

In this two part series, we are delving into a few of the many controversies regarding procedural sedation and explore how to reduce resource utilization and ED length of stay.
In PART 1, we discussed preprocedural fasting and concluded that adherence to fasting guidelines is unnecessary in healthy patients undergoing procedural sedation in the ED. A review of existing literature showed no evidence that preprocedural fasting reduces rates of adverse events, including aspiration, in ED sedations.
In PART 2, we will review the safety profile and adverse event rates of Ketamine and Propofol – two commonly used agents in procedural sedation. We will subsequently explore whether agent choice affects sedation time and ED LOS.
Procedural sedation is commonly performed in the Emergency Department. It is a critical tool that helps facilitate unpleasant but often necessary procedures that our patients would otherwise not tolerate.
However, procedural sedation is also an extraordinarily resource-intensive endeavour. Most often, it requires cardiac monitoring and many interprofessional personnel. Also, despite its frequent use, it is an area where there is wide practice variation and many controversies.
Consider this illustrative case:
- 30M presenting to the ED for an unstable trimalleolar fracture after falling while skating on the Rideau Canal
- Orthopedics asks you to perform procedural sedation to allow for reduction
- Patient is otherwise healthy with a reassuring airway exam
- However, he states that 30 minutes prior, he ate a burger and large fries
Basics of Sedation
Continuum of Sedation
When performing procedural sedation, patients can be sedated to varying depths. Depth of sedation is typically categorized based on the following Continuum of Depth of Sedation described by the American Society of Anesthesiologists (ASA)1.
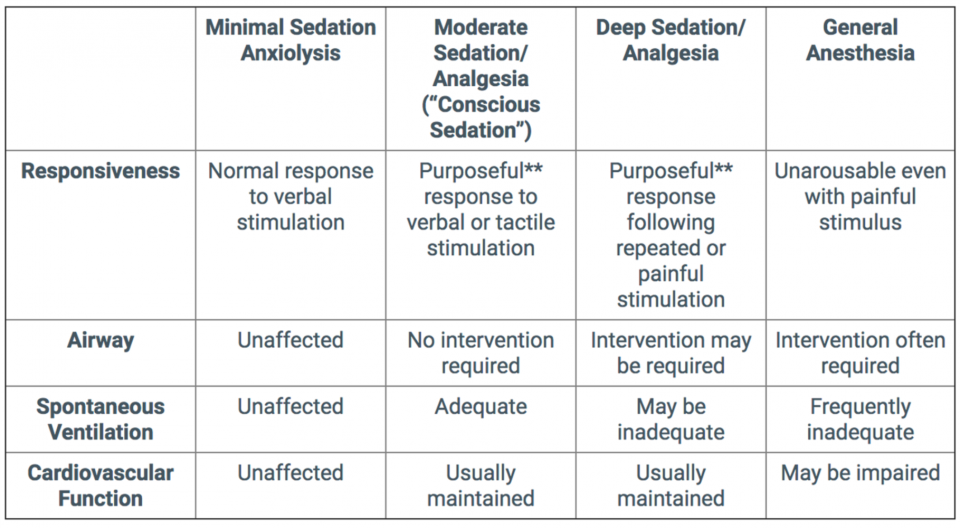
Traditionally, ED procedural sedations have been described as Moderate Sedation or “Conscious Sedation”. However, I would argue that according to the ASA categorization above, the majority of contemporary ED sedations lie in the Deep Sedation or General Anesthesia category.
During reductions of unstable fractures, we do not want our patients to be purposefully reaching or withdrawing in response to simple verbal or tactile stimulation. For optimal reduction conditions, it is desirable that our patients have minimal response to manipulation of their fracture.
Pharmacokinetics of Procedural Sedation
In an informal survey of ED physicians at our site, it appears that Propofol and Ketamine are the agents most commonly used in procedural sedations in our ED. Both are sedative or dissociative agents with a rapid time of onset that are used to facilitate painful or unpleasant procedures.
