

In this post, we will aim to review the literature looking at identifying clinical and historical features that can help differentiate stroke mimics from strokes. We will also discuss the safety of the administration of IV tPA to misdiagnosed stroke mimics. This post will not focus on the recent developments in endovascular therapy for stroke and the implications of this.
Background
Cerebrovascular accidents (CVA), commonly termed “strokes”, are among the top five causes of death and the number one cause of disability in North America (CDC 1999-2009). Current guidelines recommend rapid recognition and potentially aggressive treatment of patients presenting with possible stroke symptoms (Mozzafarian et al., 2015). However, it is not always easy for physicians to correctly identify these symptoms and despite advances in imaging modalities, the diagnosis of stroke and stroke mimics remain largely clinical.
Intravenous (IV) tissue plasminogen activator (tPA) remains one of the mainstays of treatment for acute ischemic stroke. The diagnosis of stroke is time-sensitive, and emergency department (ED) physicians have the difficult task of making this diagnosis in often suboptimal conditions.
Depending on the area of the brain affected, stroke presentations can be incredibly variable, making this an important differential for almost any neurological complaint. Up to 1/3 of strokes diagnosed in the ED are later diagnosed as stroke mimics, and up to 15% of stroke mimics are treated with tPA (Merino 2013). For those working in a referral centre, the literature has found that higher stroke mimic rates are found in larger volume stroke centres (Nguyen & Chang, 2015). Conversely, smaller- volume hospitals are associated with lower rates of stroke mimics.
Stroke – A Quick Review
The American Heart Association / American Stroke Association (AHA/ASA) characterizes stroke as a neurological deficit attributed to an acute focal injury of the central nervous system (CNS) by a vascular cause, including cerebral infarction, intracerebral hemorrhage (ICH), and subarachnoid hemorrhage (SAH). However, some local experts would argue, for simplicity sake, to focus on ischemic stroke (i.e., cerebral infarction) and set aside the hemorrhagic causes as treatment differs greatly. The World Health Organization (WHO) defines stroke as rapidly developing clinical signs of focal (or global) disturbance of cerebral function, lasting more than 24 hours or leading to death, with no apparent cause other than that of vascular origin.
Brain Anatomy
Since strokes symptoms occur within the vascular distribution area of the affected artery, it is important to have a basic understanding of brain anatomy to make an appropriate diagnosis.
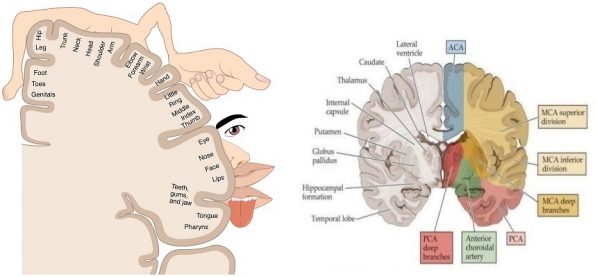
The brain is supplied by 3 main arteries: the anterior, middle, and posterior cerebral arteries. By super-imposing the above 2 images, you can infer which parts of the body will be affected during an ischemic event. From an ED physician perspective, motor and sensory deficits are grossly along the same distribution.
- The anterior cerebral artery (ACA) supplies the basal and medial aspects of the cerebral hemispheres and extends to the anterior two-thirds of the parietal lobe.
- The middle cerebral artery (MCA) feeds the lenticulostriate branches that supply the putamen, part of the anterior limb of the internal capsule, the lentiform nucleus, and the external capsule. The main cortical branches of the middle cerebral artery supply the lateral surfaces of the cerebral cortex from the anterior portion of the frontal lobe to the posterolateral occipital lobe.
- The posterior circulation is smaller and supplies only 20% of the brain. It supplies the brainstem (which is critical for normal consciousness, movement, and sensation), cerebellum, thalamus, auditory and vestibular centers of the ear, medial temporal lobe, and visual occipital cortex.
Anterior Cerebral Artery Stroke
Occlusion of the ACA is uncommon, but when a unilateral occlusion occurs, it can result in: (Tintinalli):
- Altered mentation, impaired judgment and insight
- Paralysis and hypoesthesia of the lower limb contralateral to the lesion
- Leg weakness is more pronounced than arm weakness
- Apraxia or clumsiness in the patient’s gait
- Presence of primitive grasp and suck reflexes on physical examination
- Bowel and bladder incontinence
Middle Cerebral Artery Stroke
The MCA is the most commonly involved vessel in stroke, and presentation can be quite variable, depending on where the lesion is located and which brain hemisphere is dominant. (Remember, in most people, the left hemisphere is dominant). MCA strokes typically present as (Tintinalli):
- Contralateral motor and sensory symptoms, usually worse in the arm and the face
- Facioplegia
- If the dominant hemisphere is involved, can have expressive or receptive aphasia
- If the non-dominant hemisphere is involved, can have hemineglect
- Homonymous hemianopsia and gaze preference toward the affected side may also be seen, regardless of the side of the infarction
Posterior Cerebral Artery Stroke
PCA infarcts cause the widest variety of symptoms and can be the most difficult to diagnose. The most common presenting complaint is a unilateral headache (Brandt et al., 2000). PCA stokes can present with (Tintinalli):
- Homonymous hemianopsia
- Visual field defects
- Memory loss, alexia, inability to recognize objects or colors
- Vertiginous symptoms
Stroke Mimics – What are they?
