

Head injuries are commonly seen in the emergency department and a large group of these patients will subsequently be diagnosed with a concussion. In this three-part series, we will summarize the most up to date definition of a concussion (Part 1), review how to make the diagnosis and provide concussion counseling to your patients (Part 2), discuss the complications of concussions and why proper concussion care is a public health concern (Part 3).
Part 1: What is a Concussion?
The definition of a concussion varies slightly depending on what source you use; however, there are a few key components that are consistent in all sources for both adult and pediatric patients.1–3 Focusing on these features, a concussion:
- Is a form of mild traumatic brain injury (mTBI)
- Occurs when biomechanical forces are transmitted to the brain and disrupt normal neurophysiology
- Presents as a short-lived, spontaneously resolving neurological impairment
- Creates a functional impairment rather than a structural injury that can not be seen on conventional imaging
- Generates an objective pattern of clinical and cognitive symptoms that typically follow a sequential recovery
Traumatic Brain Injury (TBI)
TBI’s are a group of brain disorders that occur after traumatic injury and are classified in various ways with the most commonly used system being categorization by severity.1 TBI severity is defined by the patient’s Glasgow Coma Scale (GCS) at assessment or within 30 minutes of injury, which was originally described in 1974.4 An important concept to remember is that although all concussions are mild TBIs, not all mild TBIs are concussions, and they can be distinguished by an inconsistent history, imaging findings, or persistent neurological deficits.1
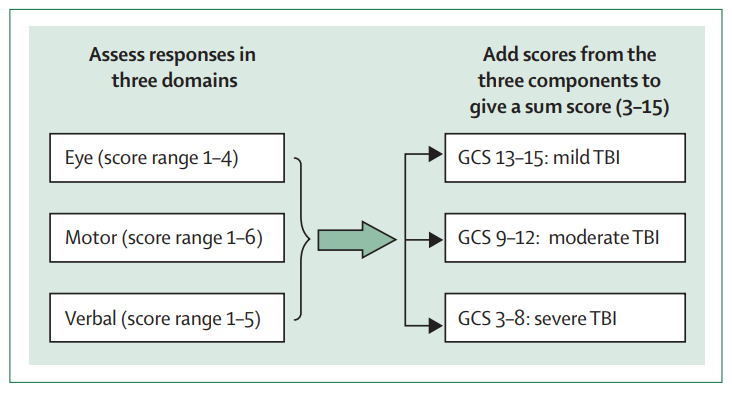 Figure from Maas et al5
Figure from Maas et al5
Biomechanical Forces
Blunt trauma creates mechanical energy, and if it is applied to the head, neck, or body, it can transmit forces to the brain, resulting in a concussion. Thus, you do not need to be hit in the head to get a concussion.2,6 Although there are both linear and rotational force components, it is the rotation that is most highly correlated with injury.6–8 It is important to realize that it doesn’t have to be a hard straight-on hit; if there is a significant rotation with lower forces, you can still get a concussion.
One myth that is often described is that the “brain bounces around in skull” and the contact between the brain and skull creates a concussion.9,10 However, this is not what concussion experts believe. Firstly, if the brain bounces around in the skull, we would see coup-contrecoup injuries on conventional imaging, which contradicts the definition of a concussion.2 Secondly, the brain is surrounded by cerebrospinal fluid which acts as a shock absorber and cushion that limits contact. Finally, the brain has fixed points – Falx Cerebri and Tentorium Cerebelli, which limit movement. The newest data demonstrates that these fixations create “local areas of deformation,” which distributes these forces centrally.7,11 If you think about it, this makes sense because to lose consciousness or become amnestic, you need to injure your brainstem or reticular activating system (RAS), which is located centrally.