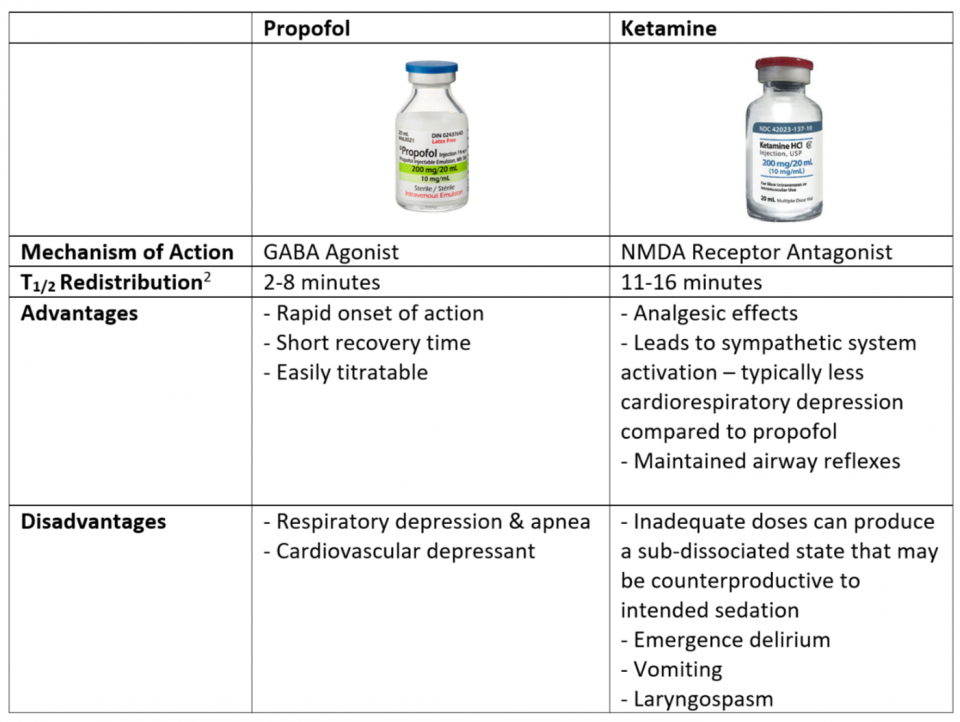
It is important to note the difference in the half life of redistribution (T1/2 Redistribution) between these two agents.
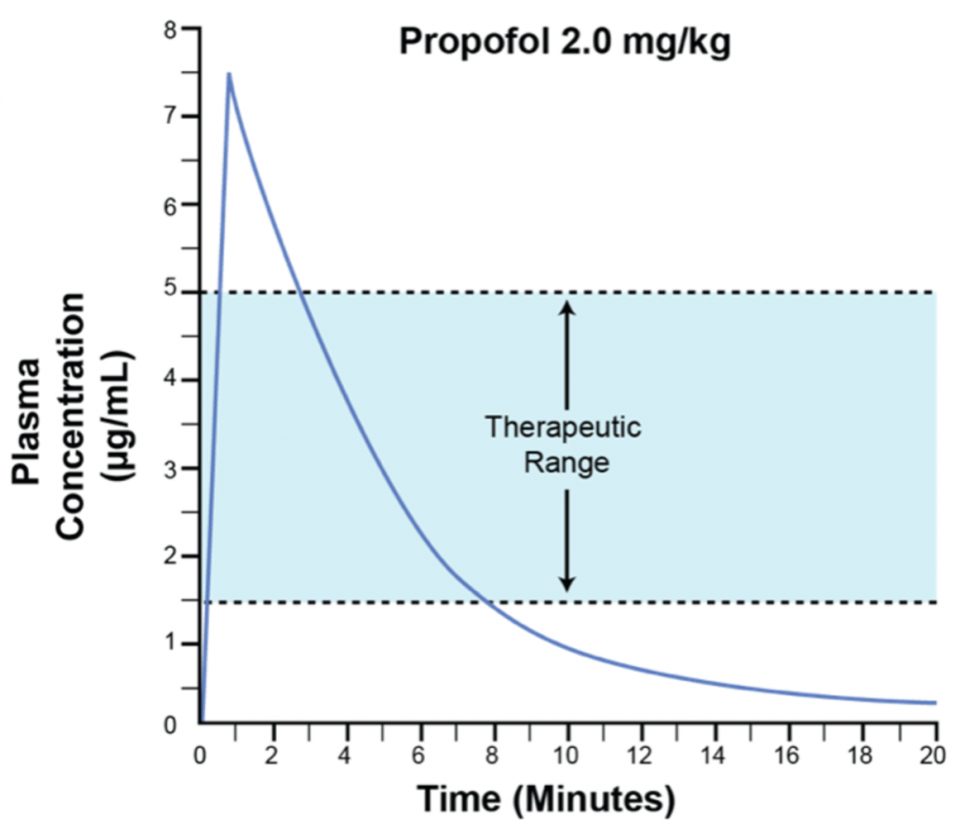
Above is a graph of plasma concentration over time following a bolus of Propofol2. After the initial peak in plasma concentration, the level rapidly falls within minutes. The fall in plasma concentration is due to redistribution of the drug into peripheral tissues.
Likewise, Ketamine also redistributes into the peripheral tissues. Thus the T1/2 of each drug gives us clues as to the duration of sedation.