As you can imagine, since there is no universally accepted definition for stroke, there is even less consensus on a definition for stroke mimics. In very simple terms, a stroke mimic is when someone presents with stroke-like symptoms but is ultimately found not to have a stroke. Do not get confused with the term stroke chameleons, which are patients who present with non-stroke like symptoms, but are ultimately found to have a stroke (another discussion for another day). For a more formal definition, here is one from a clinical review by Nguyen & Chang (2015):
“Heterogeneous group, presenting with acute onset focal neurological deficits that are later found to have nonvascular etiologies ”
An important caveat in the literature that makes defining stroke mimics even more complex is that studies and stroke referral centres will often use different criteria to make the final diagnosis of a stroke mimic. That is, some will diagnose a stroke mimic when the initial plain CT head is negative for ischemia. Other centre will go further in the diagnostic work-up and will only diagnose a stroke mimic once more advanced imaging (e.g. MRI, MRA, CTA, etc.) are negative for ischemia. As you can imagine, these more extensive work-ups are more sensitive in identifying potential ischemic events, and can sometimes result in different conclusions when it comes to identifying common characteristics of mimics or determining common etiologies of stroke mimics. Furthermore, these advanced imaging modalities are not common practice in most hospitals. This adds a lot of heterogeneity to the literature on stroke mimics and can sometimes make conclusions less applicable to routine practices. The goal of this review is to focus on a general approach to thinking about stroke mimics.
Are there reliable features that can help differentiate Stroke from Stroke Mimic?
Now that we know what strokes look like on paper, we can apply this knowledge in the real world. However, as we know, strokes have a wide variety of presentations, and mimics present even more diversely! The question becomes, are there any features that have a higher odds ratio of being diagnostic of mimic?
Looking at the literature
One of the first papers looking at clinical variables that can aid in the diagnosis of stroke mimic is by Libman et al. in 1995 and is still commonly quoted in the literature.
- Published in the American Academy Journal of Neurology
- Study size: 411 patients
- 78 (19%) were diagnosed as stroke mimic, slightly lower percentage compared to more recent studies
- In this study, they were calculating the odds ratios for stroke mimic based on features from the history and from exam findings.
- In this table, a higher number (in red) indicate increase odds for mimic while lower numbers (green) indicate variables that lean towards a diagnosis of stroke
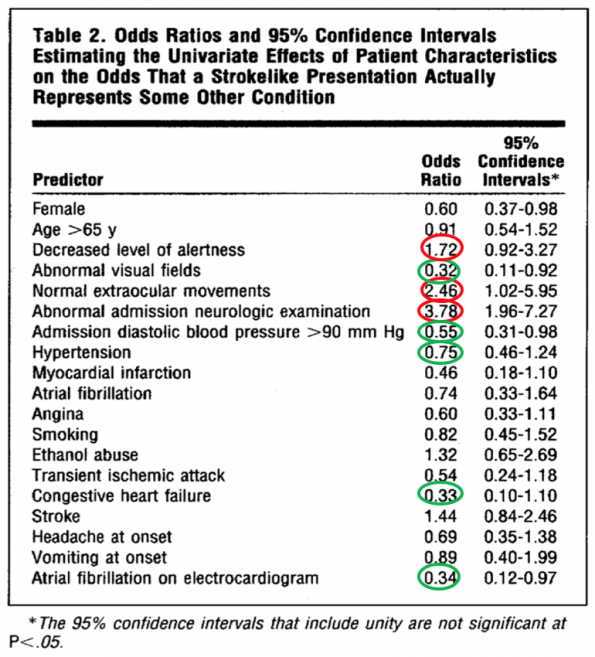
- Overall, none of the ORs were very high, with the highest being 3.78 for an abnormal neurological exam. Ironically enough, this was not found to be statistically significant on univariate analysis because of the large confidence intervals.