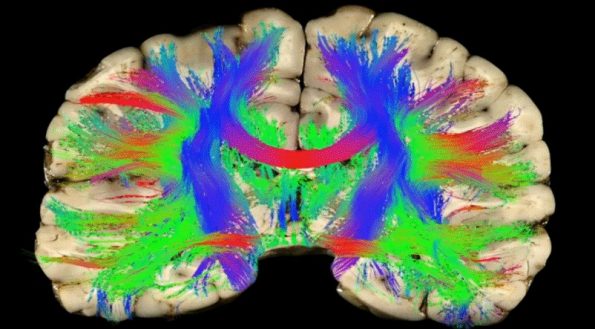 **Red represent areas of increased force and injury. Image is taken from Dr. D. Camarillo’s TedTalk at https://www.ted.com/talks/david_camarillo_why_helmets_don_t_prevent_concussions_and_what_might
**Red represent areas of increased force and injury. Image is taken from Dr. D. Camarillo’s TedTalk at https://www.ted.com/talks/david_camarillo_why_helmets_don_t_prevent_concussions_and_what_might
Neurophysiology Alterations
A concussion instantly creates multiple changes in neurochemistry, which are more complex than what the average emergency physician needs to know. However, one component that is beneficial to understand is that concussions immediately create what experts call an “energy crisis.”12,13 The brain immediately releases its glucose stores, but its ability to uptake glucose gets depressed. Furthermore, cerebral blood flow is immediately decreased and remains that way for days or even weeks after the initial injury.12,13
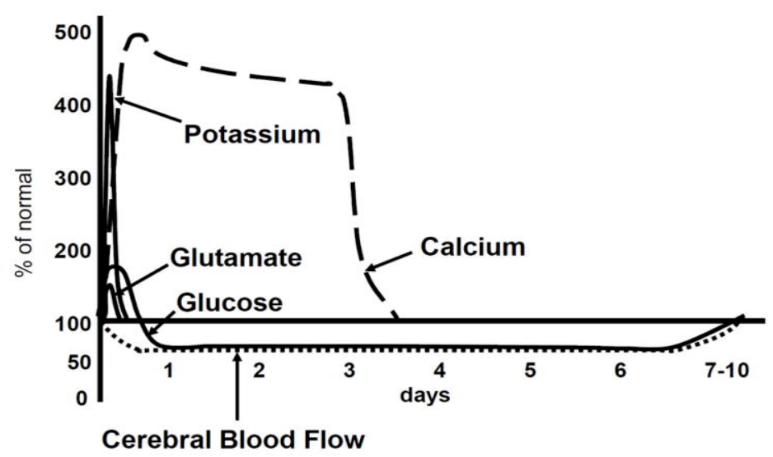 Figure is from Giza et all13
Figure is from Giza et all13
This is important to understand because your brain is about 2% of your body mass but uses 20% of your energy.14 You’ve got an impaired ability to use glucose for energy, and the brain is physically getting less blood flow to it, thus it has no choice but to operate at lower functional capacity for the first few days after a concussion.
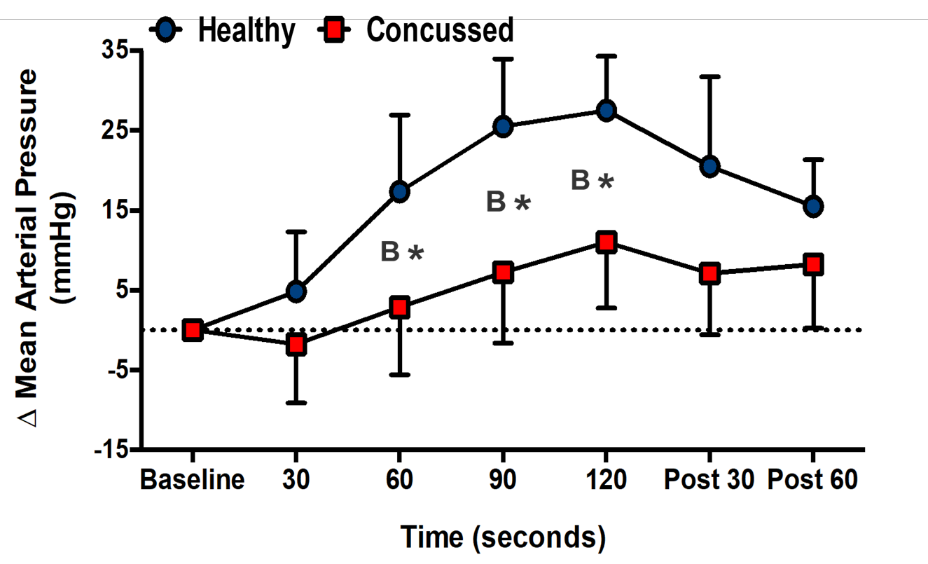 Johnson BD, Sackett JR, Schlader ZJ, & Leddy JJ. Attenuated cardiovascular responses to sympathoexcitation in recently concussed college athletes. Journal of Athletic Training, in press.
