

In this two-part series, Dr. Michael Wong begins by reviewing a rational and patient-centered approach to difficult discussions in the Emergency Department around goals of care and resuscitation. In part two, we discuss the process for obtaining consent for incapable persons in the Emergency Department.
Common pitfalls with the current paradigm
Heyland et al.1 interviewed 1439 patients and family members across 16 Canadian hospitals and compared the patient/substitute decision maker (SDM)’s self-described resuscitation preferences to the documented code status in the chart. They found a 37% error rate – 35% of patients didn’t want CPR but had a full code order, and 2% wanted CPR and had a no-CPR order. This is an unacceptable level of avoidable medical error.
DNR forms were first described in 19762, in an era when whether or not patients received CPR would be up to the resident/staff on call, and decisions were often not shared with patients.3 These forms were an attempt to standardize these decisions to improve patient transparency, autonomy, and to help bedside personnel who would often be first on the scene. Unfortunately, the result was often a menu-like list of options without counseling towards appropriate options – an area in which we must do better.
This “resuscitation menu,” or asking “should we do everything if your heart stops?” is an ineffective way to have goals of care conversations. From the patient perspective, our medical expertise and knowledge mean that when we offer a treatment or a menu of options, they are reasonable and realistic options – when in reality, they may not be appropriate or in keeping with the patient’s values around the quality of life. Studies show that patients often have a poor understanding of CPR, intubation, and unrealistically optimistic expectations.4–7
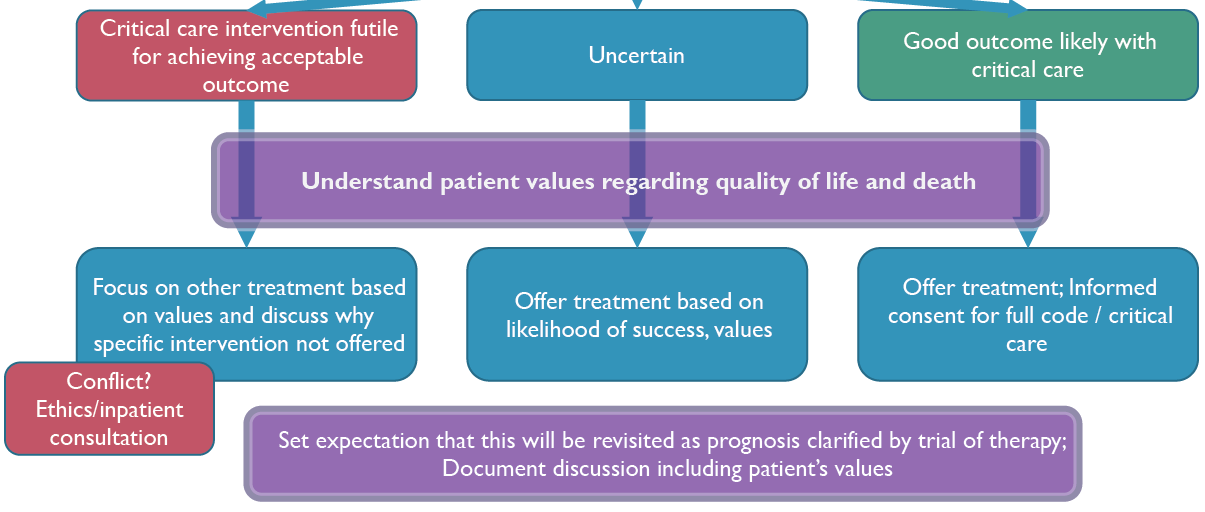
Instead, we should focus on understanding a patient’s values and wishes in life and death, and then use our expertise to counsel patients around risks/benefits/alternatives. Ultimately, we must only suggest treatments in keeping with their wishes.
To begin, we must establish patient capacity or identify the best substitute decision-maker. If the patient is not capable, Ontario and most Canadian provinces have a hierarchy of SDMs.8 Some jurisdictions have an age requirement to act as an SDM – in Ontario the minimum age is 16. Once we have the appropriate individual, we can begin.
