
Most clinicians are familiar with and utilize the Glasgow Coma Scale (GCS) on a daily basis, but many are not aware of the updates and additions to the score that were made in 2014 and 2018, respectively. Clarifications in the wording of the scale attempt to increase the ease of use and inter-rater reliability, while the addition of pupil examination and CT findings seek to increase prognostic accuracy. This post highlights these updates and the data supporting them.
The GCS, developed by Prof. Graham Teasdale in 1974, was designed to quantify level of consciousness in the brain injured patient1. Since its inception it has evolved from a 14-point scale to the modern 15-point scale and has become an integral part of the assessment of and prognostication for altered mental status patients across the world2. It was adopted in the 1st edition of ATLS in 19803 and continues to be included in its more modern form in the 10th edition of ATLS.
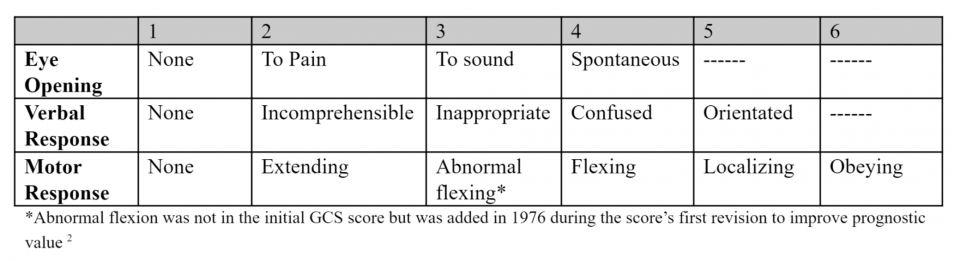
The original components of the GCS were as follows:
Glasgow Coma Scale 1974
Clarification of Terminology
This edition of the GCS scale is the one that most people are aware of. However, on the 40th anniversary of the scale, it underwent an update to terminology with the goal to simplify the language used2. That version of the GCS is as follows (changes are highlighted).
Glasgow Coma Scale 2014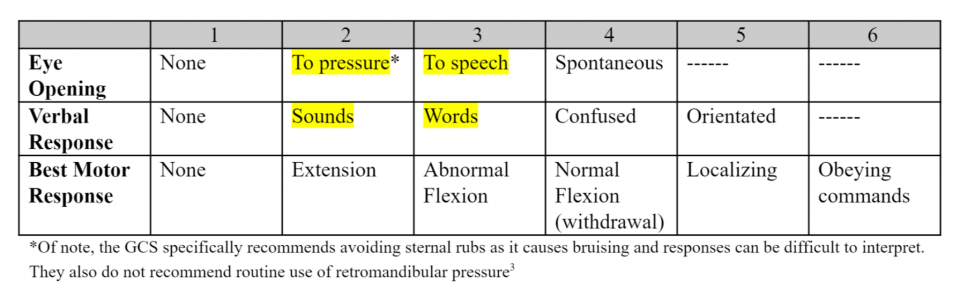
Reporting of Non-testable Score Aspects
In the new 2014 version, scores are tabulated as previous with a combined score from 3 to 15 and individual scores. However, in the case of a non-testable aspect, the new GCS should only be noted in its components. Here is an example:
42 year old man, intubated after traumatic brain injury (TBI) for decreasing GCS. Currently, he opens his eyes to pressure, is intubated, and withdraws his left arm and leg to pain.
1979 – GCS: E 2, V 1t, M 4. Combined GCS: 7t
2014 – GCS: E 2, V NT, M 4. It is no longer recommend to assign 1 point to non-testable elements, therefore a combined score should not be used here as it would imply that the patient is more unwell than they really are. Any element that cannot be tested should be marked as NT, for “not testable”4.