Johnson BD, Sackett JR, Schlader ZJ, & Leddy JJ. Attenuated cardiovascular responses to sympathoexcitation in recently concussed college athletes. Journal of Athletic Training, in press.
Another neurophysiological issue after a concussion is autonomic dysregulation, where concussed patients lose the ability to appropriately switch between “fight or flight” and “rest and digest.” This was demonstrated by Johnson et al., where we see significantly depressing responses from concussed patients when exposed to a stressful stimulus compared to controls.15 The autonomic dysregulation presents as exercise intolerance because when their body is stressed, it cannot appropriately compensate and may over or undershoot its normal response.
Short-lived Neurological Impairment that Resolves Spontaneously
Regarding concussions, a brief neurological impairment is one of the following:2,3,16,17
- Loss of consciousness for up to 30 minutes
- Post-traumatic amnesia before or after the accident for as much as 24 hours; or
- Alteration of mental state at the time of the injury
The last criteria is the most vague part of the definition, and varies depending on the source but includes feeling off or in a fog, being disoriented, or confusion. It is important to understand that these symptoms must be present at the time of injury and may be completely resolved by the time you see the patient. If the time intervals are longer than those listed above, then they have a mild TBI and not a concussion.
Functional Disturbance Rather than Structural Injury
Concussions lack evidence of an intracranial or structural injury on standard imaging tests. However, there is evidence of microstructural injuries on axons, which lead to functional issues within the brain we can see on functional MRI (fMRI).13 There have been three studies that compared concussed varsity athletes to controls using a combination of neurocognitive testing and fMRI.18–20 They all found that fMRI changes persisted even when the athletes did not show any physical or neurocognitive signs of injury on standardized testing and were cleared for return to sport. A concussion expert stated that this disruption of neuro-connections necessitates a re-learning process and that a concussed brain has to re-learn how to do things that were once straight forward.
Pattern of Clinical and Cognitive Symptoms
The final key component of defining concussions is that they have a pattern of clinical and cognitive symptoms that typically follow a sequential recovery. These symptoms and features are organized into four categories:1,2,16,21
- Physical or somatic symptoms
- Headache, nausea, dizziness, sensitivity to light or noise, or visual disturbances
- Cognitive symptoms
- Feeling like they’re in a fog, difficulty concentrating or remembering, or answering questions slowly
- Emotional/behavioral symptoms
- Irritable, sad, anxious, or emotional lability
- Sleep disturbance
- Fatigue, drowsiness, or insomnia
The most common symptoms are headache, dizziness, and fatigue. Of note, in some patients, it can take up to 24 hours for symptoms to evolve or even present.
Concussions heal in a typical way, which differs slightly in adults and children. For children, since the brain is still developing, it takes longer to recover because it needs to both heal and catch up. In adults with their first concussion, 85–90% will resolve within 14 days.2,16,22 Athletes tend to recover quicker than the general population, in approximately 10 days.23 In pediatrics, we used to think they had the same timeline, but a large prospective Canadian study has changed that.24 They followed over 3000 children for several months, reviewing their symptom scoring and plotting their recoveries over time. They found that preadolescent children (age < 8) were similar to adults, with an average of 2 weeks for symptom recovery. In adolescents (age 8-12) and teenage males, average symptom recovery can take up to 4 weeks; however, in female adolescents (age 13-18), their typical recovery can last for several weeks (~8 weeks).
Take Home Points
A Concussion:
- Is an mTBI created by biomechanical forces that disrupt normal neurophysiology
- Any force that is transmitted to the brain can cause a concussion
- The brain is physiologically stunned immediately and for several days after injury
- Presents with a spontaneously resolving, rapid onset neurological impairment
- Creates a functional rather than a structural injury with no evidence on standard imaging tests
- Has a typical pattern of clinical and cognitive symptoms that follow a sequential recovery
- For adults and children under 8 years old, 85-90% will recover in 2 weeks
- For children 8-12 years old and male teenagers, recovery typically takes 4 weeks
- For female teenagers, recovery is longer, typically > 4 weeks
References
- Marshall, S. Guideline for Concussion / Mild Traumatic Brain Injury & Persistent Symptoms.
- McCrory, P. et al. Consensus statement on concussion in sport—the 5 th international conference on concussion in sport held in Berlin, October 2016. Br. J. Sports Med. 51, bjsports-2017-097699 (2017).
