
In this post, we discuss the pharmacology, myths, and a myriad of roles for Ketamine in the ED; including analgesia, sedation, agitation, alcohol withdrawal, and suicidal ideation.
Part I: Pharmacokinetics and pharmacodynamics of ketamine
- Produced in 1970s, structurally related to PCP
- Use declined with: advent of propofol, increasing documented cases of abuse, concerns regarding side effects and ICP effects1
- Relegated to “Horse Tranquilizer”
- Resurgence in its use in past 20 years2
Mechanism of action:
- NMDA receptor antagonist3
- Sympathomimetic reuptake inhibitor
- Dissociative anesthetic
Pharmacokinetics:
- Rapidly distributes across the blood brain barrier4
- Metabolized by the liver and eliminated by the kidneys
- Dosing based on ideal not actual body weight
- Onset IV: <1 min
- Duration (of dissociation) IV: 5-10 min
Pharmacodynamics: dosing ranges4
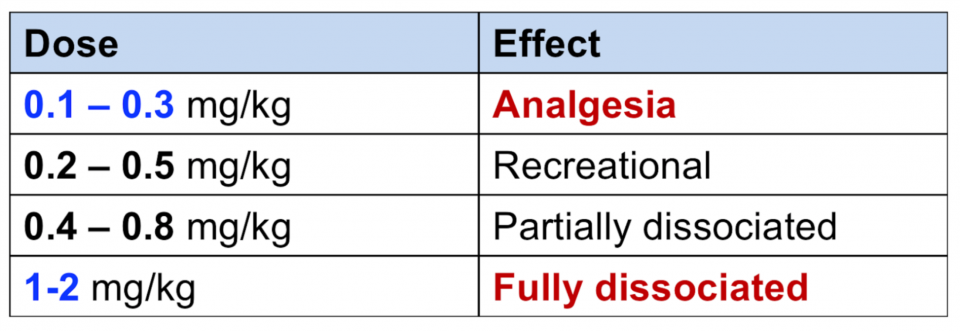
Take home points:
- Ketamine has different dosing ranges that are crucial to it’s use in the ED
- Ketamine should be used either in the:
- Analgesic dosing range (0.1-0.3 mg/kg), or
- Dissociative range (>1 mg/kg)
- Avoid in cases of psychotic disorders
- There are many uses for ketamine in the ED other than RSI
Part II: Ketamine for Analgesia
- There is interest in the ED for a non-opioid analgesic alternative such as subdissociative ketamine for the following reasons:
- Patients’ pain in the ED is often poorly controlled
- The rising opioid crisis
- The rising rate of chronic pain
Mechanism of action:
- Glutamate is released by afferent nociceptive neurons in the dorsal horn of the spinal cord5
- This pathway appears to be not only involved in acute pain but also involved in the development of chronic pain
- Central sensitization
- Opioid tolerance
- Opioid hyperalgesia
- Ketamine’s action of blocking these NMDA receptors should treat acute pain and also may help prevent chronic pain and opioid tolerance6
ED subdissociative ketamine combined with opioids:7-9
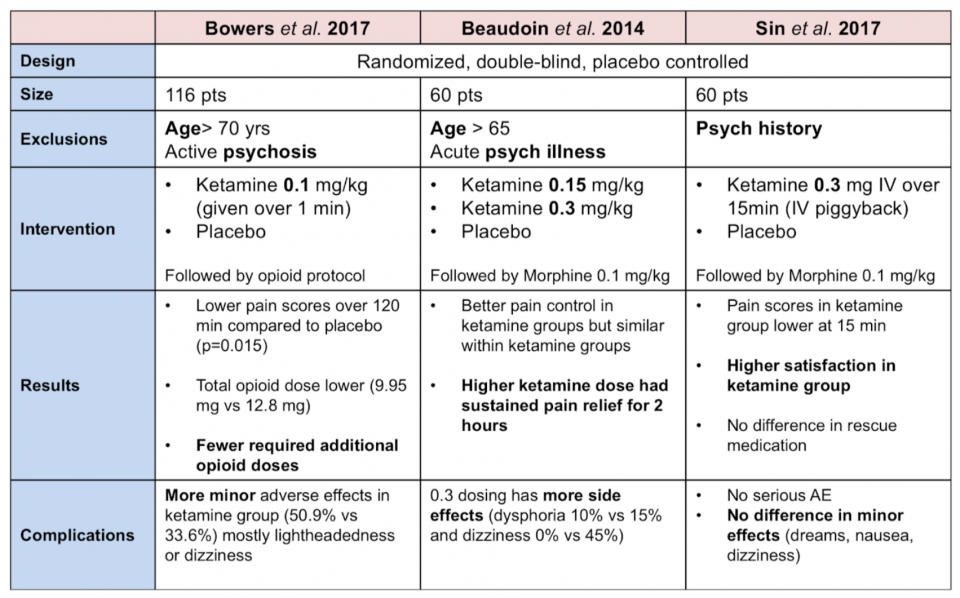
For a full review of Beaudoin et al. 2014 see here
ED subdissociative ketamine instead of opioids:10, 11
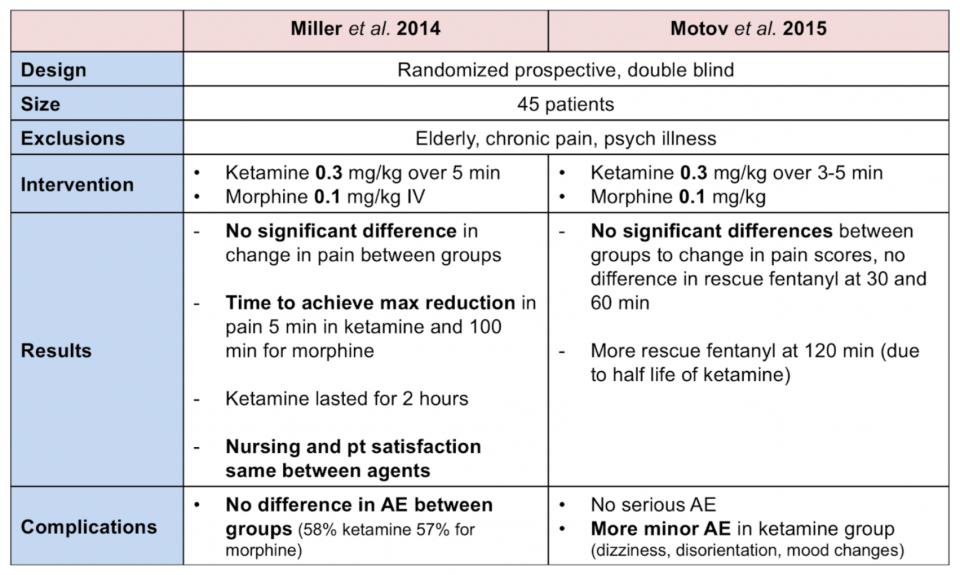
For a full review of Motov et al. 2015 see here