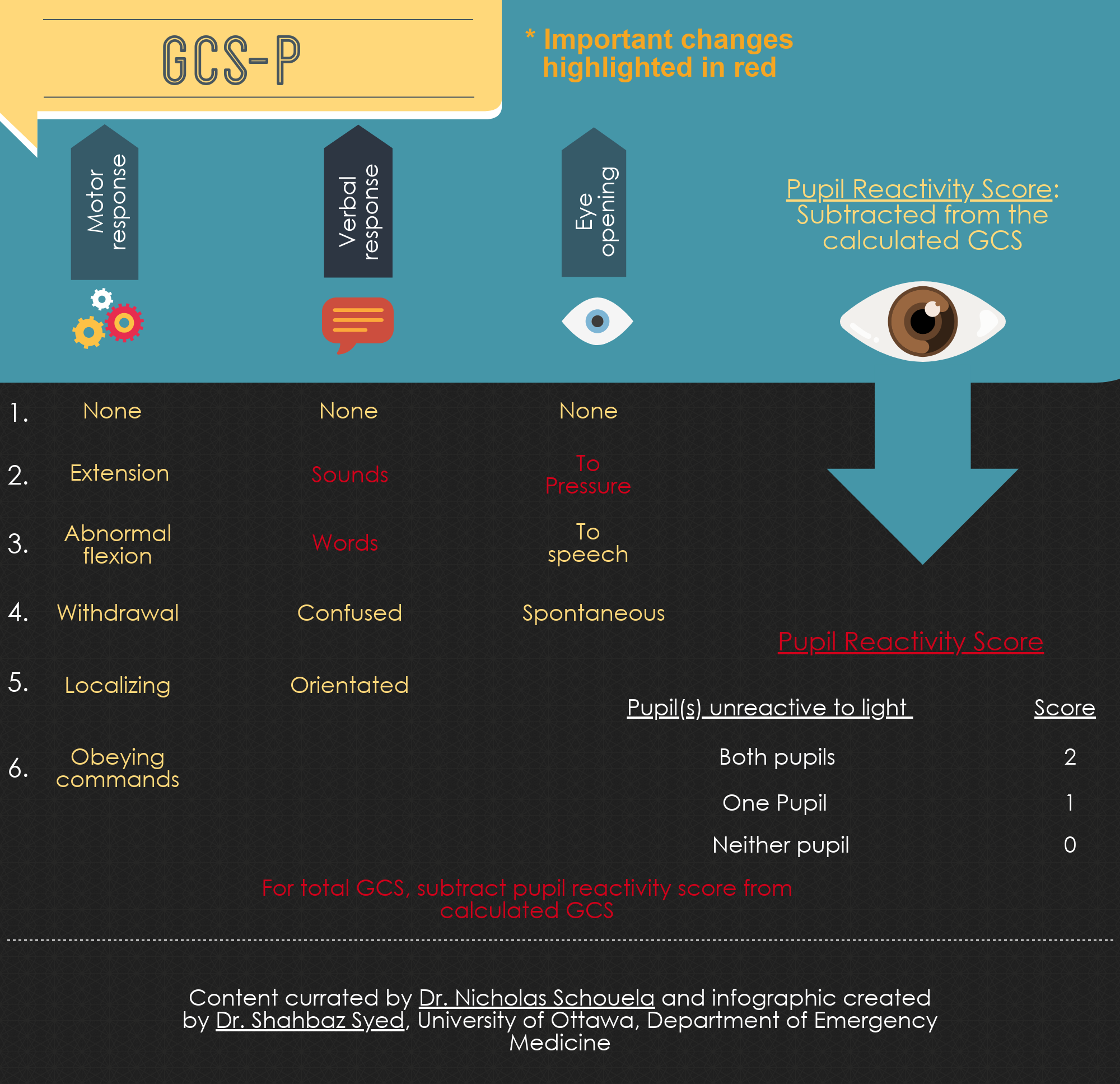
Adoption of the Pupil Reactivity Score (GCS-P)
Prof. Teasdale was not finished however. The ability to prognosticate based on initial presentation is important for both downstream management of the injured patient as well as to help guide goals of care discussions. As a result, this year a new paper was published calling for the adoption of the GCS-P score. The GCS-P is scored from 1 to 15 and is calculated by subtracting a pupil reactivity score (PRS) from the calculated GCS.
