid in bleeding trauma patients: an exploratory analysis of the CRASH-2 randomised controlled trial. Lancet. 2011 Mar 26;377(9771):1096-101, 1101.e1-2.
- Roberts I, Shakur H, Ker K, Coats T; CRASH-2 Trial collaborators. Antifibrinolytic drugs for acute traumatic injury. Cochrane Database Syst Rev. 2012;12:CD004896.
- Scaggs TR, Glass DM, Hutchcraft MG, Weir WB. Prehospital Ketamine is a Safe and Effective Treatment for Excited Delirium in a Community Hospital Based EMS System. Prehosp Disaster Med. 2016 Oct;31(5):563-9.
- Scheppke KA, Braghiroli J, Shalaby M, Chait R. Prehospital use of i.m. ketamine for sedation of violent and agitated patients. West J Emerg Med. 2014 Nov;15(7):736-41.
- Shakur H, Roberts I, Bautista R, Caballero J, Coats T, Dewan Y, El-Sayed H, Gogichaishvili T, Gupta S, Herrera J, Hunt B, Iribhogbe P, Izurieta M, Khamis H, Komolafe E, Marrero MA, Mejía-Mantilla J, Miranda J, Morales C, Olaomi O, Olldashi F, Perel P, Peto R, Ramana PV, Ravi RR, Yutthakasemsunt S. Effects of tranexamic acid on death, vascular occlusive events, and blood transfusion in trauma patients with significant haemorrhage (CRASH-2): a randomised, placebo-controlled trial. Lancet. 2010 Jul 3;376(9734):23-32.
- Tranberg T, Lippert FK, Christensen EF, Stengaard C, Hjort J, Lassen JF, Petersen F, Jensen JS, Bäck C, Jensen LO, Ravkilde J, Bøtker HE, Terkelsen CJ. Distance to invasive heart centre, performance of acute coronary angiography, and angioplasty and associated outcome in out-of-hospital cardiac arrest: a nationwide study. Eur Heart J. 2017 Jun 1;38(21):1645-1652.
- Vyas A, Chan PS, Cram P, Nallamothu BK, McNally B, Girotra S. Early Coronary Angiography and Survival After Out-of-Hospital Cardiac Arrest. Circ Cardiovasc Interv. 2015 Oct;8(10).