- Multivariate analysis showed that only decreased level of consciousness independently predicted the presence of a stroke mimic, and only a history of angina independently predicted a stroke
- Bottom line:
- Findings that were more indicative of mimic:
- Decreased LOC (OR 1.72, CI 0.92 – 3.27)
- Normal eye movements (OR 2.45, CI 1.02 – 5.95)
- Findings that were more indicative of stroke:
- Abnormal visual fields (OR 0.32, CI 1.0 to 0.9)
- Initial diastolic BP greater than 90 mmHg (OR 0.55, CI (0.31 – 0.98)
- Atrial fibrillation on ECG (OR 0.34, CI 0.12-0.97)
- History of angina (OR 0.60, CI 0.33 – 1.11)
- Findings that were more indicative of mimic:
The next study we will review is the Distinguishing Between Stroke and Mimic at the Bedside: The Brain Attack Study by Hand et al. in 2006:
- Published in the journal Stroke
- They looked at the frequency and nature of stroke mimics and aimed to identify the key clinical features that distinguish between stroke and mimic at the bedside.
- A prospective observational study, 336 patients, 350 presentations with a 31% stroke mimic rate
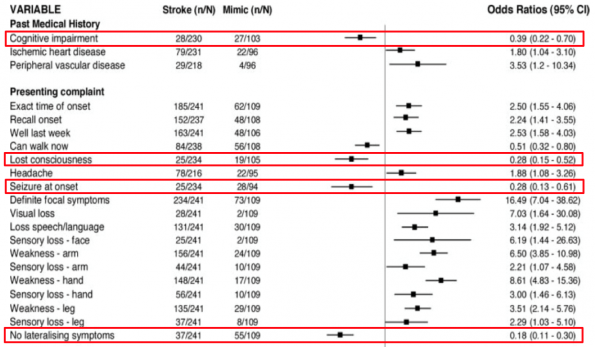
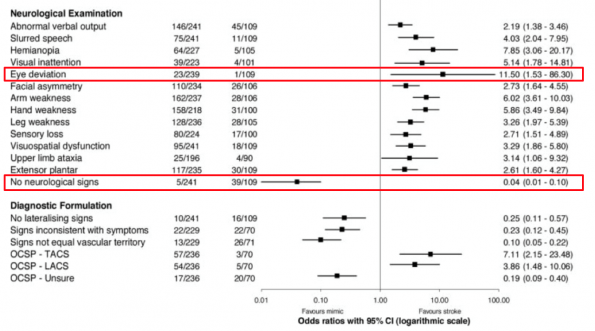
- In this table, ORs less than 1 are predictive of stroke mimic, while those above 1 are predictive of stroke
- Similar to the previous study, lost consciousness was found to be a significant predictor of mimic
- In addition, they found a history of cognitive impairment, seizure at onset, and the absence of lateralizing symptoms were the best predictors of stroke mimic.
- Eye deviation was found to have a significant predictive value for stroke (OR 11.5), but a fairly large CI
- Normal neurological exam was also found to have significant value as a predictor for mimic
In 2013, Merino et al. conducted the largest prospective study aiming to identify predictors and determine the rate of of stroke mimics entitled Predictors of Acute Stroke Mimics in 8187 Patients Referred to a Stroke Service.
- In this study, patients were referred for evaluation of suspected stroke to the National Institutes of Health (NIH) Stroke Program in 2 stroke referral centres in the Washington, DC, metropolitan area. It is the largest prospective study to look at consecutive patients seen by the National Institutes of Health Stroke Program over 10 years
- 30% (2454 patients) stroke mimic rate
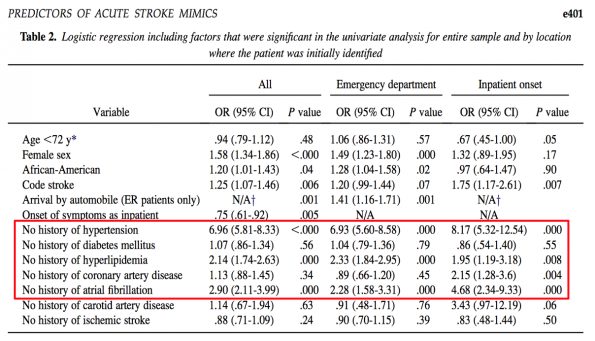
Overall, they found that the absence of hypertension, hyperlipidemia, atrial fibrillation, diabetes, and coronary artery disease were stronger predictors of a stroke mimic than other demographic or clinical features. The more risk factors patients were lacking, the stronger the prediction for stroke mimic. Although this sounds intuitive, now there is some data to confirm it.