- Harmon, K. G. et al. American Medical Society for Sports Medicine position statement: concussion in sport. Br. J. Sports Med. 47, 15–26 (2013).
- Teasdale, G. & Jennett, B. ASSESSMENT OF COMA AND IMPAIRED CONSCIOUSNESS. A Practical Scale. Lancet (1974). doi:10.1016/S0140-6736(74)91639-0
- Maas, A. I. R. et al. Traumatic brain injury: integrated approaches to improve prevention, clinical care, and research. Lancet Neurol. 16, 987–1048 (2017).
- Graham R, Rivara FP, F. M. Neuroscience , Biomechanics , and Risks of Concussion in the Developing Brain. in Sports-Related Concussions in Youth: Improving the Science, Changing the Culture. (National Academies Press (US), 2014).
- Graham. Sports-Related Concussions in Youth: Improving the Science, Changing the Culture. Inst. Med. Rep. (2013). doi:10.7205/MILMED-D-14-00516
- F., H. et al. Six Degree-of-Freedom Measurements of Human Mild Traumatic Brain Injury. Annals of Biomedical Engineering (2015).
- CDC. What Is a Concussion? Available at: https://www.cdc.gov/headsup/basics/concussion_whatis.html.
- Mayo Clinic. Concussion. Available at: https://www.mayoclinic.org/diseases-conditions/concussion/symptoms-causes/syc-20355594.
- Giordano, C. & Kleiven, S. Evaluation of Axonal Strain as a Predictor for Mild Traumatic Brain Injuries Using Finite Element Modeling. Stapp Car Crash J. (2014).
- Giza, C. C. & Hovda, D. A. The Neurometabolic Cascade of Concussion. J. Athl. Train. 36, 228–235 (2001).
- Giza, C. C. & Hovda, D. A. The New Neurometabolic Cascade of Concussion. Neurosurgery 75, S24–S33 (2014).
- Clarke DD; Sokoloff L. Regulation of Cerebral Metabolic Rate. in Basic Neurochemistry: Molecular; Cellular and Medical (1999).
- Johnson, B. D. et al. Face cooling exposes cardiac parasympathetic and sympathetic dysfunction in recently concussed college athletes. Physiol. Rep. (2018). doi:10.14814/phy2.13694
- Levin, H. S. & Diaz-Arrastia, R. R. Diagnosis, prognosis, and clinical management of mild traumatic brain injury. Lancet Neurol. 14, 506–517 (2015).
- Ruff, R. M., Iverson, G. L., Barth, J. T., Bush, S. S. & Broshek, D. K. Recommendations for Diagnosing a Mild Traumatic Brain Injury: A National Academy of Neuropsychology Education Paper. Arch. Clin. Neuropsychol. 24, 3–10 (2009).
- Slobounov, S. M. et al. Alteration of brain functional network at rest and in response to YMCA physical stress test in concussed athletes: RsFMRI study. Neuroimage (2011). doi:10.1016/j.neuroimage.2011.01.024
- Dettwiler, A. et al. Persistent Differences in Patterns of Brain Activation after Sports-Related Concussion: A Longitudinal Functional Magnetic Resonance Imaging Study. J. Neurotrauma 31, 180–188 (2014).
- Churchill, N. W. et al. Neuroimaging of sport concussion: persistent alterations in brain structure and function at medical clearance. Sci. Rep. 7, 8297 (2017).
- Zemek, R. et al. Clinical Risk Score for Persistent Postconcussion Symptoms Among Children With Acute Concussion in the ED. JAMA 315, 1014 (2016).
- Seabury, S. A. et al. Assessment of Follow-up Care After Emergency Department Presentation for Mild Traumatic Brain Injury and Concussion: Results From the TRACK-TBI Study. JAMA Netw. open 1, e180210 (2018).
- Ellis, M. J., Leddy, J., Cordingley, D. & Willer, B. A Physiological Approach to Assessment and Rehabilitation of Acute Concussion in Collegiate and Professional Athletes. Front. Neurol. 9, 1–14 (2018).
- Ledoux, A.-A. et al. Natural Progression of Symptom Change and Recovery From Concussion in a Pediatric Population. JAMA Pediatr. 173, e183820 (2019).


Trackbacks/Pingbacks