Pupil Reactivity Score

Here is a case example:
37 year old female with a traumatic subarachnoid hemorrhage (SAH). On presentation to the ED, she does not open her eyes, she moans, and displays abnormal flexion in her limbs to pain. On examination of her pupils they are both fixed and dilated.
Her GCS is 6. Her GCS-P is 6-2 = 4.
According to pooled data from CRASH and IMPACT trials used to derive the score, a GCS of 6 carries a 6-month mortality of 28.82%. However, patients with a GCS of 6 and bilateral fixed pupils (GCS-P = 4) have a 6-month mortality of 42.94%5. The addition of a pupil examination appears to allow clinicians to prognosticate outcomes better than GCS alone and can be done quickly and easily at the bedside.
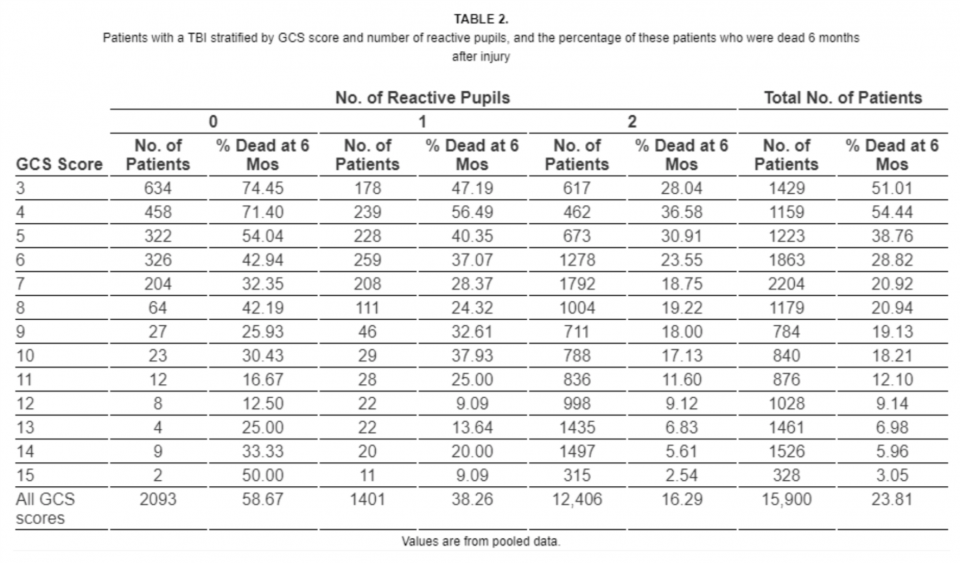
Mortality vs GCS score stratified by pupil reactivity using CRASH and IMPACT data5
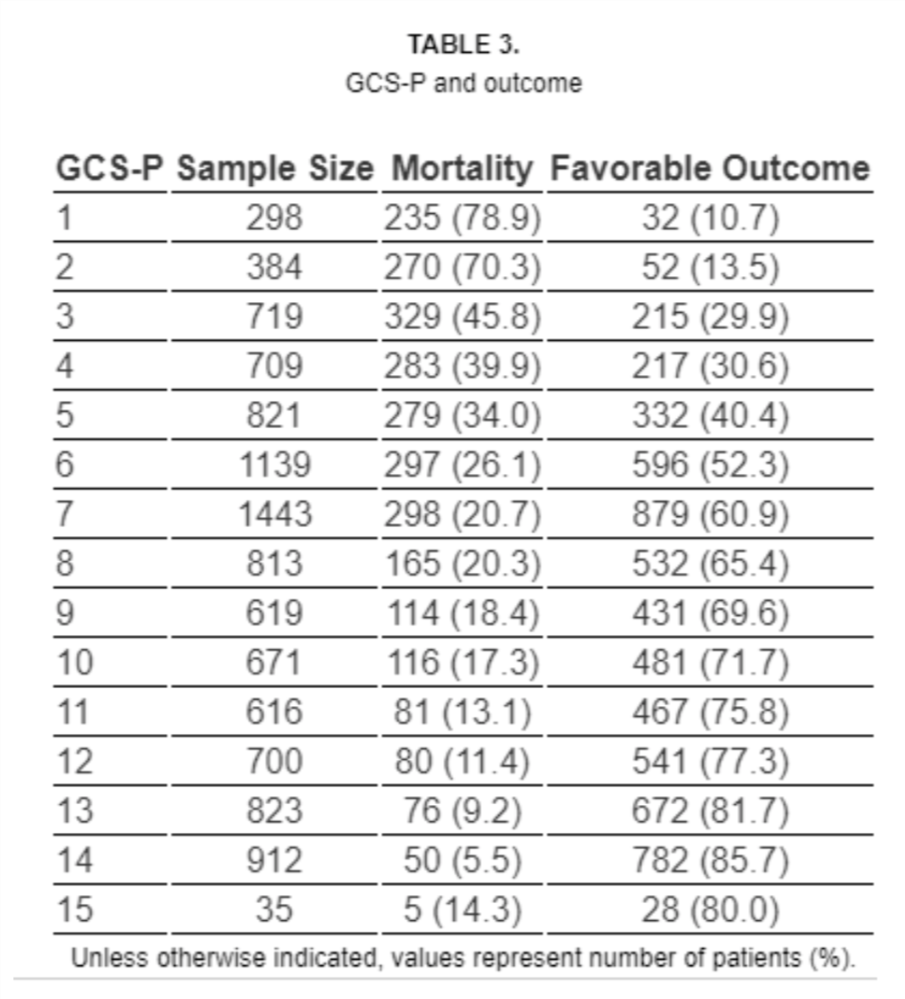
Table of calculated GCS-P score and corresponding mortality and outcomes6
The study authors took this one step further by combining the most predictive factors for mortality and unfavorable outcomes in TBI. They incorporated age and CT findings with GCS-P and created GCS-PA CT (GCS, pupils, age, and CT findings).5 While potentially useful from a prognostic standpoint, this is not as easily applied at the bedside and requires a chart to interpret. Due to ease of use, the GCS-P appears more likely to be readily adopted than the more cumbersome GCS-PA CT.
GCS-PA CT prediction charts
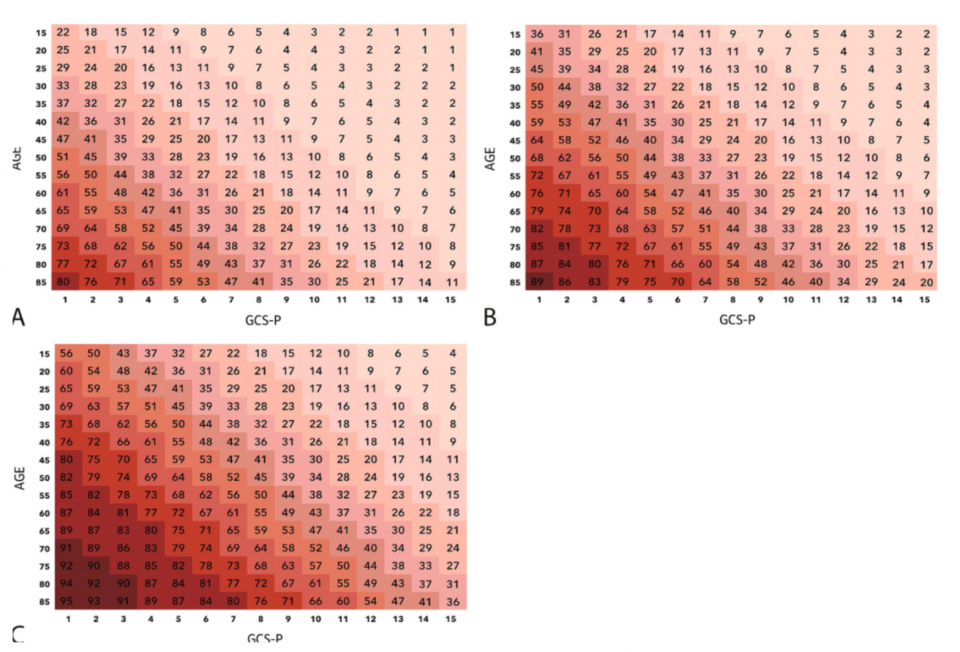
Probability of mortality 6 months after head injury based on the patient’s admission GCS-P and age with no CT abnormality (A), exactly 1 CT abnormality (B), and 2 or more CT abnormalities (C). Potential CT abnormalities include intracranial hematoma, absent cisterns, and SAH.6
