

In the second part of this two-part series, Dr. Michael Wong discusses the process for obtaining consent for incapable persons in the Emergency Department. For a review of a rational and patient-centered approach to difficult discussions in the Emergency Department around goals of care and resuscitation, please see the first installment of this series.
Ontario’s Health Care Consent Act allows for treatment of an incapable person in an emergency “if the delay required to obtain consent/refusal on the person’s behalf will prolong the suffering that the person is apparently experiencing or will put the person at risk of sustaining serious bodily harm.” 1
However, we should also consider if resuscitation is inappropriate and the legal/professional expectations in these cases.
Case 1: The Case of the Missing SDM
|
90 y.o. woman dx with severe dementia & aspiration event
|
Section 26 of the Health Care Consent Act reads, “A health practitioner shall not administer a treatment under [emergency consent] if the health practitioner has reasonable grounds to believe that the person, while capable and after attaining 16 years of age, expressed a wish applicable to the circumstances to refuse consent to the treatment.” 1
To rephrase, one cannot treat someone if you have evidence of a clear previously expressed wish. One precedent in which this is clear is Malette vs. Schulman.2 In 1979, Mrs. Malette was a Jehovah’s Witness practitioner and carried a signed but undated wallet card describing her wish to never be transfused. Dr. Schulman chose to transfuse her in the context of severe trauma and likely saved her life by doing so. Nonetheless, Dr. Schulman was found guilty of battery and paid $20,000 for acting against her wishes.
In 100% of circumstances, the health care team should make every effort to reach a substitute decision maker (SDM). Barring a Consent and Capacity Board ruling that the SDM is no longer acting in the patient’s best interests, the SDM is always considered the health care team’s best knowledge of previous wishes. But in the absence of a SDM, consider other evidence of prior wishes – and the likely validity of DNR Confirmation Forms, wallet cards, etc.
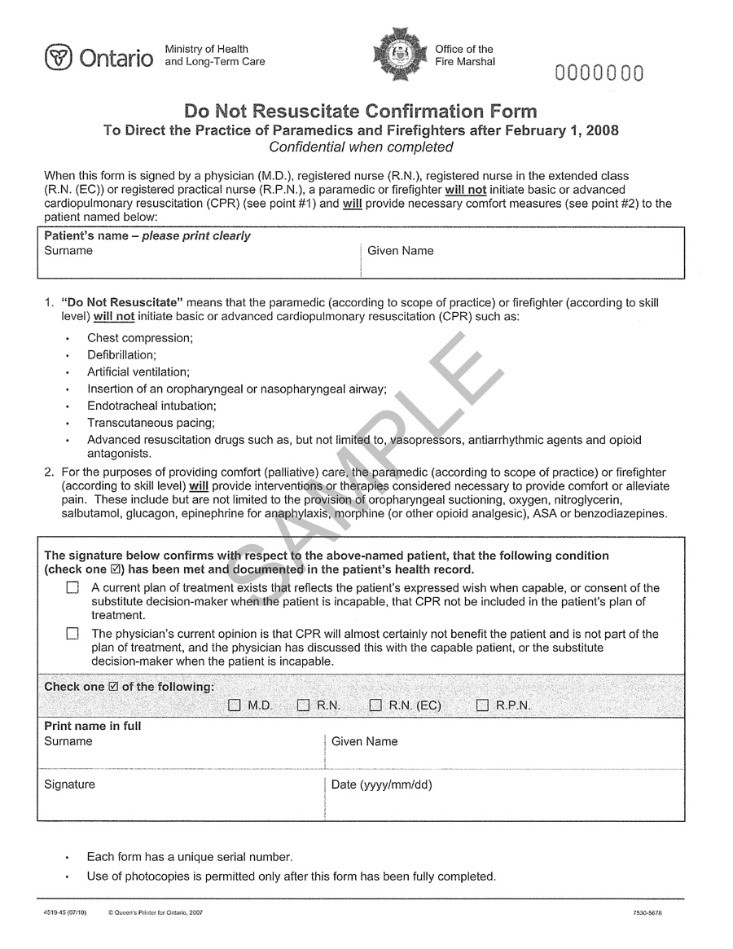
In this case, the Ontario DNR Confirmation form is very specific in barring paramedics from providing CPR, defibrillation, artificial ventilation, oro/nasopharyngeal airways, intubation, transcutaneous pacing, vasopressors, antiarrhythmics, and opioid antagonists, while confirming that a previous discussion took place between a physician and the patient or SDM to confirm this wish. Although the form is targeted towards paramedics, it represents a clearly delineated wish that hospital-based practitioners should respect if no SDM can be reached. The expectation, nonetheless, is that all efforts must be made to contact an SDM. In the absence of any previous wish or SDM, physicians may use their judgement in what care to provide.
