
For other POCUS focused cases please see our ultrasound archives
Case
The next chart you pick up is for an 87 year-old female brought in by EMS from her nursing home for agitation and vomiting. She is afebrile and her vital signs are normal. She has a past medical history of advanced dementia and a remote oophorectomy for ovarian cancer.
Documents sent in from the nursing home state that she’s been increasingly agitated over the past week. A few days ago, a urine dip performed in the nursing home was positive, so she was started on appropriate antibiotic therapy. Despite this, she has become more agitated today and took a swing at one of the nursing staff. On review of systems, you identify that the patient has 24-48 hours of increased abdominal girth and nausea/vomiting (3-4 times today, no blood). It is unclear whether there have been any recent changes in bowel movements or flatus. No reported falls/trauma/etc. Current medications include dimenhydrinate PRN, TMP-SMX, and donepezil. She has no drug allergies.
Your physical examination yields a slightly agitated, confused patient. Screening neurological, cardiorespiratory, MSK, and dermatologic exams are within normal limits. Her abdominal exam yields a moderately distended abdomen with mild epigastric tenderness and no peritoneal signs.
At this point, what is your differential diagnosis?
Information is significantly lacking, so we need to cast a broad net here. Essentially, the patient is presenting with agitated delirium NYD. A commonly used mnemonic for delirium DDx is “DIMES”
D – drugs (dimenhydrinate, withdrawal)
I – infection (pneumonia, GI, UTI, skin and soft tissue), ischemia (MI, gut)
M – metabolic (fluid/electrolyte abnormalities, acidosis)
E – environmental
S – structural (stroke, urinary retention, volvulus, bowel obstruction)
Any bedside tests you would like to perform?
POC Glucose – normal
ECG – shows normal sinus rhythm
Portable CXR – shows no significant abnormalities
What about POCUS?
In this elderly, confused lady presenting with agitated delirium, vomiting, and abdominal distension, we can assess for a number of possible etiologies using POCUS:
- Lung scan checking for focal or diffuse B-lines
- AAA scan
- FAST looking for abdominal free fluid/ascites
- Renal/bladder scan checking for urinary retention or hydronephrosis
- Gallbladder scan checking for stones and signs of cholecystitis
POCUS
You put the probe on the abdomen over the right and left upper quadrants and this is what you see:
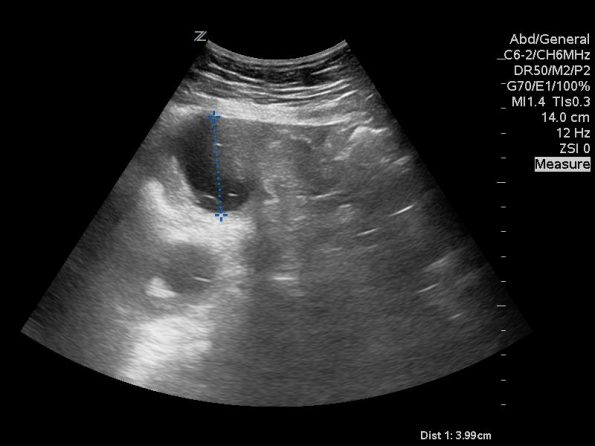
What is the most likely diagnosis?
Small bowel obstruction. Based on this lady’s POCUS, an NG was inserted, a surgical consult was obtained, and advanced imaging was pursued. CT abdomen/pelvis later showed moderate distension of a segment of mid to distal small bowel, possibly due to adhesions in the pelvis. Distal small bowel demonstrates fluid and distension, suggesting partial distal SBO.
POCUS for SBO:
Indications:
- Acute abdominal pain
- Peritonitis
- Abdominal distension or mass
- Persistent nausea/vomiting
Why POCUS?
- Immediate, convenient bedside test
- No ionizing radiation
- Helpful in low-resource settings
- Abdominal/KUB diagnostic accuracy equivocal (40-60%)1 — See Dr. Krishan Yadav’s Grand Rounds “Abdominal X-rays, What’s the Point?” for more information.
