

Procedural sedation is commonly performed in the Emergency Department. It is a critical tool that helps facilitate unpleasant but often necessary procedures that our patients would otherwise not tolerate.
However, procedural sedation is also an extraordinarily resource-intensive endeavor. Most often, it requires cardiac monitoring and many interprofessional personnel. Also, despite its frequent use, it is an area where there is significant practice variation and many controversies.
In this post, the first in a two-part series, we will delve into these controversies regarding procedural sedation and explore how to reduce resource utilization and ED length of stay. To illustrate these points, let’s begin with a case.
Case
- 30M presenting to the ED for an unstable trimalleolar fracture after a mechanical fall while skating on the Rideau Canal
- Orthopedics service asks you to perform procedural sedation to allow for reduction
- Patient is otherwise healthy with a reassuring airway exam
- However, he states that 30 minutes prior, he ate a burger, and large fries.
In PART 1, we will discuss the need for fasting prior to ED procedural sedations.
In PART 2, we will review the safety profile and adverse event rates of Ketamine and Propofol – two commonly used agents in procedural sedation. We will subsequently explore whether agent choice affects sedation time and ED LOS.
Aspiration during Sedation – How common is it?
OR Data
Historical data from the 1960-1980’s suggested rates of aspiration as high as:
- 1 in 400 for pediatric emergency anesthetics
- 1 in 600-800 for adult emergency anesthetics1
However, contemporary data suggest that true rates of aspiration in patients undergoing general anesthesia are closer to 0.7-10.2 cases per 10 0002.
Risk Factors
Risk factors for aspiration were described to be3:
- Airway difficulties (i.e. difficult intubation, laryngospasm)
- Emergency surgery
- Advanced age (i.e. >70yrs)
- Higher ASA Class
- Conditions predisposing to gastroesophageal reflux
- Hiatal hernia
- Small bowel obstruction
- Ileus
- Elevated ICP
ED Sedation is Different
Procedural sedation in the ED is very different compared to general anesthesia in the OR. There are fundamental difference that likely further reduce the rates of aspiration in our population.
Green (2002) describes the following differences:
- 2/3 of aspirations during general anesthesia occur during manipulations of the airway (i.e. laryngoscopy, intubation, extubation)
- Airway manipulation is exceedingly rare in ED sedations
- Higher ASA score was associated with increased aspiration
- The majority of patients being sedated in the ED are healthy (ASA I & II)
- Up to 40% of patients undergoing GA in the OR are ASA ≥ III
- Inhalational agents used throughout the duration general anesthesia are emetogenic
- Our sedations are brief and do not involve the use of emetogenic agents throughout the sedation
- Ketamine is considered emetogenic, but it’s rates of post-sedation emesis are lower than that of general anesthetics
In 2017, Green performed a systematic review looking at all reported cases of pulmonary aspiration during procedural sedation outside the OR4:
- He identified 192 articles in which aspiration was recorded as an adverse event
- 34 cases of aspiration in non-endoscopy procedures
- NONE in ASA I & II patients
- Most cases of aspiration occurred in patients with significant comorbidities (e.g. active cancer, severe GERD, or neurologic conditions)
- This is not the patient population that we are routinely sedating in the ED
Knowing that general anesthesia in the OR and out-of-OR procedural sedation are fundamentally different, what do the guidelines recommend regarding procedural sedations in the ED environment?
Fasting Prior to Procedural Sedation – The Guidelines
Traditionally, it has been suggested that patients should meet fasting guidelines prior to procedural sedation. This teaching predominately comes from the ASA’s Practice Guideline for Sedation and Analgesia by Non-Anesthesiologists published in 2002 (and earlier iterations).
It suggested that our patients should meet the following fasting guidelines prior to procedural sedation5,6:
- NPO to clear fluids ≥2h
- NPO to other fluids & solids ≥ 6h
They state that for urgent/emergent situations, we should consider lighter sedation or intubation in patients who have not met fasting guidelines.
Continuing with our case, the patient may not tolerate adequate reduction of an unstable orthopedic injury with lighter sedation and intubation in the ED to facilitate this seems excessive.
Interestingly, within the guideline paper itself, the ASA notes that:
The literature does not provide sufficient evidence to test the hypothesis that preprocedure fasting results in a decreased incidence of adverse outcomes in patients undergoing either moderate or deep sedation.5
Since 2002, various other guiding agencies have put out statements on procedural sedation that advocate for less restrictive fasting guidelines.