The Ketamine Brain Continuum3
Another key difference between Propofol and Ketamine is the clinical effects of these agents when utilized at different mg/kg doses. Higher/lower doses of Propofol result in varying levels of sedation. However, the effect of Ketamine varies based on dosing as shown below:
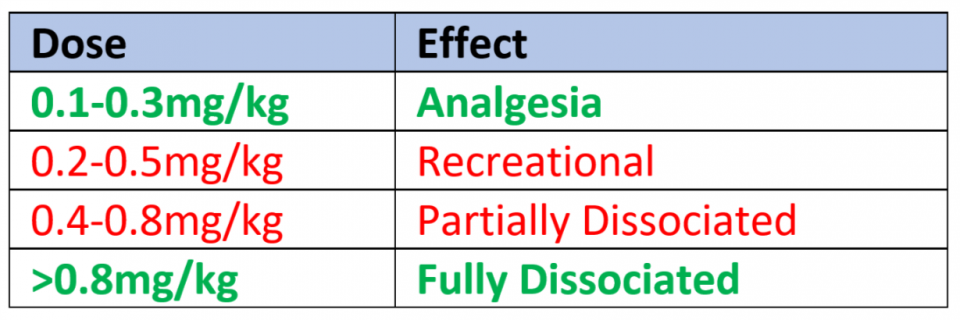
Depending on the indication, ketamine in the ED should either be dosed at the analgesic level or the fully dissociative level. In the partially dissociated state, patients may maintain some awareness and may make some purposeful movements. While most patients tolerate the partially-dissociated state well, it is a terrifying experience for some patients. As a result, in healthy patients undergoing procedural sedation in the ED, partial dissociation should be avoided.
If you find your patient to be in a partially dissociated state and in distress following your initial dose of ketamine, administer a repeat dose to help them reach the fully dissociated state.
Safety and Adverse Events – Ketamine vs Propofol
As we just discussed, Ketamine and Propofol are very different sedation agents that both produce desired effects in ED sedations. Ketamine was synthesized following World War II and was used extensively as a sedative and anesthetic. It fell out of favour with the advent of Propofol due to (1) Propofol’s ease of use and (2) the negative connotation from Ketamine’s use as a recreational drug. In the last 10-20 years, Ketamine has seen a resurgence due to its favourable cardiorespiratory profile.
It is clear that each of these sedative agents have their advantages and disadvantages. In this section, we will explore what the differences between Propofol and Ketamine are in terms of adverse events and more importantly, whether these difference are statistically and clinically significant.
To determine the adverse event rates during ED procedural sedations, we will examine the following papers:
ADULT DATA: Incidence of Adverse Events in Adults Undergoing Procedural Sedation in the Emergency Department: A Systematic Review and Meta-analysis. – Bellolio et al. Academic Emergency Medicine (2016)4
- Systematic review and meta-analysis of 55 studies (30 observational and 25 RCT)
- Population = Adult patients undergoing procedural sedation in the ED
- 9652 total sedations
NOTE: The reported rates of respiratory and cardiovascular adverse events in this paper appear low compared to what we have seen in clinical practice. This may be driven by reporting bias in the observational studies included in the meta-analysis. Indeed when Bellolio et al. analyzed only the RCTs, they showed a higher rate of desaturation and apnea overall. However, the authors did not break down adverse events by sedating agent for the RCTs alone, so we are unable to present these numbers.
That being said, this was a well conducted systematic review and the best evidence that we have to date.
PEDIATRIC DATA: What Works and What’s Safe in Pediatric Emergency Procedural Sedation: An Overview of Reviews. – Hartling et al. Academic Emergency Medicine (2016)5
- Summary of 14 systematic reviews
- Population = Children undergoing procedural sedation in the ED or similar settings
- >60 000 sedations
The results from these two papers are summarized below.
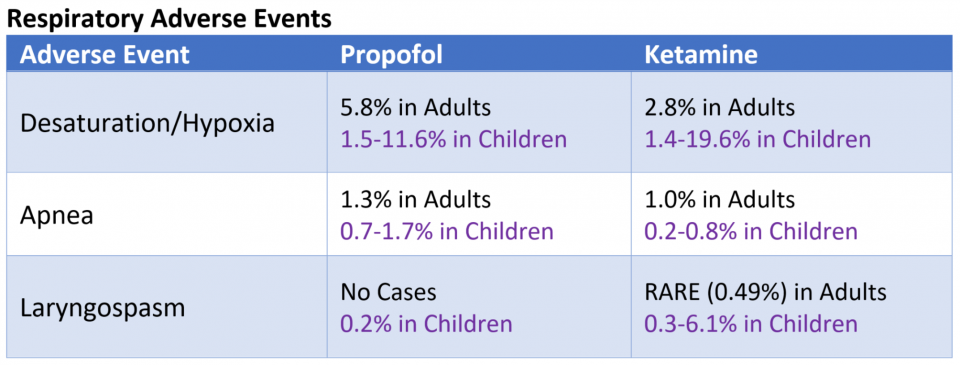
These papers show that there is an increased rate of hypoxia/desaturation and apnea in sedations with Propofol compared to those with Ketamine. However, this is not a patient-centered outcome. In the vast majority of cases, desaturation was transient requiring only supplemental O2 and/or airway repositioning.