IV push vs short infusion:
- A study by Motov et al. 2017 compared giving ketamine 0.3 mg/kg IV over 5 min (IVP) OR mixed in 100 cc NS given over 15 min (short infusion)12
- Same analgesic effect in reducing pain scores
- They found feeling of unreality 91.7% IVP vs 54.2% infusion (p=0.008) and that the IVP group showed more sedation at 5 min (median RASS -2 vs 0)
Take home points:
- Subdissociative ketamine is a viable choice for treatment of both acute and chronic pain in the ED
- It can be given alone or combined with multimodal agents (ex: opioids)
- Dosing:
- 0.3 mg/kg IV over 15 min (mixed in 100 cc NS) – best evidence, or
- 0.1 mg/kg IVP over 3 min
- No monitoring is required at this dosing range
Part III: Ketamine for Procedural Sedation
Ketamine Single Agent Sedation
- Ketamine has been the single most popular agent for procedural sedation in children for over 20 years
- Has been underutilized as an agent in the adult population
- If single agent sedation – use a fully dissociative dose31-2 mg/kg IV
- 5 mg/kg IM
- Benefits:
- Potent analgesia, sedation, and amnesia
- Preserved respiratory drive and airway reflexes
- HD neutral/indirect sympathomimetic
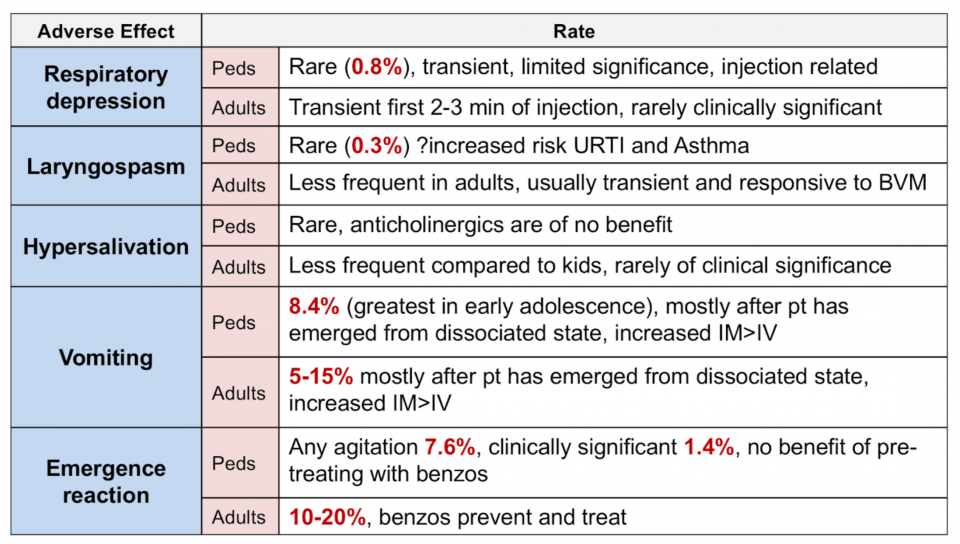
Ketamine single agent sedation: Adverse effects13-15
Ketamine single agent sedation: Contraindications
Absolute:3
- Age < 3 months
- Schizophrenia
Relative:
- Procedures with laryngeal stimulation
- Okay for ED procedures (oral laceration, dental, foreign body removal)
- High rate of laryngospasm in EGD (8%)
- URTI (peds)
- Cardiac disease (increased myocardial oxygen demand)
Ketamine single agent sedation: Mitigating Common Adverse Effects
Nausea:
- Prophylactic Zofran may reduce vomiting
Emergence reactions:
- Routine prophylactic benzos may benefit adults but not children
- Midazolam 0.03 mg/kg IV effective to prevent and terminate emergence in adults
Multi Agent Sedation with Ketamine
- A study done by Messenger et al. in 2008 compared using ketamine 0.3 mg/kg IV vs Fentanyl 1.5 mcg/kg in addition to titrated Propofol16
- They found severe adverse events occurred in 0% of the ketamine group and 16% of the fentanyl group
- The ketamine group also had:
- Smaller propofol requirement