Summary
- GCS score has evolved over the last 44 years and now includes new terminology and an expanded GCS-P score
- Sternal rub and retromandiublar pressure are NOT recommended
- Do not include a combined score when one of the elements of the scale is non-testable
- While the GCS-P should not be used as the sole decision instrument in TBI, it appears to be a useful tool in our decision-making arsenal when combined with clinical judgment
- GCS may be even more predictive if you incorporate patient age and CT findings (GCS-PA CT)
References
- Teasdale G, Jennett B. Assessment of coma and impaired consciousness. A practical scale. Lancet 1974;2:81-4.
- Teasdale G, et al. The Glasgow Coma Scale at 40 years: standing the test of time. The Lancet Neurology , 2014;13(8):844–54
- The Glasgow Structured Approach to Assessment of the Glasgow Coma Scale. Retrieved from http://www.glasgowcomascale.org/
- Meredith W, Rutledge R, Fakhry SM et al. The conundrum of the Glasgow Coma Scale in intubated patients: a linear regression prediction of the Glasgow verbal score from the Glasgow eye and motor scores. J Trauma. 1998; 44:839-45.
- Brennan P, Murray G, Teasdale G. Simplifying the use of prognostic information in traumatic brain injury. Part 1: The GCS-Pupils score: an extended index of clinical severity. J Neurosurgery, 2018;128(6):1612-20
- Murray G, Brennan P, Teasdale G. Simplifying the use of prognostic information in traumatic brain injury. Part 2: Graphical presentation of probabilities. J Neurosurgery, 2018;128(6):1621-34