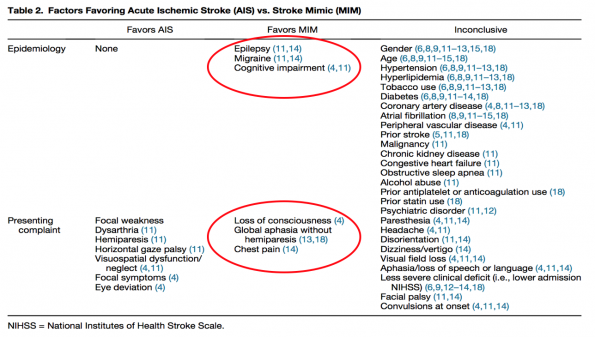
The next 2 review articles by Nguyen & Chang (2015) and Long & Koyfman (2016) essentially reviewed the literature with the aim of presenting strategies for differentiating stroke from mimics. The paper from Long & Koyfman was specifically focused for emergency physicians. Both were published in the Journal of Emergency Medicine with very similar findings.
- Nguyen & Chang (2015)
- They found that stroke mimic patients were younger, more likely female, and were without CV risk factors (atrial fibrillation, hypertension, and hyperlipidemia). However, these findings were inconclusive and can only suggest a diagnosis.
- Interestingly, no study showed smoking history as being predictive of acute ischemic stroke.
- Long & Koyfman (2016)
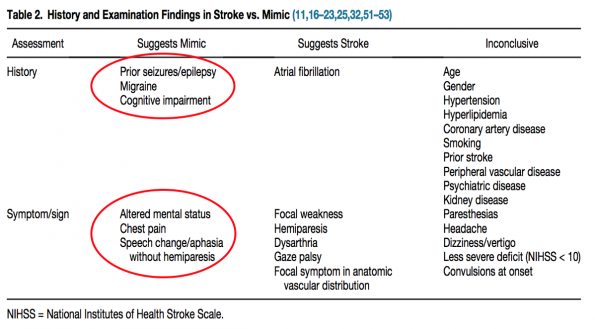
- Two or three focal findings (acute facial paralysis, arm drift/weakness, change in speech) with abrupt onset suggest CVA, whereas the lack of these findings suggest mimic
- In this paper, they comment on the sensitivity of imaging modalities used to aid in the diagnosis of stroke. Non-contrast CT head had the lowest sensitivity, ranging from 12% to 52%. CT angiography in addition to non-contrast head CT increases the sensitivity to over 70%, with the specificity approaching 88%.
- To sum it up:
- A prior history of epilepsy, baseline cognitive impairment, and migraine are more predictive of stroke mimics
- Exam findings of altered/decreased mental status, chest pain, and aphasia without hemiparesis were also found to be predictive of stroke mimics
- Atrial fibrillation was often associated with acute ischemic stroke, but there exists some conflicting evidence on this
The Bottom Line
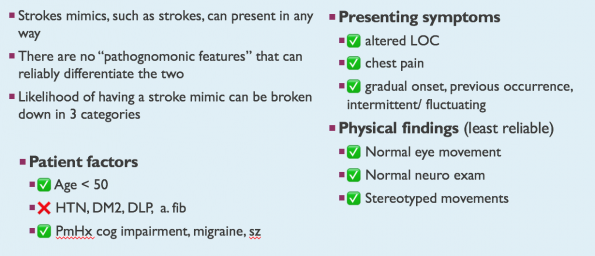
The diagnosis of stroke in the ED remains a difficult one, and the literature does not identify any “key” or “pathognomonic” features that can easily guide the treating physician. At the end of the day, strokes are a complex pathophysiological process with heterogeneous presentations that can ultimately have devastating consequences for patients. For these reasons, ED physicians should have a low index of suspicion for making the diagnosis of ischemic stroke and treating aggressively.
That being said, what the literature does demonstrate are a few features that can help guide physicians when they are suspicious of a stroke mimic. Assessing a patient’s likelihood of stroke mimics can be divided into the following categories:
- Pre-test probability
- Age < 50 years
- The absence of HTN, diabetes, hyperlipidemia, atrial fibrillation
- History of cognitive impairment, migraines, or seizures
- Chief complaint
- Loss or altered level of consciousness
- Chest pain
- Features of chief complaint:
- Symptom onset (fast vs. gradual)
- Previous occurrence? If so, how many times
- Intermittent vs. persistent
- Physical exam findings
- Normal eye movement
- Normal neurological exam
- Stereotyped movements
*Note: aphasia or speech change without hemiparesis has some moderate evidence to be predictive of stroke mimic, but one should be very careful when using this as a data-point in their decision making. It is not as universally accepted as compared to the other features mentioned above.
Remember, these features are simply there to guide a physician when they have a suspicion of stroke mimic and should not be used as a rule or in the absence of clinical judgement. There is a subset of rarer neurological conditions such as CADASIL/CARASIL, Moyamoya disease, Capsular Warning Syndrome, to name a few, that will have atypical presentations and may have features more commonly seen in mimics. The features mentioned above are meant as a guide for common stroke presentations when there is a clinical suspicion of stroke mimic.