Algorithm for doing goals of care discussions in the ED
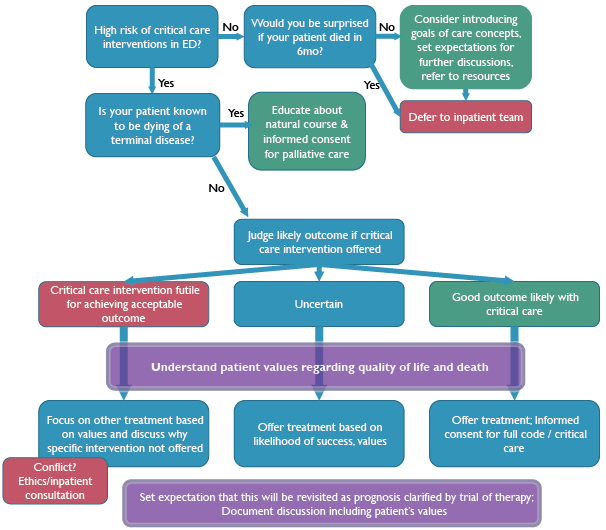
This is a general algorithm that can be applied in the context of CPR vs. no-CPR, intubation vs. no-intubation, or other critical care interventions. Let’s walk through the steps in more detail.
Step 1: Is a goals of care discussion time sensitive?

While it is standard of care for admitting teams to explore a patient’s goals of care on admission to hospital, the Emergency Department team must balance departmental flow. The Emergency Physician should target high-risk patients like:
- Anyone for whom critical care is being proposed
- Unstable patients with advanced cancer, comorbidities, or advanced physiological age/frailty
- Patients who have critical diagnoses at high risk for decompensation (STEMI, massive PE, etc.)
In those patients who are not at high risk, consider using the surprise question to screen for patients who may still benefit from a discussion or referral to resources.
Step 2: Is your patient known to be dying of a terminal disease? Do they already have palliative goals of care?
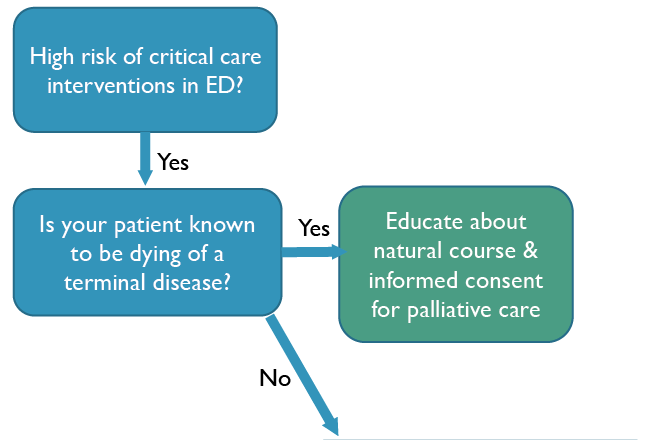
If so, we should focus our conversation on good dying, educating about the natural course of the disease, and emphasizing interventions we can do for symptom control. Disposition (hospice, home, or hospital) is key, and we should learn what local resources to call and help our patient in their journey.
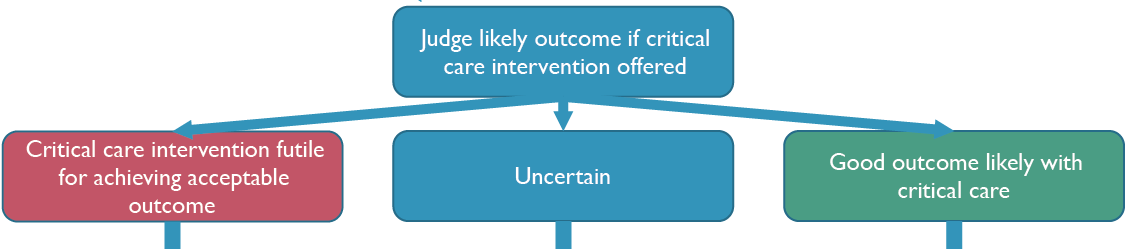
Step 3: Prognosticate – would your patient benefit from critical care? Intubation? CPR?
Consider the nature of the acute illness, the patient’s baseline function and comorbidities, and their overall trajectory of life and function.