- Shorter recovery time
- No difference in patient or team satisfaction
- Zero cases of emergence phenomenon
See here for Andolfatto et al.‘s 2012 study on the effectiveness of “Ketofol” in procedural sedation
Take home points:
Ketamine single agent
-
- Give full dissociative dose (1-2 mg/kg)
- Consider prophylactic ondansetron and midazolam
- Benzos to treat emer gence (consider routinely writing a PRN)
0.3 mg/kg and titrated Propofol
-
- Less adverse reactions compared to fentanyl and Propofol
- Less emergence reactions
Part IV: Ketamine for Agitation
- Classically options have included benzodiazepines, antipsychotics, or combinations of both
- Emerging evidence to use Ketamine IM as an alternative for undifferentiated agitation
- Listed on ACEP white paper for agents to be used for agitated delirium17
- Being rolled out to EMS in Ontario in the next few months
Evidence: Ketamine as Rescue
- Isbister et al. 2016 performed an observational prospective study looking at ketamine as rescue for difficult to sedate pts in ED18
-
- Most pts received 2 doses of 10mg droperidol prior (some 3 doses)
- Received Ketamine 4-6 mg/kg IM
- 6% had adverse effects
- Vomiting (n=2); oxygen desat to 90% (n=1)
Evidence: Ketamine single agent for agitation
Con studies:
- Two studies by Cole et al. published in 2016 and 2017 looked at prehospital use of Ketamine 5 mg IM for sedation of agitated patients19,20
- Ketamine worked very quickly (time to sedation): 4-5 min
- Extremely high rate of adverse events, most notably ED intubation rates of 39% and 57%; not entirely clear why rate so high
Pro studies:
- Riddell et al. published a prospective ED study in 2017 comparing different agents for sedation of agitated patients21
- Time to sedation fastest in ketamine group (6.6 min vs 15 min for midazolam and 13.4 min for Haldol)
- Changes in vital signs similar between groups
- 2 intubations in ketamine group, single intubation in other groups
- Limitations: too small to detect serious adverse events, small doses of sedatives used
Take home points:
- Ketamine 5 mg/kg IM is a viable option for sedating agitated patients
- More studies are needed to determine rates of rare but serious adverse events