In the adult cohort, only 2 patients required intubation. One patient was intubated following aspiration. The other was an asthmatic who was intubated for apnea, but subsequently self-extubated ~30min later.
In the pediatric cohort, a small subset of patients (<1%) required bag mask ventilation. Endotracheal intubation was exceedingly rare and documented cases were typically in sicker patients (ASA ≥ III) and in settings outside the ED (i.e. endoscopy).
Although there may be a statistical difference between the rates of respiratory adverse events in Propofol vs Ketamine sedations, we don’t believe that this difference is clinically significant. The overwhelming majority of desaturation episodes resolve with supplemental O2, airway repositioning, or bag-mask-ventilation. At the end of the day, patients likely do not care that they received these interventions. If we have administered sedation properly, the patient will be unaware anyways. Patients likely only care if they end up intubated, and thankfully that is exceedingly rare.
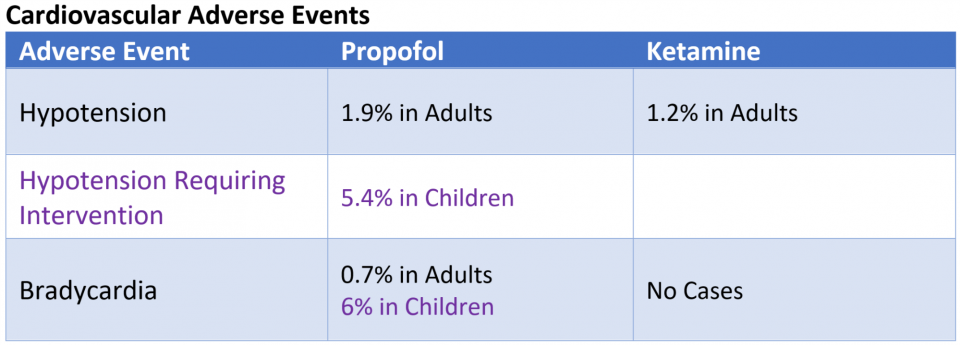
These data show an increased rate of cardiovascular adverse events associated with Propofol sedations compared to Ketamine sedations. Again, these outcomes are not patient-centered. The overwhelming majority of these adverse events were transient. Fluid bolus was the ONLY intervention required in these patients. Invariably, they did not require vasopressors, inotropes, or pacing.
Given that these patients already had an IV for their sedation, I doubt that they would care if they received a fluid bolus during their ED stay. Thus, while a statistical difference may exist, I would argue that there is no clinical relevance to this difference in healthy patients.
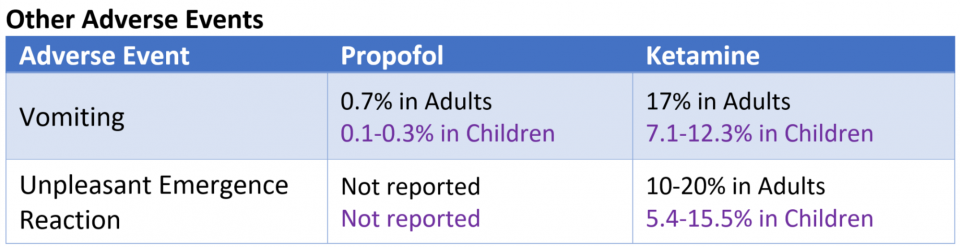
While there seems to be more intra-sedation events with Propofol compared to Ketamine, Ketamine seems to be associated with more post-sedation events. Patients undergoing sedation with Ketamine have significantly more vomiting and emergence reactions compared to those sedated with Propofol.
While patients may not care whether they get supplemental O2 or IV fluids, they do care if they wake up in psychological distress or if they vomit.
While up to 1 in 5 patients sedated with Ketamine experience an unpleasant emergence reaction, few are severely distressing. Thankfully, the incidence of both emergence delirium and vomiting seen in Ketamine sedations can be reduced with targeted pretreatment.