- Recent studies of ED provider-performed POCUS for SBO
- Recent review articles and meta analyses show favourable diagnostic characteristics for ED provider-performed POCUS (with variable level of training)2,3
- Sensitivity 94-100%
- Specificity 81-100%
- LR+ 21.1
- LR- 0.08
- Recent review articles and meta analyses show favourable diagnostic characteristics for ED provider-performed POCUS (with variable level of training)2,3
Technique:
- Generally, patient supine, but can use lateral decubitus
- Curvilinear probe, indicator to patients right, depth of 12-18cm
- Image in 4 spots: epigastric, L pericolic gutter, R pericolic gutter, suprapubic
- If nothing found, consider scanning everything

Typical findings:
- Dilated bowel loops (>25mm)
- Take at 90 degrees to bowel wall (avoid oblique measurements)
- Increased intraluminal fluid
- Alternating peristalsis (initially hyper, then hypo)
- “To and fro” movement of intraluminal contents
- Later on in obstruction, contents may become hyperechoic
- “Keyboard sign” in jejunum – where plica become dilated in fixed loop of bowel, take on keyboard appearance in longitudinal views
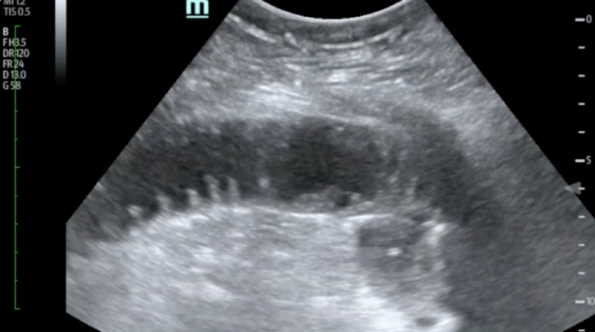
Reproduced from Journal of Teaching in Emergency Medicine
- “Tanga sign” – Circumscribed free fluid between bowel loops that should raise concern for bowel strangulation
- According to Wikipedia, the Tanga is “a pair of briefs consisting of small panels connected by strings at the sides. There are tanga briefs both for men and for women. The style and the word comes from Brazil.”
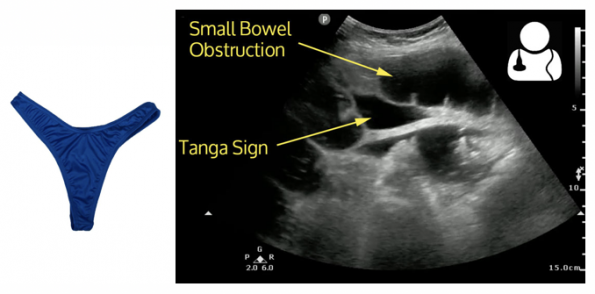
Reproduced from Ultrasound of the Week Cast #20
Limitations:
- Big/gassy patients
- Operator
Clinical application:
- If positive
- Consider CT if the cause of obstruction is not readily evident or concern for bowel ischemia
- Consider emergent surgical
- Consider urgent NG placement
- If equivocal
- Bloodwork
- Consider other advanced imaging
POCUS Fellow Commentary
POCUS has great value in the diagnosis of SBO in the emergency department and is by no means an technically challenging scan. Abdominal CT is often quoted in the literature as highly sensitive and specific (sensitivity 92-94%, specificity 94-96%) for the diagnosis of SBO however takes time, money, may not always be available and increases the patient’s exposure to radiation 4,5. Abdominal ultrasound has an accuracy around 50-92% and, in most cases, can be akin to “flipping a coin” to diagnose SBO2. Radiology performed ultrasound is an accepted alternative in pregnant and pediatric patients with sensitivity of around 83% and specificity around 100% 4. POCUS for SBO does not currently have robust, high quality evidence to support its use however does have some observational data indicating it efficacy.
A 2017 meta-analysis by Gottleib et al, looked at 11 observational studies including 1178 patients examining the accuracy of ultrasound in the detection of SBO6. Unfortunately, only 3 studies were ED based and in a majority of studies the US was not performed by an emergency physician. Additionally, each study did not use a standardized protocol or gold standard. Nonetheless, they found a sensitivity of 92.4% and specificity of 96.6%6. When they looked at ED only studies the numbers did not change much (sensitivity 93%, specificity 96%). Unfortunately, they did not have enough data to complete a subgroup analysis based on provider completing the US.