Trajectories of Illness
Images below are from Lunney et al.9
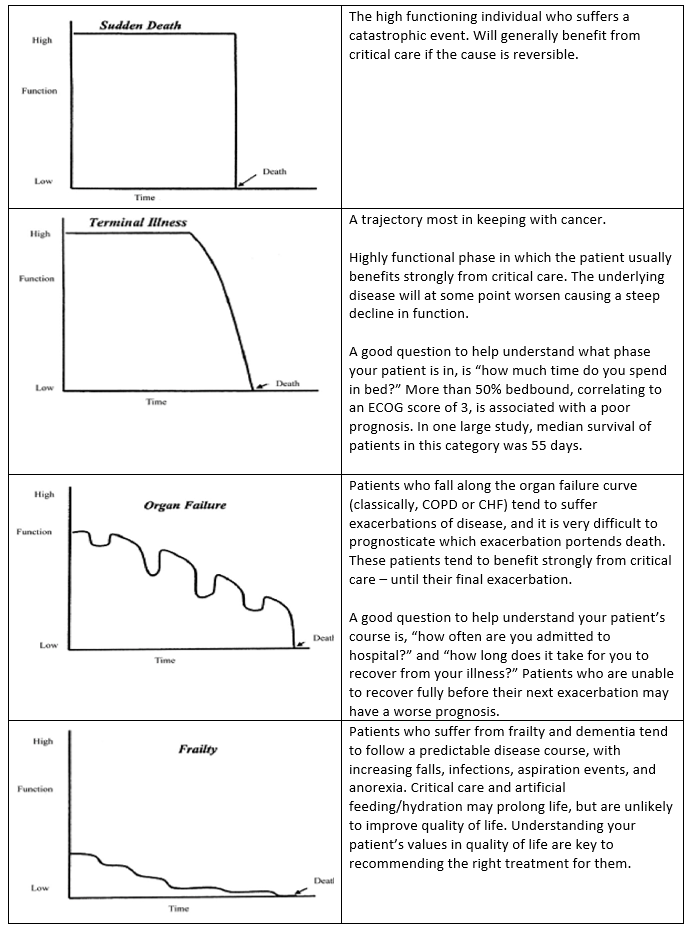
Specifically, for cardiac arrest, the following information may help understand the risks/benefit of CPR.
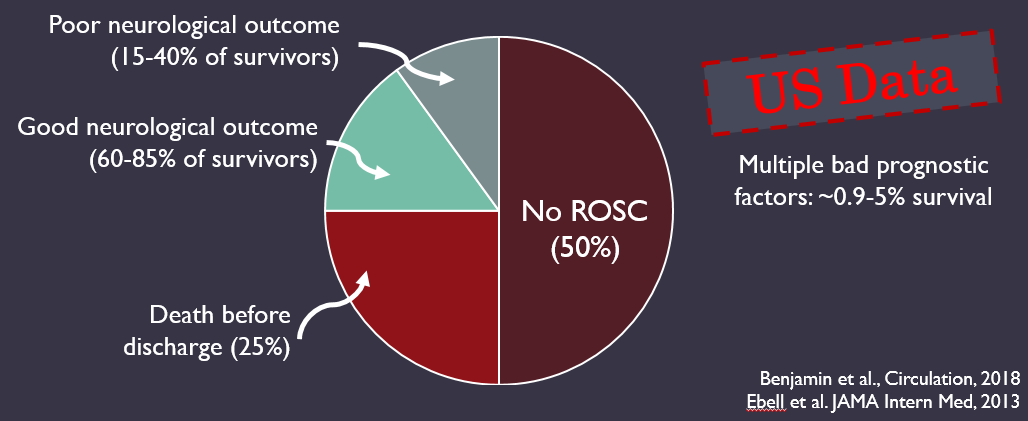
- General outcomes data
According to 2018 US data,10 amongst hospitals subscribed to a specific data collection and quality improvement system, survival to hospital discharge from cardiac arrest is ~25%, but 15-40% of these survivors will have a poor neurologic outcome. The risks of CPR include a poor neurologic outcome, chronic ventilation/dialysis, and prolonged hospital stay with a high mortality rate.