- Vomiting seen with Ketamine sedations rarely occurs during sedation, it typically occurs during the recovery period. Pretreatment with Zofran can reduce the rate of post-sedation vomiting6
- Pretreatment with midazolam (0.05mg/kg IV) can reduce the rate of emergence reactions7
Risk Factors for Adverse Events in Emergency Department Procedural Sedation for Children. – Bhatt et al. JAMA Pediatrics (2017)8
This is the most relevant paper published since the data presented above. This study was a prospective, multicenter cohort study in 6 Canadian Pediatric Emergency Departments.
- 6295 total sedations with wide variety of sedating agents
- 970 Propofol-based sedations
- 4162 Ketamine-based sedations
- Propofol-based sedations = Propofol was the primary sedating agent (includes Propofol alone & Propofol/Fentanyl)
- Ketamine-based sedations = Ketamine was the primary sedating agent (includes Ketamine alone and Ketamine/Midazolam)
In this study, the authors found the following adverse event rates:
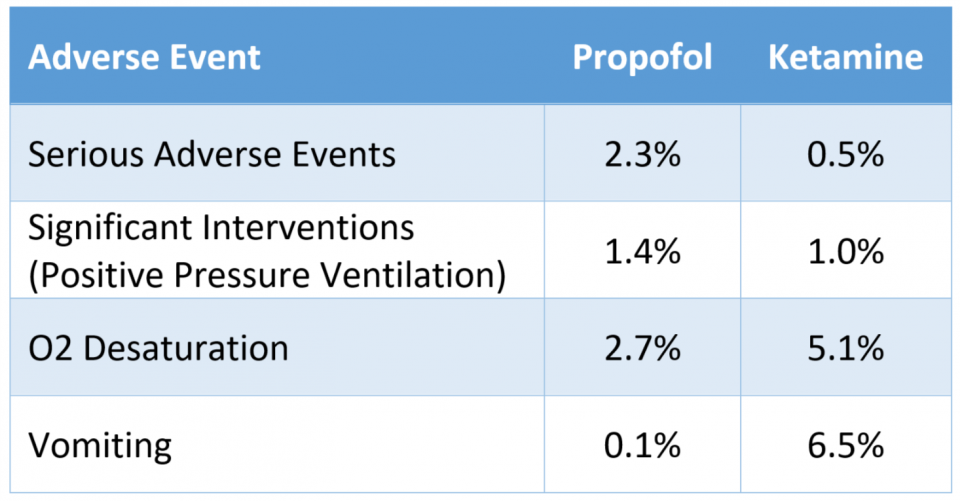
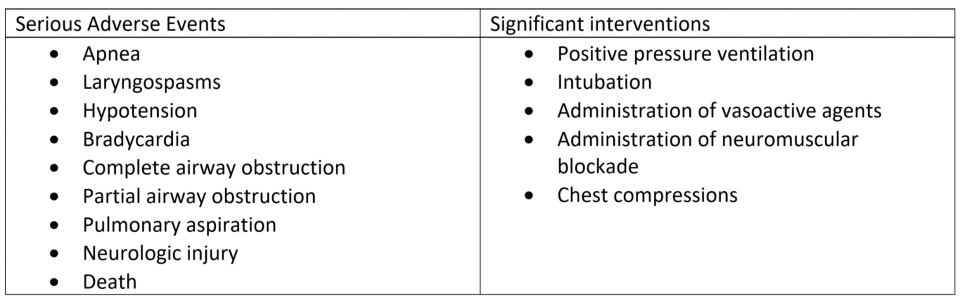
Like the papers before it, this study showed Propofol-based sedations to be associated with an increased rate of serious adverse events compared to Ketamine-based sedations.
While there was a 1.8% difference in the rate of serious adverse events, the difference in the rate of significant interventions was only 0.4%. Furthermore, the ONLY “significant intervention” that any patient required in this study was positive pressure ventilation.
Once again, while the authors may have demonstrated a difference in adverse event rates, this difference is unlikely to be clinically relevant.
Summary – Adverse Events: Ketamine vs Propofol
In healthy patients undergoing brief procedural sedation in the ED, there is unlikely to be a clinically significant difference between choosing Propofol vs. Ketamine as the primary sedating agent.
Propofol-based sedations may have increased rates of intra-sedation events such as hypoxia and hypotension compared to ketamine.
- These events almost never require aggressive intervention
- While there may be a statistical difference in the studies, it is unlikely to be of any clinical relevance in healthy patients
Ketamine-based sedations may have increased rates of emesis and unpleasant emergence reactions.
- Emesis is rare intra-sedation, mostly occurring during the recovery phase
- The majority of emergence agitation is not severely distressing to the patient
- Rates of emergence reaction and emesis may be reduced with benzodiazepine and ondansetron pretreatment, respectively
Caveats
The data presented from the studies mentioned come from patient populations that are heavily skewed towards healthy (ASA I & II) patients. Providers should take into consideration patient factors and the pharmacologic properties of sedating agents when choosing a sedating agent for higher risk patients.