- Current suggestions for use:
- Initial dose(s) of benzos fail (second line agent), or
- Extremely rapid take down (required for safety)
Part V: Ketamine for Alcohol Withdrawal
Mechanism of ketamine in alcohol withdrawal:
- Repeated EtOH use causes:22
- Downregulation of GABA receptors
- Upregulation of excitatory NMDA receptors
- Most treatments simulate GABA receptors (benzos, Propofol, phenobarbital)
- Ketamine as an NMDA receptor antagonist works on other side of pathophysiology
Evidence:23-25
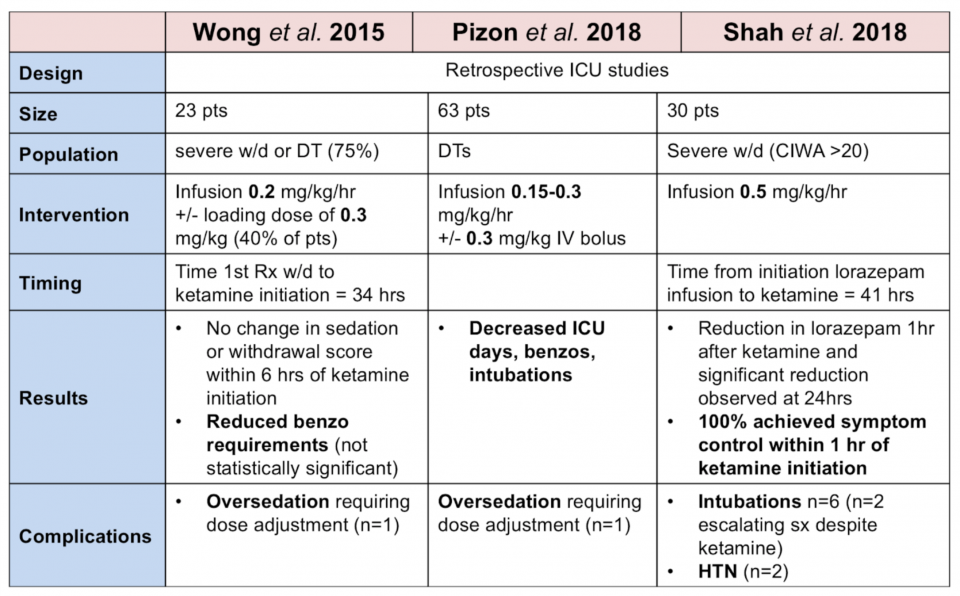
Take home points:
- Limited evidence for Ketamine use in EtOH withdrawal, none are ED studies
- Consider in ED if large doses of benzos and considering intubation
- Most studies used infusion at 0.1-0.3 mg/kg/hr +/- bolus of 0.3 mg/kg
- Benzos remain by far first line for EtOH withdrawal
Part VI: Ketamine for Suicidal Ideation
Ketamine for depression:
- Berman et al. 1990 published a small study with 7 patients showing that ketamine 0.5 mg/kg possessed antidepressant qualities26
- Many subsequent trials support this effect but antidepressant effects seems to be transient (effect abating at about 1 week post infusion)
Ketamine for suicidal ideation:
- Grunebaum et al. in 2018 performed a double blind RCT with 80 inpatients (voluntary admission) and compared Ketamine 0.5 mg/kg over 40 mins vs. Midazolam 0.02 mg/kg (active control)27
- They found that ketamine had greater reduction in suicidality (SSI score) 55% vs 30% on day 1 (NNT=4)
- A meta-analysis published in 2018 by Wilkinson et al. included 10 studies done in a variety of settings (none the ED) and found that Ketamine rapidly reduced suicidal thoughts, within 1 day and for up to 1 week in depressed patients with suicidal ideation28
Ketamine for suicidal ideation in the ED:
A study done by Kashni et al. in 2014 looked at EPs administering ketamine to decrease suicidality in the ED29
- Patients received Ketamine 0.2 mg/kg IV over 1 min
- Suicidal ideation measured with standardized scales before injection, 40 min, 80 min, 120 min, 10 days via telephone
- 10 day follow-up → 85.7% did not have any suicidal thoughts
- Numerous limitations:
- No control group, small study