Thanks for this! It was both informative and fascinating. I came for the former, stayed for the latter. I’m recommending this blogpost to my students and juniors.
Thank you for the insightful updates on the Glasgow Coma Scale! It’s fascinating to see how these revisions can enhance our assessment and understanding of patient conditions. I’m looking forward to applying some of these concepts in practice.
Thanks for the excellent review.
I have couple of questions: (probably hypothetical)
1. in case the patient is having hemiplegia how would you GSC him/her?
2. in case the patient shows different response i.e. Withdrawal on one side and extension on the other side, which one would you consider?
Best
Thank you for the insightful update on the Glasgow Coma Scale! The changes and enhancements you’ve outlined are crucial for improving patient assessment. I appreciate how this adaptation can lead to better outcomes in emergency care. Looking forward to seeing how these updates are implemented in clinical settings!
Really appreciate the clear updates on the Glasgow Coma Scale! It’s impressive how these changes can improve how we evaluate patient responses. Can’t wait to put some of this new knowledge into action.
Great insights on the updates to the Glasgow Coma Scale! It’s fascinating to see how evolving practices can improve patient assessment. Looking forward to seeing how these changes will impact clinical outcomes!
Great insights on the updates to the GCS! It’s fascinating to see how even small changes can impact clinical assessment and patient outcomes. Looking forward to seeing how these updates will be integrated into practice!