

Care of the Elderly is an ever-growing, important, and prevalent part of an Emergency Physician’s repertoire of skills. With increasing numbers of elderly patients presenting to EDs across Canada, we look to discuss the issue of polypharmacy, prescribing, and deprescribing for this high risk population in the ED. After reading this post, we hope you will:
- Understand polypharmacy and deprescribing,
- Develop a strategy to identify high risk medications
- Learn a framework to guide deprescribing in the ED
For more information regarding Frailty, Falls and Pain Management in the Elderly, please see Dr. Ariel Hendin’s post here.
Why is Polypharmacy and Deprescribing in the ED Important?
Polypharmacy: multiple definitions exist, but the one I prefer is the concurrent use of 5 or more medications (including both prescription and non-prescription products). Polypharmacy exists when the theoretical benefits of multiple medications is outweighed by the negative effects of the sheer number of medications. Polypharmacy is not solely about the number of medications used, but also about the effectiveness, utility, and potential harm of each medication, both individually and in combination.
Prevalence of polypharmacy (CIHI, 2016):
- >66% of Canadians over 65 take at least 5 different prescription medications
- 25% of those over 65 years take more than 10 medications, and
- >40% of those over 85 years take more than 10 medications
Risks of polypharmacy:
- Drug-drug interactions
- Decreased compliance
- Increased chance of medication errors
- Associated with increased mortality, even when adjusted for sociodemographic and comorbidity factors
- Impaired ability to prescribe new medications due to concerns about the above
It is likely that many of the medications that contribute to polypharmacy in older people are historical remnants of conditions and issues gone by, whose treatment requirements and goals are now different, and have not been regularly re-assessed for a variety of reasons (e.g. changing care providers, loss to follow-up, provider hesitancy to stop medications in a ‘stable’ patient, lack of primary care provider, etc.). It is also likely that an appropriately counselled older person would be willing to stop medications, as found by Sirois and colleagues in 2017, when they found that over 70% of older Canadians were willing to discontinue medications with a doctor’s recommendation.
Deprescribing: the planned and supervised process of reducing or stopping medications that may no longer be of benefit or may be causing harm. The goal is to reduce medication burden and harm, while maintaining or improving quality of life.
Across all Canadian ED’s, adults over the age of 65 make up over 20% of all visits, impacting EDs in a big way, as patients over the age of 65 have an ED length of stay twice as long as the national average (CIHI 2015). They require more imaging, more labs, and more consultation services than other groups (Lantham 2014).
How do I identify High Risk Medications in the ED?
AGS BEERS Criteria
There are many different resources, from literature reviews, food and drug administration reports, and clinical care guidelines which can be used to assist in identifying high risk medications in older people. One of the most well-known is the American Geriatrics Society’s Beers Criteria (2015 update). A list of medications whose use is deemed potentially inappropriate in older people, where harm is thought to commonly outweigh the benefit. The Beers Criteria are not meant to be punitive, in other words, it is not that the medications listed are never to used; it is however meant to flag medications we should avoid when other safer alternatives exist, and to closely monitor when the use of one of these higher risk medications is required.
In Canada, potentially inappropriate medication use is common. In 2016, the CIHI reported that over 49 percent of older people in Canada were on at least 1 potentially inappropriate medication. These medications are associated with significant costs. In 2016, Morgan and colleagues used data from the National Prescription Drug Utilization Information System to estimate the cost of inappropriate medication prescribing in Canada (excl. Quebec). They found the cost of potentially inappropriate medication use outside of the hospital to be $419 million annually in Canada, and the cost of treating the harmful effects of these medications at $1.4 billion every year.
STOPP/START Criteria
The STOPP (Screening Tool of Older Persons’ Prescriptions) and START (Screening Tool to Alert to Right Treatment) criteria were designed and validated as criteria to help prevent the use of potentially inappropriate medicines and prescribing errors, as well as to reduce adverse drug reactions and events (ADRs, ADEs). The criteria were developed in 2008 and updated in 2015 (O’Mahony et al, 2018).
According to the STOPP/START Criteria, the top 10 STOPP Criteria include:
- Long term benzodiazepine use
- Duplicate prescriptions for the same drug class
- Proton pump inhibitor use in peptic ulcer disease at full dose for >8 weeks
- NSAIDS in patients with moderate to severe hypertension
- Long term use of opiods as first line for mild to moderate pain
- Aspirin use without adequate cardiovascular risks
- Warfarin and NSAID use together
- Betablocker use in patients with COPD
- Prolonged use of first generation antihistamines
- NSAID use in patients with CKD
Other useful resources for prescribing and deprescribing include:
- Choosing Wisely Canada (www.choosingwiselycanada.org): the national voice for reducing unnecessary tests and treatments in health care which provides speciality specific guidelines, including emergency medicine.
- Medstopper (www.MedStopper.com): An interactive website where medication lists can be entered, and the plan will generate a list of medications in order of stopping priority based on a complex algorithm of interactions, risks, and harm.
- Anticholinergic Burden Scale (www.ACBCALC.com): allows you to determine the individual and cumulative anticholinergic burden of medication, and can aid in decision making. It even will provide a list of medications in similar classes that have lower anticholinergic impact.
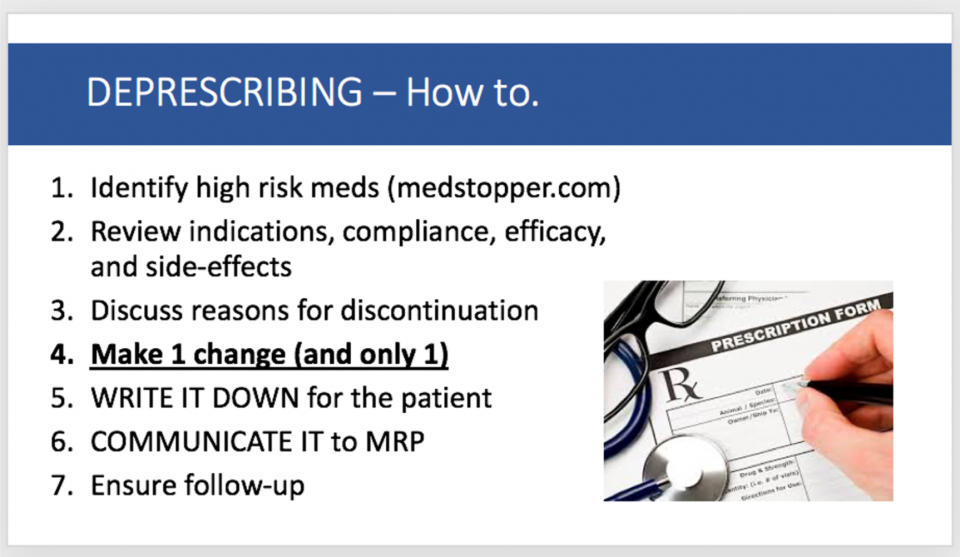
How do I Deprescribe?
References