Below are a few situations (amongst many) in which providers may prefer Ketamine over Propofol:
- Concerns about ability to bag-mask ventilate (as Ketamine preserves respiratory drive)
- Severe LV dysfunction (Patients may not be able to tolerate negative inotropy of Propofol)
- Hemodynamic instability (Negative inotropy and vasodilatory effects of Propofol are unfavourable)
Ketamine vs Propofol – ED Length of Stay
In the previous section, I convinced you that in healthy patients undergoing brief procedural sedation in the ED, there is unlikely any clinically significant differences in adverse events in patients undergoing sedation with Ketamine and Propofol. Given that both are safe in this patient population, we will explore whether there is a difference in ED length of stay (LOS) between sedations using Ketamine vs. Propofol
The NICE Guidelines for Sedation in Children and Young People from the UK published in 2010 addressed the following issue9:
“For children and young people under the age of 19 undergoing painful procedures, is Propofol effective and safe for sedation in comparison with Ketamine?
Both Ketamine and Propofol are well tolerated and effective drugs suitable for painful procedures. Propofol has a tendency to cause deep sedation and anesthesia in which airway and breathing may need an intervention or support. Ketamine has few appreciable effects on the airway and breathing but [Ketamine] has longer recovery time than Propofol and causes vomiting.”
The guideline clearly identifies longer recovery times as a downside to Ketamine sedations when compared to Propofol. However, they do not provide any references/citations to support this claim.
Wanting to know if this translated to a significant difference in clinical practice, we took a look at the literature. For the studies that we will present below, it is important to understand two key terms:
- Recovery Time = Time from when the last dose of medication was given to when the patient returned to their baseline mental status
- Total Sedation Time = Time from when the first dose of medication was given to when the patient returned to their mental status baseline
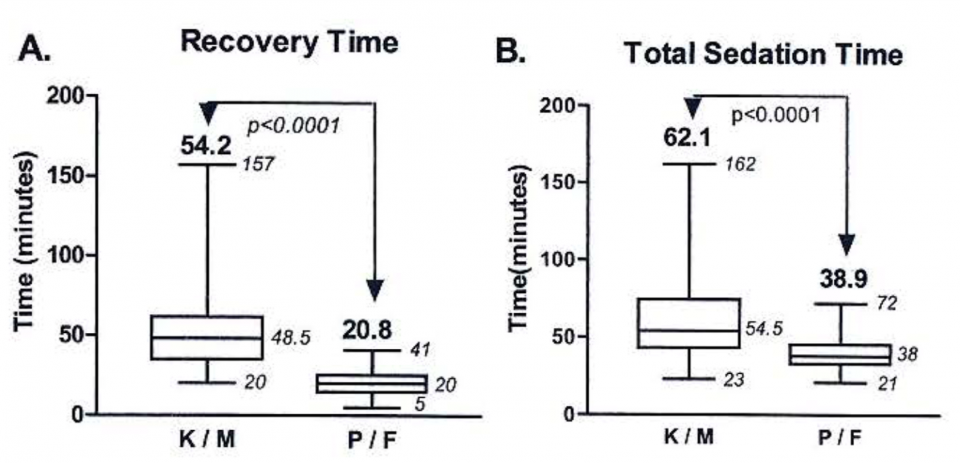
Comparison of propofol/fentanyl versus ketamine/midazolam for brief orthopedic procedural sedation in a pediatric emergency department. – Godambe et al. Pediatrics (2003) 10
Prospective partially blinded, non-randomized study in a single Pediatric Emergency Department
- 113 Patients undergoing sedation for orthopedic reductions
- 54 Ketamine/Midazolam
- 59 Propofol/Fentanyl
- Difference in Recovery time (K/M – P/F) = 33.4 minutes
- Difference in Total Sedation Time (K/M – P/F) = 23.2 minutes
Randomized clinical trial of propofol versus ketamine for procedural sedation in the emergency department. – Miner et al. Academic Emergency Medicine (2010)11
Prospective single-center randomized, non-blinded trial
- 97 adults undergoing procedural sedation in the Emergency Department
- 50 sedations with Propofol
- 47 sedations with Ketamine
Median recovery time was shorter in the Propofol group compared to the Ketamine group
- Propofol – 5 minutes
- Ketamine – 14 minutes
- Difference – 9.38 minutes
Procedural sedation with propofol for painful orthopaedic manipulation in the emergency department expedites patient management compared with a midazolam/ketamine regimen: a randomized prospective study. – Uri et al. Journal of Bone and Joint Surgery, American (2011)12
Prospective, randomized, single-blinded, single-center trial
- 60 Patients undergoing procedural sedation for Orthopedic reductions in the ED
- 30 sedations with Propofol
- 30 sedations with Ketamine and Midazolam
Limitations
All three studies presented above were single-centre studies with a small number of included patients. All were either non-blinded or partially blinded. This puts the studies at risk for bias and limits potential generalizability.