Safety of Administering IV tPA to Stroke Mimics
As we mentioned earlier, up to 1/3 of patients diagnosed as “stroke” in the ED will later have their diagnosis changed to “stroke mimic”. About 15% of these stroke mimic patients will receive IV tPA. What happens to these patients? Are the risks of tPA administration to a mimic worth the risk of withholding the treatment for someone with a missed stroke?
Brief overview of the literature
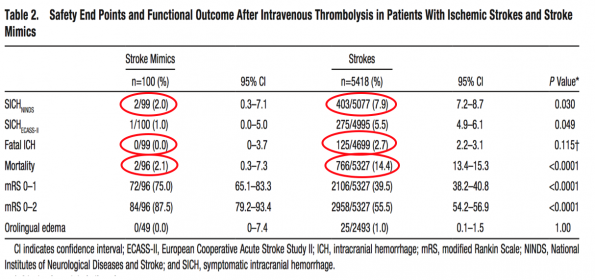
There are multiple studies, including the ones previously mentioned in this blog post, that discuss the safety of tPA administration to stroke mimics. Here, we will review one of the larger and more commonly quoted studies looking specifically at this question by Zinkstok et al. (2013):
- Multicenter observational cohort study containing 5581 patients treated with intravenous thrombolysis for suspected stroke. Stroke mimic was ultimately diagnosed in 100 patients (1.8%).
- 2 patients had symptomatic intracranial hemorrhage (ICH):
- One was a 76-year-old man, finally diagnosed with an epileptic seizure.
- The other patient was a 73-year-old man who presented with an epileptic seizure resulting from a previous post-operative defect.
- Both had a favourable functional recovery.
- No fatal ICH occurred in stroke mimics.
- Mortality in stroke mimics was lower compared with strokes: 2.0% vs. 14.4% (P<0.0001), and the cause of death was not related to the administration of IV tPA.
- Among the 2 stroke mimic patients who died, one had an epileptic seizure with a sudden death 2 weeks before the 3-month follow-up visit. The other died from a brain tumor.
- Among the 2 stroke mimic patients who died, one had an epileptic seizure with a sudden death 2 weeks before the 3-month follow-up visit. The other died from a brain tumor.
- An important limitation in this study is the small percentage of stroke mimic patients treated with tPA (1.8%), which is much lower than other studies. Part of this is attributable to the definition of stroke mimic used in this study, as well as its retrospective design.
Summary
- Overall, the literature strongly supports that giving IV tPA to stroke mimic patients is safe.
- The rate of symptomatic ICH in stroke mimics, which is what we care about, is very low (0–2%). These rates are similar to those found to have symptomatic ICH in patients treated with tPA for acute myocardial infarction.
- No mortality in the literature to date has been caused by ICH following tPA.
- From Nguyen & Chang (2015) literature review
Other factors to consider
- Over-diagnosis can lead to an increase in resource utilization and increased health care costs
- Incorrect labeling can lead to unnecessary testing (with the potential of unnecessary risk or potential complications)
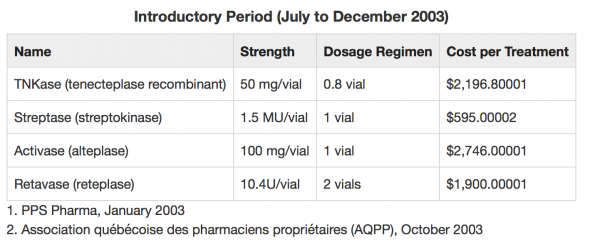
- Cost of IV tPA in Ontario is roughly $2700!
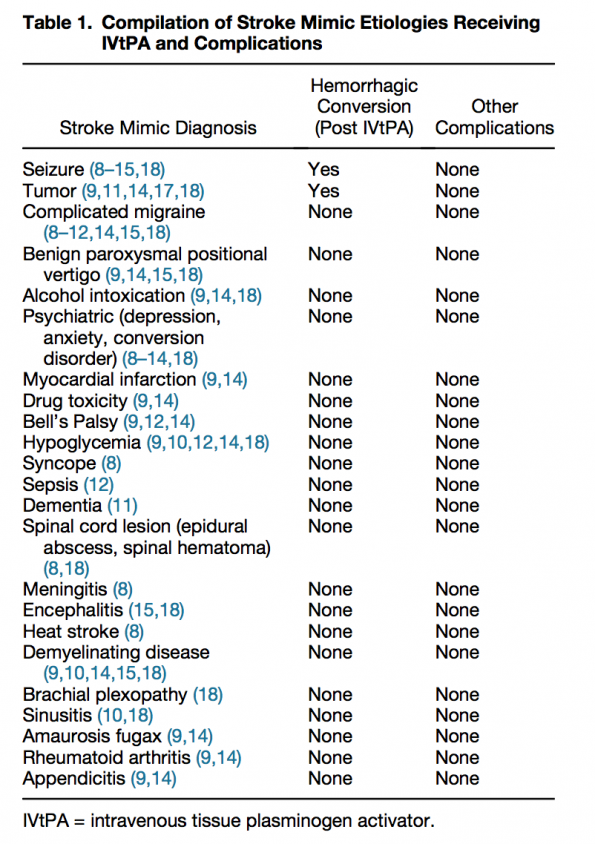
What are common stroke mimics?