- Different setting compared to Canadian EDs
- Ethical implications
- Abuse potential
Take home points:
- No role at present for ketamine use in the ED for suicidality
- More studies needed, logistical, and ethical roadblocks remain
- Possible future role (after much more study) for single dose ketamine in the ED and expedited follow up for selected patients with suicidal ideation
References:
- Mion G. History of anaesthesia: The ketamine story – past, present and future. Eur J Anaesthesiol. 2017;34(9):571-575.
- Sheikh S, Hendry P. The Expanding Role of Ketamine in the Emergency Department. Drugs. 2018;
- Green SM, Roback MG, Kennedy RM, Krauss B. Clinical practice guideline for emergency department ketamine dissociative sedation: 2011 update. Ann Emerg Med. 2011;57(5):449-61.
- Strayer. SMACC Presentation 2015 https://www.smacc.net.au/2015/12/ketamine-how-to-use-it-fearlessly-for-all-its-indications-by-reuben-strayer/
- Gorlin AW, Rosenfeld DM, Ramakrishna H. Intravenous sub-anesthetic ketamine for perioperative analgesia. J Anaesthesiol Clin Pharmacol. 2016;32(2):160-7.
- Kurdi MS, Theerth KA, Deva RS. Ketamine: Current applications in anesthesia, pain, and critical care. Anesth Essays Res. 2014;8(3):283-90.
- Bowers KJ, Mcallister KB, Ray M, Heitz C. Ketamine as an Adjunct to Opioids for Acute Pain in the Emergency Department: A Randomized Controlled Trial. Acad Emerg Med. 2017;24(6):676-685.
- Beaudoin FL, Lin C, Guan W, Merchant RC. Low-dose ketamine improves pain relief in patients receiving intravenous opioids for acute pain in the emergency department: results of a randomized, double-blind, clinical trial. Acad Emerg Med. 2014;21(11):1193-202.
- Sin B, Tatunchak T, Paryavi M, et al. The Use of Ketamine for Acute Treatment of Pain: A Randomized, Double-Blind, Placebo-Controlled Trial. J Emerg Med. 2017;52(5):601-608.
- Miller JP, Schauer SG, Ganem VJ, Bebarta VS. Low-dose ketamine vs morphine for acute pain in the ED: a randomized controlled trial. Am J Emerg Med. 2015;33(3):402-8.
- Motov S, Rockoff B, Cohen V, et al. Intravenous Subdissociative-Dose Ketamine Versus Morphine for Analgesia in the Emergency Department: A Randomized Controlled Trial. Ann Emerg Med. 2015;66(3):222-229.e1.