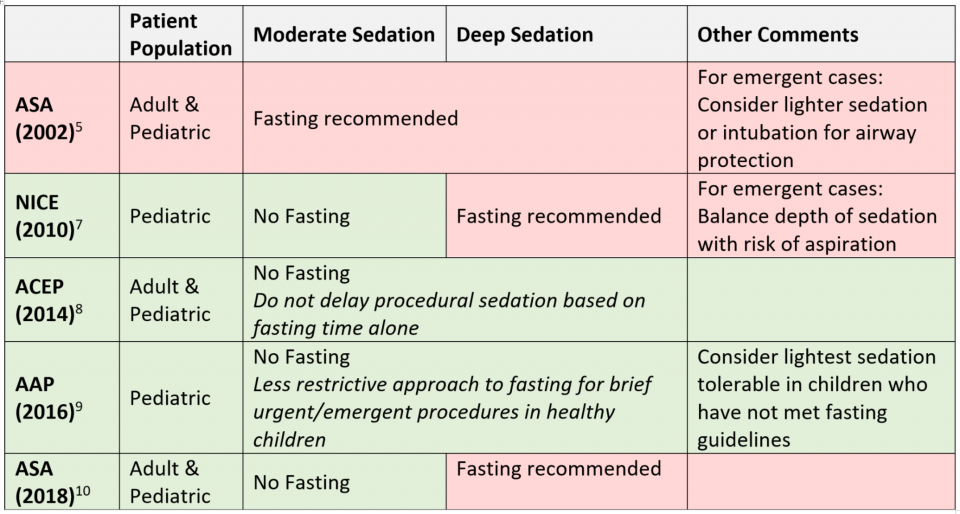
As noted in table above, our guiding agency, the American College of Emergency Physicians (ACEP), released a Clinical Policy & Position Paper in 2014 which recommended the following8:
- Do not delay procedural sedation based on fasting times alone
- Recommendation based on appraisal of the literature which showed no evidence that fasting reduces risk of emesis or aspiration in ED sedations
This overview of guidelines shows a wide variation in recommendations regarding preprocedural fasting by various guiding agencies. This suggests that preprocedural fasting is still an area of controversy. Let’s see what the contemporary literature shows.
Fasting Prior to Procedural Sedation – Review of Recent Literature
Major Adverse Events and Relationship to NPO Status in Pediatric Sedation/Anesthesia Outside the Operating Room – Beach et al. Anesthesiology (2016)11
Database study involving 42 Pediatric Hospitals
- 139 142 Pediatric Sedations outside the OR
- 30 089 (21.6%) performed by Emergency Physicians
Fasting data available for 107 947 (77.6%) patients
- 82 546 (59.3%) were NPO
- 25 401 (17.5%) were not NPO
Had 10 cases of aspiration
- 8 out of 82 546 in NPO group = 0.97 per 10 000
- 2 out of 25 401 in Non-NPO group = 0.79 per 10 000
- No statistically significant difference between NPO and non-NPO groups
- No cases of aspiration in sedations performed by Emergency Physicians
Major Complications
- Aspiration, cardiac arrest, death, or unexpected admission
- NPO group = 5.6 per 10 000
- Non-NPO group = 5.9 per 10 000
- No statistically significant difference between NPO and non-NPO groups
This is a study with a huge population size. However, it is not solely an ED-based study. In fact, 58.0% of their patient cohort was sedated for MRI/CT – not typical of reasons we would be sedating for in the ED.
So what does contemporary ED literature show?
Procedural Sedation in the Emergency Department by Dutch Emergency Physicians: a Prospective Multicentre Observational Study of 1711 Adults – Smits et al. Emergency Medicine Journal (2016)12
Prospective observational study at 8 hospitals in the Netherlands
- 1711 adults undergoing procedural sedation performed by EPs
Fasting data available for 1311 patients
- 249 (19%) were fasted <3h
- 582 (44.4%) were fasted 3-6h
- 480 (36.6%) were fasted >6h
Regardless of fasting time, no aspiration events were noted.
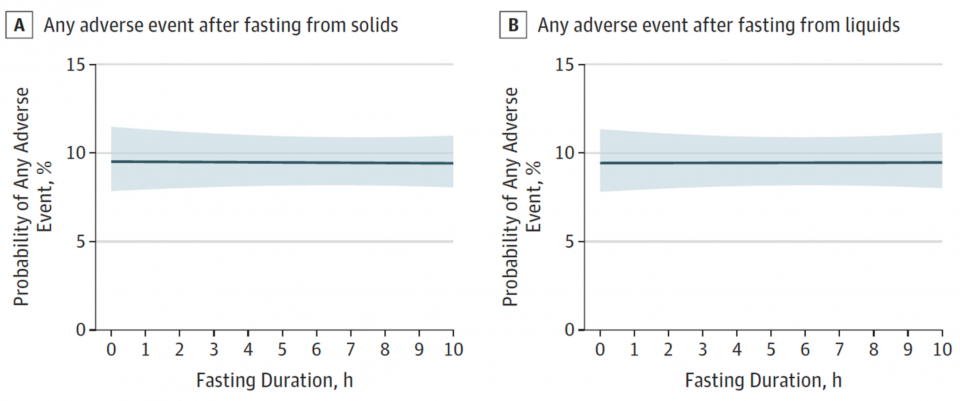
Association of Preprocedural Fasting With Outcomes of Emergency Department Sedation in Children – Bhatt et al. JAMA Pediatrics (2018)13
Prospective multicenter observational cohort study in 6 Canadian Pediatric EDs
- 6183 Patients undergoing ED procedural sedation
Over 50% of their patient cohort did not meet fasting criteria
- 2974 (48.1%) were not NPO for solids
- 310 (5.0%) were not NPO for liquids
NO ASPIRATIONS REGARDLESS OF FASTING STATUS
They also showed that duration of fasting had no effect on rate of adverse events.