One could argue that almost any condition could be considered a stroke mimic. Most studies in the literature review done for this article have their own list. Here are few of the more common etiologies:
- Seizure
- Sepsis
- Toxic / metabolic (includes hypoglycemia)
- Space-occupying lesion (e.g. tumor)
- Syncope/ presyncope
Remember, just because these etiologies are not strokes does not mean they are not critical, and a good clinician will be working through and acting on these differentials even though they may still be considering the diagnosis of stroke. Hypoglycemia can be fatal, and there are numerous case reports of patients presenting with focal neurological findings who were later found to be hypoglycemic. Sepsis can also be life-threatening, and the treatment algorithm is both time-sensitive and quite different from that of stroke. Status epilepticus is a neurological emergency and must be treated aggressively once it is identified.
Approach to the suspected stroke mimic patient
- Ischemic stroke should always be on the top of your differential – “time is brain” and brain is quality of life
- ABCs
- Check the glucose and manage appropriately
- Neurological exam
- Pay attention to eye movements – lateralizing gaze or abnormal eye movements are concerning for stroke
- A normal neurological exam and normal eye movements increases the odds for stroke mimic.
- Look for stereotyped movements (may be subtle) – more common with mimics
- ECG
- Always get one in the ED
- AFib at the time of presentation is strongly correlated with stroke (more so than a history of AFib).
- Metabolic panel
- Looking for metabolic / toxic causes
- Consider ABG/VBG if altered mental status
- CT head (stat) +/- CTA
- If there is a new ischemic lesion, then the diagnosis of stroke can be made.
- Assess for other intracranial pathology (new mass, etc.)
To call or not to call a Code Stroke?
- The most important factor is timing. Has it been more or less than 6 hours since the time of symptom onset (some institutions are still using the 4.5 hour cut-off, check with your stroke referral centre)?
- Strokes are the main cause of impairment and can have devastating consequences to one’s quality of life. Therefore, as ED physicians, it’s something we should strive not to miss.
- In the absence of any clear clinical features that can easily aid in differentiating stroke from stroke mimic, the diagnosis of stroke should remain high on your differential.
- However, if it has been more than 6 hours since time of symptom onset, and you have a high clinical-suspicion of stroke and have ruled-out common stroke mimic etiologies such as hypoglycemia, sepsis, and seizure and have assessed for space-occupying lesions in the brain, consider discussing the case with your local stroke referral centre for suggestions on management.
Conclusions
- Strokes are the number one cause of disability in North America and have a significant impact on a patient’s quality of life and the health care system. Emergency physicians must make a timely diagnosis and treat accordingly.
- Stroke mimics can have a wide array of presentations and can be very difficult to differentiate from an ischemic stroke at the bedside.
- Historical features that can increase the likelihood of stroke mimic are:
- History of: migraines, seizures, or cognitive impairment
- Age < 50
- The absence of HTN, T2DM, AFib, and dyslipidemia
- Presenting features or chief complaint that are more indicative of stroke mimic are:
- Decrease or loss of consciousness
- Chest pain
- Gradual onset of symptoms
- Physical exam findings have been the least reliable in the literature to increase the likelihood of stroke mimic, but some features that have been associated are:
- Normal extraocular movements
- Normal neurological exam
- Stereotyped movements
- When assessing someone with stroke-like symptoms, always rule-out:
- Hypoglycemia
- Sepsis
- Seizure
- IV tissue plasminogen activator (tPA) is given in up to 15% of stroke mimics. The literature supports its safety; the rate of ICH in stroke mimics is less than 2%.
References
- Anathhanam, Sujo, and Ahamad Hassan. “Mimics and Chameleons in Stroke.” Clinical Medicine 17, no. 2 (April 1, 2017): 156–60. https://doi.org/10.7861/clinmedicine.17-2-156.
- Bakradze, Ekaterina, and Ava L. Liberman. “Diagnostic Error in Stroke—Reasons and Proposed Solutions.” Current Atherosclerosis Reports 20, no. 2 (February 2018). https://doi.org/10.1007/s11883-018-0712-3.