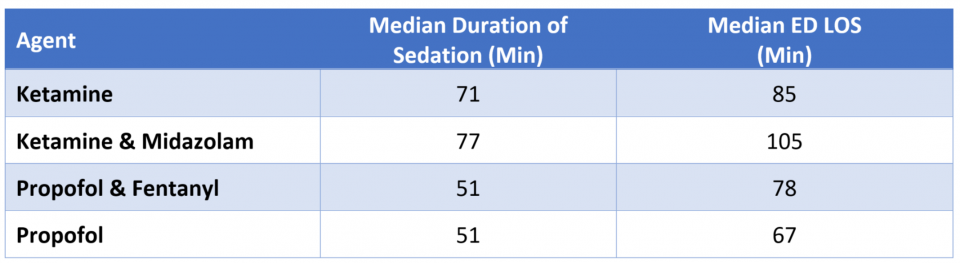
Risk Factors for Adverse Events in Emergency Department Procedural Sedation for Children. – Bhatt et al. JAMA Pediatrics (2017)8
This is the most relevant paper published since the data presented above. This study was a prospective, multicenter cohort study in 6 Canadian Pediatric Emergency Departments.
- 6295 total sedations with wide variety of sedating agents
- 3916 Ketamine
- 246 Ketamine & Midazolam
- 726 Propofol & Fentanyl
- 244 Propofol
Since this was not a randomized control trial and thus did not have a specific dosing protocol, it is important to examine the doses used in sedation to ensure that they are similar to what we would use.
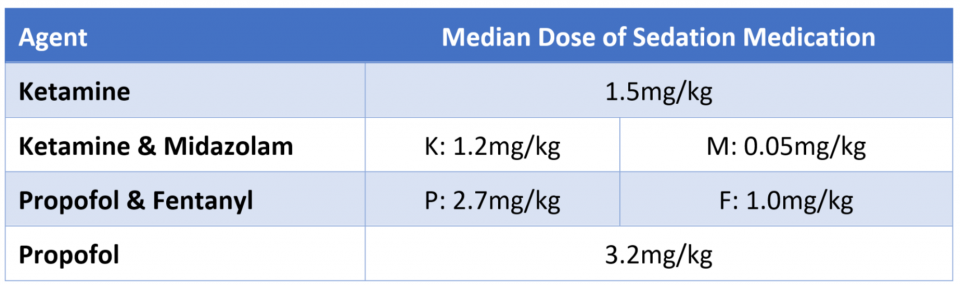
The median doses used in the study are reasonable and comparable to doses that we would use in Pediatric sedations.
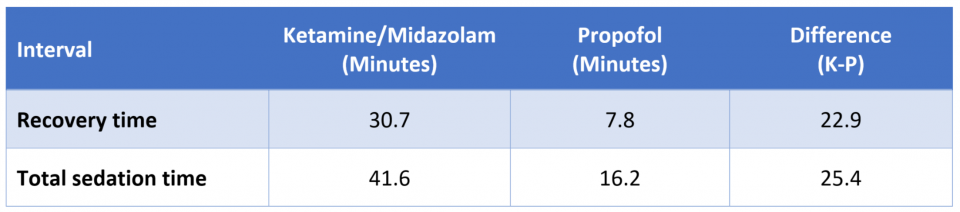
The authors found a longer sedation time in patients receiving Ketamine-based sedations compared to those receiving Propofol-based sedations. Furthermore, this difference translated to longer lengths of stay in the Emergency Department.
Summary – ED Length of Stay: Ketamine vs Propofol
Below is a summary of the results of the 4 papers we presented in this section.
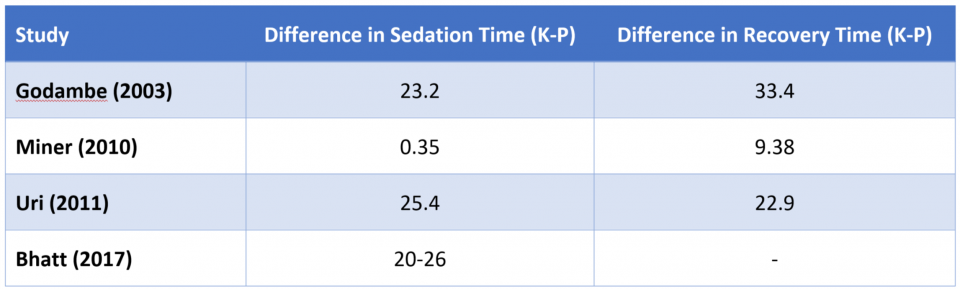
Each one of these papers has their own set of limitations, and while the differences in sedation and recovery times are variable, all available ED literature suggests that sedations with Propofol are associated with shorter recovery/sedation times compared to Ketamine. Furthermore, the Bhatt et al. paper provides compelling data that these shorter sedation times translates to shorter lengths of stay in the ED for those patients.