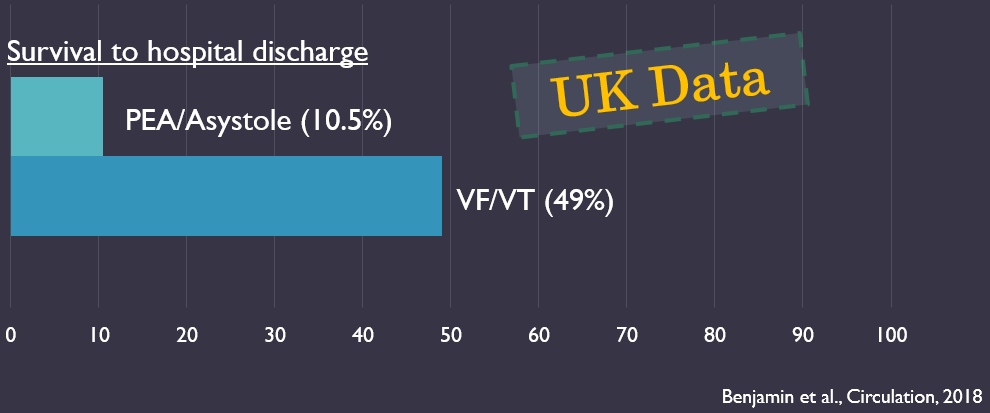
Patients who suffer VF/VT arrests have much better survival rates (49%) than PEA/asystolic arrests (10%),10 and thus, patients admitted for active cardiac disease are more likely to benefit from full code status.
- GO-FAR score11
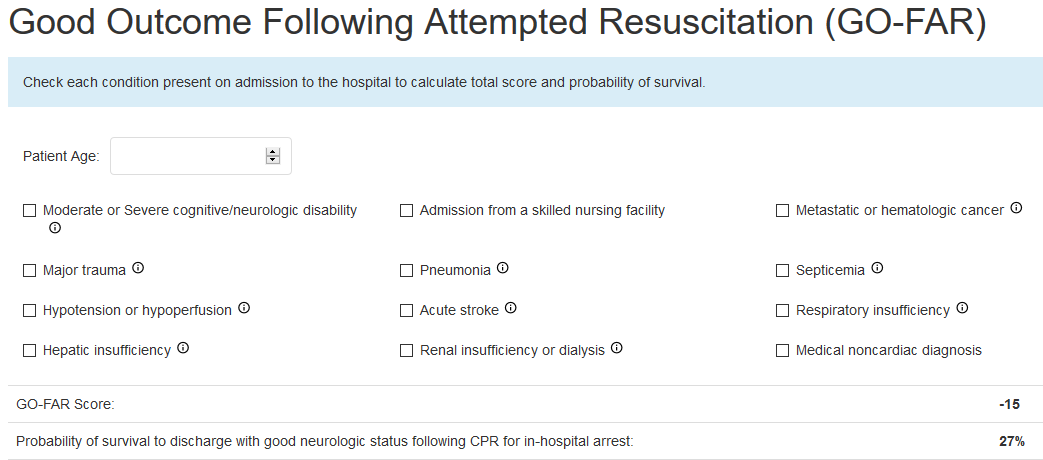
(From Jonathan Rubins website: https://www.gofarcalc.com/)
The GO-FAR score is the best clinical decision rule for prognostication for in-hospital cardiac arrest. Each of the variables confers additional poor prognosis in a cumulative fashion. Of note, active cardiac disease is not one of the factors – again emphasizing that patients admitted for cardiac disease are more likely to survive in-hospital cardiac arrest.
The GO-FAR score may help to trigger or frame your discussion, but communicating numbers and statistics are unlikely to be helpful in an emotional situation.
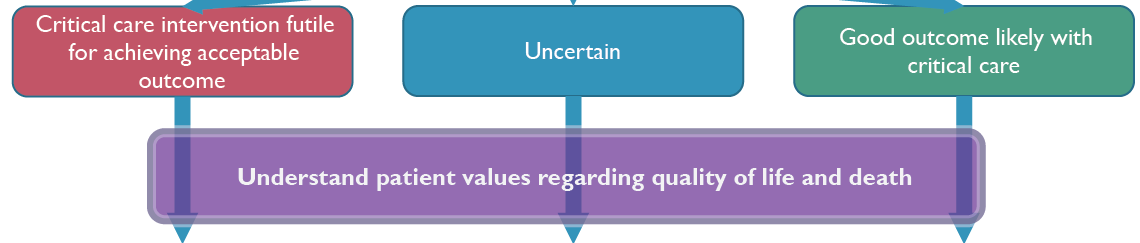
Step 4: “Concern, Context, Counsel”
Speak to your patient and their family to understand values and wishes around quality of life. Adapted from Gray.12
Some key phrases may be helpful in talking to patients or substitute decision makers: 13
- I am really worried about <the patient>, he/she is really sick
- Would you be able to tell me about how things are going at home – what is <the patient’s> day like on a good day?
- If <the patient> could have this conversation with us, what would <the patient> say about this situation?