- Brandt T, Steinke W, Thie A, et al: Posterior cerebral artery territory infarcts: clinical features, infarct topography, causes and outcome. Multicenter results and a review of the literature. Cerebrovasc Dis 10(3): 170, 2000
- Brunser, Alejandro M., Sergio Illanes, Pablo M. Lavados, Paula Muñoz, Daniel Cárcamo, Arnold Hoppe, Verónica V. Olavarria, Iris Delgado, and Violeta Díaz. “Exclusion Criteria for Intravenous Thrombolysis in Stroke Mimics: An Observational Study.” Journal of Stroke and Cerebrovascular Diseases 22, no. 7 (October 1, 2013): 1140–45. https://doi.org/10.1016/j.jstrokecerebrovasdis.2012.10.019.
- Chalela, Julio A, Chelsea S Kidwell, Lauren M Nentwich, Marie Luby, John A Butman, Andrew M Demchuk, Michael D Hill, Nicholas Patronas, Lawrence Latour, and Steven Warach. “Magnetic Resonance Imaging and Computed Tomography in Emergency Assessment of Patients with Suspected Acute Stroke: A Prospective Comparison” 369 (2007): 6.
- Chang, Jason, Mohamed Teleb, Julian P. Yang, Yazan J. Alderazi, Kristina Chapple, James L. Frey, and Lucas Restrepo. “A Model to Prevent Fibrinolysis in Patients with Stroke Mimics.” Journal of Stroke and Cerebrovascular Diseases 21, no. 8 (November 2012): 839–43. https://doi.org/10.1016/j.jstrokecerebrovasdis.2011.04.018.
- Chang, Jason, Mohamed Teleb, Julian P. Yang, Yazan J. Alderazi, Kristina Chapple, James L. Frey, and Lucas Restrepo. “A Model to Prevent Fibrinolysis in Patients with Stroke Mimics.” Journal of Stroke and Cerebrovascular Diseases 21, no. 8 (November 2012): 839–43. https://doi.org/10.1016/j.jstrokecerebrovasdis.2011.04.018.
- “Conditions That Mimic Stroke in the Emergency Department: Implications for Acute Stroke Trials | JAMA Neurology | JAMA Network.” Accessed November 9, 2018. https://jamanetwork-com.proxy.bib.uottawa.ca/journals/jamaneurology/fullarticle/593727.
- Dawson, Ang, Geoffrey C. Cloud, Anthony C. Pereira, and Barry J. Moynihan. “Stroke Mimic Diagnoses Presenting to a Hyperacute Stroke Unit.” Clinical Medicine 16, no. 5 (October 1, 2016): 423–26. https://doi.org/10.7861/clinmedicine.16-5-423.
- Fernandes, Peter M, William N Whiteley, Simon R Hart, and Rustam Al-Shahi Salman. “Strokes: Mimics and Chameleons.” Practical Neurology 13, no. 1 (February 2013): 21–28. https://doi.org/10.1136/practneurol-2012-000465.
- Fitzpatrick, Tess, and Michael Shamy. “Cohort Study of Features Used by Experts to Diagnose Transient Ischemic Attack,” (pending publication)
- Hand, Peter J., Joseph Kwan, Richard I. Lindley, Martin S. Dennis, and Joanna M. Wardlaw. “Distinguishing Between Stroke and Mimic at the Bedside: The Brain Attack Study.” Stroke 37, no. 3 (March 2006): 769–75. https://doi.org/10.1161/01.STR.0000204041.13466.4c.
- Khan, Nadeem Israr, Shilpa Chaku, Christina Goehl, Laura Endris, Georgia Mueller-Luckey, and Fazeel M. Siddiqui. “Novel Algorithm to Help Identify Stroke Mimics.” Journal of Stroke and Cerebrovascular Diseases 27, no. 3 (March 2018): 703–8. https://doi.org/10.1016/j.jstrokecerebrovasdis.2017.09.067.
- Kose, Ataman, Taylan Inal, Erol Armagan, Ramazan Kıyak, and Aylin B. Demir. “Conditions That Mimic Stroke in Elderly Patients Admitted to the Emergency Department.” Journal of Stroke and Cerebrovascular Diseases 22, no. 8 (November 2013): e522–27. https://doi.org/10.1016/j.jstrokecerebrovasdis.2013.05.029.
- Libam, Richard., Wirkowski, Elzbieta., Alvir, Jose., Rao, Hemanth. “Conditions That Mimic Stroke in the Emergency Department: Implications for Acute Stroke Trials” Arch Neurol 1995;52:1119-1122 https://jamanetwork-com.proxy.bib.uottawa.ca/journals/jamaneurology/fullarticle/593727.
- Liberman, Ava L., and Shyam Prabhakaran. “Stroke Chameleons and Stroke Mimics in the Emergency Department.” Current Neurology and Neuroscience Reports 17, no. 2 (February 2017). https://doi.org/10.1007/s11910-017-0727-0.