- Motov S, Mai M, Pushkar I, et al. A prospective randomized, double-dummy trial comparing IV push low dose ketamine to short infusion of low dose ketamine for treatment of pain in the ED. Am J Emerg Med. 2017;35(8):1095-1100.
- Strayer RJ, Nelson LS. Adverse events associated with ketamine for procedural sedation in adults. Am J Emerg Med. 2008;26(9):985-1028.
- Green SM, Roback MG, Krauss B, et al. Predictors of airway and respiratory adverse events with ketamine sedation in the emergency department: an individual-patient data meta-analysis of 8,282 children. Ann Emerg Med. 2009;54(2):158-68.e1-4.
- Bhatt M, Johnson DW, Chan J, et al. Risk Factors for Adverse Events in Emergency Department Procedural Sedation for Children. JAMA Pediatr. 2017;171(10):957-964.
- Messenger DW, Murray HE, Dungey PE, Van vlymen J, Sivilotti ML. Subdissociative-dose ketamine versus fentanyl for analgesia during propofol procedural sedation: a randomized clinical trial. Acad Emerg Med. 2008;15(10):877-86.
- ACEP White Paper Report on Excited Delirium Syndrome 2009
- Isbister GK, Calver LA, Downes MA, Page CB. Ketamine as Rescue Treatment for Difficult-to-Sedate Severe Acute Behavioral Disturbance in the Emergency Department. Ann Emerg Med. 2016;67(5):581-587.e1.
- Cole JB, Klein LR, Nystrom PC, et al. A prospective study of ketamine as primary therapy for prehospital profound agitation. Am J Emerg Med. 2017;
- Cole JB, Moore JC, Nystrom PC, et al. A prospective study of ketamine versus haloperidol for severe prehospital agitation. Clin Toxicol (Phila). 2016;:1-7.
- Riddell J, Tran A, Bengiamin R, Hendey GW, Armenian P. Ketamine as a first-line treatment for severely agitated emergency department patients. Am J Emerg Med. 2017;35(7):1000-1004.
- Nelson LS, Lewin NA, Howland MA et al. Goldfrank’s Toxicologic Emergencies, Ninth Edition. McGraw Hill Professional; 2010.
- Wong A, Benedict NJ, Armahizer MJ, Kane-gill SL. Evaluation of adjunctive ketamine to benzodiazepines for management of alcohol withdrawal syndrome. Ann Pharmacother. 2015;49(1):14-9.
- Pizon AF, Lynch MJ, Benedict NJ, et al. Adjunct Ketamine Use in the Management of Severe Ethanol Withdrawal. Crit Care Med. 2018;
- Shah P, Mcdowell M, Ebisu R, Hanif T, Toerne T. Adjunctive Use of Ketamine for Benzodiazepine-Resistant Severe Alcohol Withdrawal: a Retrospective Evaluation. J Med Toxicol. 2018;
- Berman RM, Cappiello A, Anand A, et al. Antidepressant effects of ketamine in depressed patients. Biol Psychiatry. 2000;47(4):351-4.
- Grunebaum MF, Galfalvy HC, Choo TH, et al. Ketamine for Rapid Reduction of Suicidal Thoughts in Major Depression: A Midazolam-Controlled Randomized Clinical Trial. Am J Psychiatry. 2018;175(4):327-335.
- Wilkinson ST, Ballard ED, Bloch MH, et al. The Effect of a Single Dose of Intravenous Ketamine on Suicidal Ideation: A Systematic Review and Individual Participant Data Meta-Analysis. Am J Psychiatry. 2018;175(2):150-158.
- Kashani P, Yousefian S, Amini A, Heidari K, Younesian S, Hatamabadi HR. The Effect of Intravenous Ketamine in Suicidal Ideation of Emergency Department Patients. Emerg (Tehran). 2014;2(1):36-9.


May I please get a copy of all the citations used for this lecture? The content is great and I would like to cite appropriately.
Thanks – Susan