Case 1 Resolution: The Case of the Missing SDM
|
I would choose to:
|
Case 2: Medical Futility
|
You are an emergency physician in a rural setting, and you encounter the following:
|
The most relevant information to this case is the College of Physicians and Surgeons of Ontario (CPSO) policy and the case of Douglas DeGuerre.
In brief, Douglas DeGuerre was an 88-year-old man admitted for complications of vasculopathy. He had a previous nursing home directive that indicated a no-CPR order. Several family meetings took place that went back and forth on CPR orders, but when he required bilateral above-knee amputations, his SDM noted that she believed he would want to be full code perioperatively. Full code status was initially confirmed post-operatively, but weeks later, a team of staff physicians and ethicists were consulted, and a no-CPR order was written based on medical futility. Attempts to contact the SDM were unsuccessful. Mr. DeGuerre decompensated and unfortunately, the SDM arrived at the hospital with him in respiratory distress. At the bedside, she requested that he be resuscitated, but the physicians declined, and he died.3
After multiple hearings, the CPSO and HPARB (a board that oversees the CPSO) ruled that it was unacceptable to write a no-CPR order / change an existing treatment plan without discussing with the SDM. The CPSO policy4 subsequently changed and read:
- “A CPR order cannot be made unilaterally […] discussion [with the SDM] must occur before a no-CPR order can be written. […]
- “If the patient or SDM […] insists that CPR be provided, physicians must engage in the conflict resolution process, […and] may not write a no-CPR order. If an event requiring CPR occurs [in the interim], physicians must provide CPR. […] Physicians must act in good faith and use their professional judgment to determine how long to continue providing CPR.”
This was, of course, controversial, and the CPSO policy has several limitations.
- No adult Critical Care or Emergency Physicians were consulted in the creation of the initial policy
- Downar et al. wrote an editorial in the CMAJ and noted that “CPR is a bridge to life support; if life support is determined to be inappropriate, CPR is not clinically indicated. […] What is the appropriate duration of inappropriate CPR? […] If a physician’s judgment cannot be trusted to determine when to withhold CPR, why would it be sufficient to determine when to stop CPR?”5
The CPSO policy4 was subsequently modified in 2016 to add:
- “If the patient or SDM insists that CPR be provided […] physicians must provide CPR unless the patient’s condition will prevent the intended physiologic goals of CPR (i.e., providing oxygenated blood flow to the heart and brain) from being achieved.”
If the intended physiologic goals of CPR are impossible, and “the patient arrests, physicians may make a decision about whether or not to provide CPR while attending to the patient.”6
Case 2 Resolution: Medical Futility
|
I would choose to:
|
Take Home Points
- It is the physician’s responsibility to integrate the medical prognosis with previously known wishes to offer and recommend only reasonable treatment options
- Previous wishes
- Physicians may not provide treatment in conflict with the best knowledge of previous wishes (Health Care Consent Act)
- Barring a consent and capacity board ruling to the contrary, the SDM is considered to have the best knowledge of a previously expressed wish. It is the SDM, not the physician, who has the responsibility of interpreting a living will.
- In the absence of a SDM, a physician may utilize other available information to establish a previously known wish
- CPR
- Physicians must communicate to the patient or SDM when not offering CPR, and cannot change an existing plan of care without consent
- If CPR has the potential to be physiologically successful, and a SDM disagrees with your recommendation to not offer CPR, the current CPSO policy states that it should be provided
- In the absence of any previous wish or SDM, physicians may use their judgement to determine what care to provide
Note
- The above examples are hypothetical but common cases; any similarity to real life is accidental
- The above responses are based on Ontario, Canada law and professional frameworks – requirements and expectations may vary by practice location outside of Ontario
- Professional policies and legal precedents are likely to develop and change with time
References
- Health Care Consent Act. Ontario, Canada; 1996. https://www.ontario.ca/laws/statute/96h02.
- Hebert P. Doing Right: A Practical Guide to Ethics for Medical Trainees and Physicians. OUP Canada; 2008. https://books.google.ca/books?id=Yc5fPQAACAAJ.
- CPSO. Inquiries, Complaints, and Reports Committee: Decision and Reasons Re: Douglas DeGuerre. 2015. http://thaddeuspope.com/images/DeGuerre_-College-of-Physicians-and-Surgeons-of-Ontario.pdf.
- CPSO. CPSO Policy Statement: Planning for and Providing Quality End-of-Life Care. CPSO Policy Statement #6-16. 2016;(3):1-12.
- Downar J, Warner M, Sibbald R. Mandate to obtain consent for withholding nonbeneficial cardiopulmonary resuscitation is misguided. CMAJ. 2016;188(4):245-246. doi:10.1503/cmaj.151205.
- College of Physicians and Surgeons of Ontario. Planning For and Providing Quality End-of-Life Care: Frequently Asked Questions. 2016.


Great read guys, thanks!