Summary & Conclusions
There is a wealth of literature looking at the relationship between fasting and rates of aspiration in ED sedations. Below is a summary of results from studies since 2000:
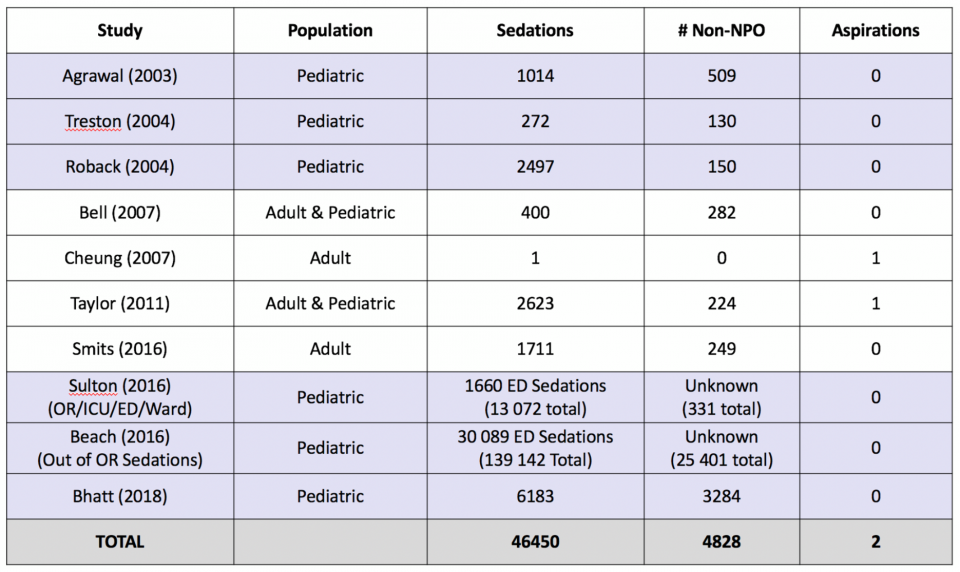
In approximately 46 500 ED based procedural sedations described in the recent literature, >4800 of which were performed in patients who had not met fasting criteria, there were only 2 reported cases of aspiration11–20; both of these were in adults who had met fasting guidelines.
In fact, in the Pediatric literature, there have never been any reported cases of pulmonary aspiration in children undergoing parenteral sedation in the ED setting despite widespread non-adherence with fasting guidelines.
Bottom Line
Adherence to fasting guidelines is unnecessary in healthy patients undergoing procedural sedation in the ED. Aspiration is an incredibly rare event in ED sedations.
ACEP’s Clinical Policy on Procedural Sedation in the ED recommends that we do not delay procedural sedation based on fasting time alone and a review of the existing literature supports this recommendation. There is no evidence that preprocedural fasting reduces rates of adverse events including aspiration.
We are taught to consider the adverse events related to sedating non-fasted patients, but rarely do we think about the downsides of delaying an important procedure. Fasting increases our patients’ length of stay in the Emergency Department. Furthermore, delaying procedures leaves patients in pain/discomfort longer, requiring more opioid analgesia as they wait, and potentially makes the procedure more difficult (e.g. dislocations become more difficult to reduce with time, atrial fibrillation can become more difficult to cardiovert the longer patients are in it, etc.).
Caveats & Directions for Future Research
The vast majority of recommendations presented above come from data derived from studies of healthy (ASA I & II) patients. There is insufficient data in the literature exploring the relationship between rates of adverse events and fasting duration in high ASA class patients. This is an area that requires further research.
Furthermore, it has been shown that certain procedures such as EGD and bronchoscopy are associated with higher rates of adverse events4.
Thus, we should consider the following risk factors and adjust our sedation strategy accordingly:
- High ASA Status
- Medical conditions predisposing patients to regurgitation (i.e. hiatal hernia, SBO, elevated ICP, etc.)