Can emergency physicians perform POCUS to accurately detect SBO?
The answer to this seems to be yes however based on two small studies. Unluer et al, performed a comparison between EM resident performed US and radiology performed US for SBO7. The EM residents underwent 6 hours of training prior to recruitment. They recruited 174 patients who underwent POCUS, radiology performed US and management at the discretion of the treating clinician. Gold standard was surgical pathology, CT or benign clinical course when telephoned 1 month later. POCUS was found to have a sensitivity 97.7% and specificity of 92.7% compared to radiology performed US at 88.4% and 100% respectively7. Their conclusion was that POCUS can be used in the ED with a high degree of accuracy7.
Jang et al, in 2010, looked at a convenience sample of 76 patients who had POCUS for SBO performed by EM residents with 10 minutes of prior training using CT as the gold standard1. They found that dilated bowel loops had a sensitivity of 91% (75-98%) and specificity of 84% (69-93%)1. In contrast, AXR had a sensitivity of 46.2% (20.4 – 73.9%) and specificity of 66.7% (48.9 – 80.9%)1. Their conclusion was that POCUS performed better than AXR and is easy to learn with most operators showing proficiency after 10-20 minutes1.
How to diagnose SBO using POCUS.
There is no set protocol however most resources will suggest looking for dilated loops of bowel over 25 mm and signs of abnormal peristalsis in 2 or more quadrants of the abdomen (epigastrium, right and left paracolic gutters and suprapubically). Additional POCUS findings are listed above. Pourmand et al, conducted a review of the literature in 2018 and found that dilated loops seemed to be consistently the most sensitive and specific marker for SBO with abnormal peristalsis increasing the test characteristics2. They suggest that noting dilated loops is essential in the diagnosis while the other findings only strengthen your argument2.
The use of POCUS in the end will depend on your pre-test probability and suspected etiology. The best use is in patients with high pre-test probability and known etiologies (ex. hernia, adhesions). In this scenario, POCUS allows you to rule in the diagnosis of SBO, initiate earlier management and decrease that patient’s length of stay in the ED. However, caution using POCUS as a rule out test in patients with high clinical probability as the sensitivity of the test approaches the low 90% in some studies. At the end of the day, POCUS is another tool in your armamentarium to improve the care for these patients in the ED.
Commentary by Dr. Rob Suttie, PGY4 and EM Ottawa POCUS Fellow 2018-2019
- Jang, T. B., Schindler, D. & Kaji, A. H. Bedside ultrasonography for the detection of small bowel obstruction in the emergency department. Emerg. Med. J. 28, 676–678 (2011).
- Pourmand, A., Dimbil, U., Drake, A. & Shokoohi, H. The Accuracy of Point-of-Care Ultrasound in Detecting Small Bowel Obstruction in Emergency Department. Emerg. Med. Int. 2018, 1–5 (2018).
- Long, B. & April, M. D. What Is the Diagnostic Performance of Ultrasonography to Diagnose Small Bowel Obstruction? Ann. Emerg. Med. 72, 312–313 (2017).
- Mallo, R., Salem, L., Lalani, T. and Flum, D. (2005). Computed Tomography Diagnosis of Ischemia and Complete Obstruction in Small Bowel Obstruction: A Systematic Review. Journal of Gastrointestinal Surgery, 9(5), pp.690-694.
- Rami Reddy, S. and Cappell, M. (2017). A Systematic Review of the Clinical Presentation, Diagnosis, and Treatment of Small Bowel Obstruction. Current Gastroenterology Reports, 19(6).
- Gottlieb, M., Peksa, G., Pandurangadu, A., Nakitende, D., Takhar, S. and Seethala, R. (2018). Utilization of ultrasound for the evaluation of small bowel obstruction: A systematic review and meta-analysis. The American Journal of Emergency Medicine, 36(2), pp.234-242.
- Ünlüer, E., Yavaşi, Ö., Eroğlu, O., Yilmaz, C. and Akarca, F. (2010). Ultrasonography by emergency medicine and radiology residents for the diagnosis of small bowel obstruction. European Journal of Emergency Medicine, 17(5), pp.260-264.