- Long, Brit, and Alex Koyfman. “Clinical Mimics: An Emergency Medicine-Focused Review of Stroke Mimics.” The Journal of Emergency Medicine 52, no. 2 (February 2017): 176–83. https://doi.org/10.1016/j.jemermed.2016.09.021.
- Magauran, Brendan G., and Meaghan Nitka. “Stroke Mimics.” Emergency Medicine Clinics of North America 30, no. 3 (August 2012): 795–804. https://doi.org/10.1016/j.emc.2012.06.006.
- Merino, José G., Marie Luby, Richard T. Benson, Lisa A. Davis, Amie W. Hsia, Lawrence L. Latour, John K. Lynch, and Steven Warach. “Predictors of Acute Stroke Mimics in 8187 Patients Referred to a Stroke Service.” Journal of Stroke and Cerebrovascular Diseases 22, no. 8 (November 2013): e397–403. https://doi.org/10.1016/j.jstrokecerebrovasdis.2013.04.018.
- Mozaffarian et Al. – Heart Disease and Stroke Statistics—2015 Update. https://www.ahajournals.org/doi/pdf/10.1161/CIR.0000000000000152.
- Nadarajan, V, R J Perry, J Johnson, and D J Werring. “Transient Ischaemic Attacks: Mimics and Chameleons.” Practical Neurology 14, no. 1 (February 2014): 23–31. https://doi.org/10.1136/practneurol-2013-000782.
- Nguyen, Peggy L., and Jason J. Chang. “Stroke Mimics and Acute Stroke Evaluation: Clinical Differentiation and Complications after Intravenous Tissue Plasminogen Activator.” The Journal of Emergency Medicine 49, no. 2 (August 2015): 244–52. https://doi.org/10.1016/j.jemermed.2014.12.072.
- Nor, Azlisham Mohd, and Gary A. Ford. “Misdiagnosis of Stroke.” Expert Review of Neurotherapeutics 7, no. 8 (August 2007): 989–1001. https://doi.org/10.1586/14737175.7.8.989.
- Sivakumaran, Prasanthi, Dipender Gill, Gheed Mahir, Aravindhan Baheerathan, and Arindam Kar. “A Retrospective Cohort Study on the Use of Intravenous Thrombolysis in Stroke Mimics.” Journal of Stroke and Cerebrovascular Diseases 25, no. 5 (May 2016): 1057–61. https://doi.org/10.1016/j.jstrokecerebrovasdis.2016.01.012.
- Tintinalli’s Emergency Medicine: A Comprehensive Study Guide. 7th
- Tobin, W. Oliver, Joseph G. Hentz, Bentley J. Bobrow, and Bart M. Demaerschalk. “Identification of Stroke Mimics in the Emergency Department Setting.” Journal of Brain Disease 1 (March 31, 2009): 19–22.
- Tsivgoulis, Georgios, Ramin Zand, Aristeidis H Katsanos, Nitin Goyal, Ken Uchino, Jason Chang, Efthimios Dardiotis, et al. “Safety of Intravenous Thrombolysis in Stroke Mimics,” n.d., 7.
- Vilela, Pedro. “Acute Stroke Differential Diagnosis: Stroke Mimics.” European Journal of Radiology 96 (November 2017): 133–44. https://doi.org/10.1016/j.ejrad.2017.05.008.
- Vroomen, Patrick C.A.J., Marieke K. Buddingh, Gert Jan Luijckx, and Jacques De Keyser. “The Incidence of Stroke Mimics Among Stroke Department Admissions in Relation to Age Group.” Journal of Stroke and Cerebrovascular Diseases 17, no. 6 (November 2008): 418–22. https://doi.org/10.1016/j.jstrokecerebrovasdis.2008.06.007.
- Zinkstok, Sanne M., Stefan T. Engelter, Henrik Gensicke, Philippe A. Lyrer, Peter A. Ringleb, Ville Artto, Jukka Putaala, et al. “Safety of Thrombolysis in Stroke Mimics: Results From a Multicenter Cohort Study.” Stroke 44, no. 4 (April 2013): 1080–84. https://doi.org/10.1161/STROKEAHA.111.000126.


Thank you for taking the extra time and effort to present this topic in this format. Excellent summary of stroke mimics.
I would just like to point out a small pitfall when reading quickly through a large amount of reading material………
The homunculus is a great visual memory aid for remembering motor and sensory representation in the lateral cortex, but it is a good idea to emphasize ( particularly when looking at the eye in the homunculus diagram ) that it does not represent function ( i.e. visual field, which is occipital cortex )
This point was made clear to me in that “old school fashion” many years ago. I still cringe when thinking about it…… Someday, if you buy me a coffee.
But if tPA does not work patients should not be exposed to any potential harm, even if the harm is small (1-2%)
http://thesgem.com/2019/02/sgem-xtra-no-retreat-no-surrender-thrombolysis-for-acute-ischemic-stroke/