- High risk procedures
- EGD
- Bronchoscopy
References
- Kalinowski CPH, Kirsch JR. Strategies for prophylaxis and treatment for aspiration. Best Pract Res Clin Anaesthesiol. 2004;18(4):719-737. doi:10.1016/j.bpa.2004.05.008.
- Ng A. Gastroesophageal reflux and aspiration of gastric contents. Anesth Analg. 2002;94(3):762-763. http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=Citation&list_uids=11867413.
- Green, SM; Krauss B. Pulmonary Aspiration Risk during Emergency. Acad Emerg Med. 2002;9(1):35-42. doi:10.1197/aemj.9.1.35.
- Green SM, Mason KP, Krauss BS. Pulmonary aspiration during procedural sedation: A comprehensive systematic review. Br J Anaesth. 2017;118(3):344-354. doi:10.1093/bja/aex004.
- Anesthesiologists A society for. Practice Guidelines for Sedation and Analgesia by Non-Anesthesiologists. Anesthesiology. 2002;84(2):459-471. doi:10.1097/00000542-199602000-00029.
- AMERICAN SOCIETY OF ANESTHESIOLOGISTS COMMITTEE. Practice Guidelines for Preoperative Fasting and the Use of Pharmacologic Agents to Reduce the Risk of Pulmonary Aspiration: Application to Healthy Patients Undergoing Elective Procedures. Anesthesiology. 2011;114(3):495-511. doi:10.1097/ALN.0b013e3181fcbfd9.
- NICE. Sedation in children and young people. 2010;(December).
- Godwin SA, Burton JH, Gerardo CJ, et al. Clinical Policy: Procedural Sedation and Analgesia in the Emergency Department. Ann Emerg Med. 2014;63(2):247-258. doi:10.1016/j.annemergmed.2013.10.015.
- Cote CJ, Wilson S. Guidelines for Monitoring and Management of Pediatric Patients Before, During, and After Sedation for Diagnostic and Therapeutic Procedures: Update 2016. Pediatrics. 2016;138(1):e20161212-e20161212. doi:10.1542/peds.2016-1212.
- Anesthesiologists A society for. Practice Guidelines for Moderate Procedural Sedation and Analgesia 2018. Vol 128.; 2018. doi:10.1097/ALN.0000000000002043.
- Beach ML, Cohen DM, Gallagher SM, Cravero JP. Major Adverse Events and Relationship to Nil per Os. 2016;(January):80-88.
- Smits GJP, Kuypers MI, Mignot LAA, et al. Procedural sedation in the emergency department by Dutch emergency physicians: A prospective multicentre observational study of 1711 adults. Emerg Med J. 2017;34(4):237-242. doi:10.1136/emermed-2016-205767.
- Bhatt M, Johnson DW, Taljaard M, et al. Association of preprocedural fasting with outcomes of emergency department sedation in children. JAMA Pediatr. 2018;172(7):678-685. doi:10.1001/jamapediatrics.2018.0830.
- Bhatt M, Johnson DW, Chan J, et al. Risk factors for adverse events in emergency department procedural sedation for children. JAMA Pediatr. 2017;171(10):957-964. doi:10.1001/jamapediatrics.2017.2135.
- Treston G. Prolonged pre-procedure fasting time is unnecessary when using titrated intravenous ketamine for paediatric procedural sedation. EMA – Emerg Med Australas. 2004;16(2):145-150. doi:10.1111/j.1742-6723.2004.00583.x.
- Roback MG, Bajaj L, Wathen JE, Bothner J. Preprocedural fasting and adverse events in procedural sedation and analgesia in a pediatric emergency department: Are they related? Ann Emerg Med. 2004;44(5):454-459. doi:10.1016/j.annemergmed.2004.03.015.
- Bell A, Treston G, McNabb C, Monypenny K, Cardwell R. Profiling adverse respiratory events and vomiting when using propofol for emergency department procedural sedation. EMA – Emerg Med Australas. 2007;19(5):405-410. doi:10.1111/j.1742-6723.2007.00982.x.
- Cheung KW, Watson ML, Field S, Campbell SG. Aspiration Pneumonitis Requiring Intubation After Procedural Sedation and Analgesia: A Case Report. Ann Emerg Med. 2007;49(4):462-464. doi:10.1016/j.annemergmed.2006.09.004.
- Taylor DM, Bell A, Holdgate A, et al. Risk factors for sedation-related events during procedural sedation in the emergency department. EMA – Emerg Med Australas. 2011;23(4):466-473. doi:10.1111/j.1742-6723.2011.01419.x.
- Sulton C, McCracken C, Simon HK, et al. Pediatric Procedural Sedation Using Dexmedetomidine: A Report From the Pediatric Sedation Research Consortium. Hosp Pediatr. 2016;6(9):536-544. doi:10.1542/hpeds.2015-0280.


Trackbacks/Pingbacks