Is this 10-20 minute difference clinically significant? It depends on where you practice and what the setup is in your Emergency Department. At the site where we train, there are no dedicated rooms for procedural sedation. Patients requiring procedural sedation must be moved to a bed with cardiac monitoring and a high level of nursing care. They remain there until they return to their baseline mental status. In a busy Canadian ED like our own, there are days where monitored beds are a precious resource. We may only save 10-20 minutes on each sedation, but I would argue that those minutes matter. Procedural sedation is something we do very often and the cumulative time saved likely makes a big difference in terms of cost savings over time and improved resource utilization.
Conclusion
In healthy patients undergoing brief procedural sedation in the ED, there does not appear to be a clinically significant difference between choosing Propofol vs. Ketamine as the primary sedating agent in terms of adverse events. Although limited, all available Emergency Department based studies suggest reduced sedation times with Propofol-based sedations, which translates to reduced ED length of stay. In our ED setting where we do not have a dedicated sedation room, sedation is a resource intensive endeavour requiring both a bed with cardiac monitoring and increased nursing care. Thus, in our setting, perhaps one may consider Propofol as the preferred agent in healthy patients undergoing brief procedural sedation.
References
- Anesthesiologists A society for. Continuum of Depth of Sedation: Definition of General Anesthesia and Levels of Sedation/Analgesia. 2014:1-2.
- Birdi T, Sullivan P. Ottawa Anesthesia Primer.
- Strayer R. The Ketamine Brain Continuum – emupdates. https://emupdates.com/the-ketamine-brain-continuum/. Published 2013. Accessed October 20, 2018.
- Bellolio MF, Gilani WI, Barrionuevo P, et al. Incidence of Adverse Events in Adults Undergoing Procedural Sedation in the Emergency Department: A Systematic Review and Meta-analysis. Acad Emerg Med. 2016;23(2):119-134. doi:10.1111/acem.12875.
- Hartling L, Milne A, Foisy M, et al. What Works and What’s Safe in Pediatric Emergency Procedural Sedation: An Overview of Reviews. Acad Emerg Med. 2016;23(5):519-530. doi:10.1111/acem.12938.
- Langston WT, Wathen JE, Roback MG, Bajaj L. Effect of Ondansetron on the Incidence of Vomiting Associated With Ketamine Sedation in Children: A Double-Blind, Randomized, Placebo-Controlled Trial. Ann Emerg Med. 2008;52(1):30-34. doi:10.1016/j.annemergmed.2008.01.326.
- Sener S, Eken C, Schultz CH, Serinken M, Ozsarac M. Ketamine With and Without Midazolam for Emergency Department Sedation in Adults: A Randomized Controlled Trial. Ann Emerg Med. 2011;57(2):109-114.e2. doi:10.1016/j.annemergmed.2010.09.010.
- Bhatt M, Johnson DW, Chan J, et al. Risk factors for adverse events in emergency department procedural sedation for children. JAMA Pediatr. 2017;171(10):957-964. doi:10.1001/jamapediatrics.2017.2135.
- NICE. Sedation in children and young people. 2010;(December).
- Godambe SA, Elliot V, Matheny D, Pershad J. Comparison of Propofol/Fentanyl Versus Ketamine/Midazolam for Brief Orthopedic Procedural Sedation in a Pediatric Emergency Department. Pediatrics. 2003;112(1):116-123. doi:10.1542/peds.112.1.116.
- Miner JR, Gray RO, Bahr J, Patel R, McGill JW. Randomized clinical trial of propofol versus ketamine for procedural sedation in the emergency department. Acad Emerg Med. 2010;17(6):604-611. doi:10.1111/j.1553-2712.2010.00776.x.
- Uri O, Behrbalk E, Haim A, Kaufman E, Halpern P. Procedural sedation with propofol for painful orthopaedic manipulation in the emergency department expedites patient management compared with a midazolam/ketamine regimen: A randomized prospective study. J Bone Jt Surg – Ser A. 2011;93(24):2255-2262. doi:10.2106/JBJS.J.01307.