- I can’t imagine how difficult it must be to try to speak for <the patient>
- Thank you for being here for <the patient>
- Would it be ok for me to share my recommendation as to how to best care for <the patient>?
Step 5: Counsel – share your recommendation with the patient / SDM
Combine your medical expertise and thoughts around the risks/benefits of CPR, intubation, or other critical care interventions you are proposing to form a recommended course of treatment.
Treatment can be a simultaneous combination of disease-modifying and palliative-like symptomatic care.14 For instance, low doses of morphine for dyspnea can be effective in pulmonary hypertension, COPD, and CHF exacerbations.
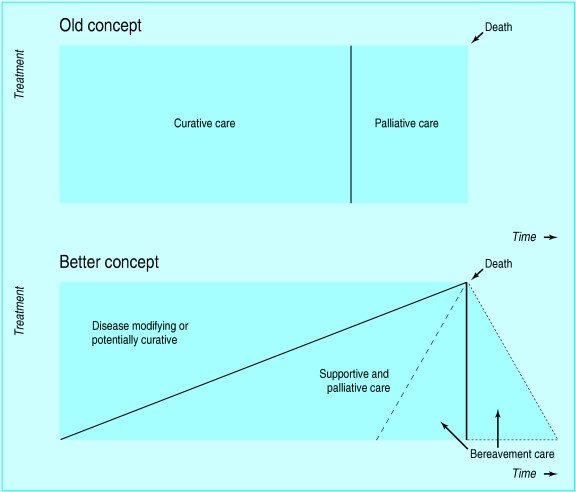
From Murray et al., BMJ, 200514
Step 6: Document and set expectations
Document your discussion, and what the patient/SDM said about their wishes and values in quality of life. Set the expectation that this is dynamic and may change as the inpatient teams understand more about the patient’s illness — handover well to the inpatient team.
Barriers to goals of care discussions, as perceived by physicians and nurses, were described by You et al.15 Clinicians biasedly rated the health literacy or patient / SDM barriers as the most significant barriers – however, it is the health care team barriers we can work on every day on shift
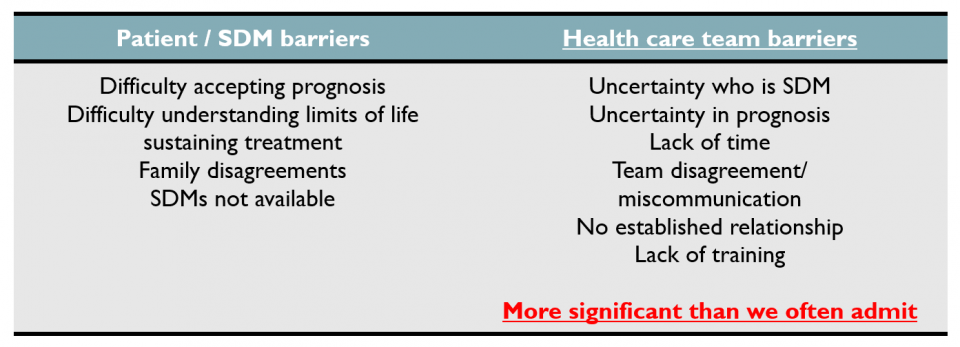
Let’s normalize goals of care conversations and prioritize learning the medical expertise and communication skills required to effectively engage and advocate for our patients.
Take Home Points
- Goals of care conversations should be initiated by the Emergency Physician for patients at high risk of requiring critical care
- Form a medical judgment of the likely outcome with critical care interventions using patient comorbidities, the nature of the acute illness (e.g., cardiac disease vs. non-cardiac disease), and the patient’s trajectory of life
- Frame discussions around understanding patient values and goals; integrate this with your medical judgement of likely outcome with critical care to form a treatment recommendation
- Physicians should only offer reasonable treatments; the “resuscitation menu” is inappropriate and ineffective
- Palliative-like symptom control and disease-modifying therapy can be simultaneous
- Help each other overcome health care team barriers to good goals of care conversations
References
- Heyland DK, Ilan R, Jiang X, You JJ, Dodek P. The prevalence of medical error related to end-of-life communication in Canadian hospitals: Results of a multicentre observational study. BMJ Qual Saf. 2016;25(9):671-679. doi:10.1136/bmjqs-2015-004567.
- Rabkin MT, Gillerman G, Rice NR. Orders Not to Resuscitate. N Engl J Med. 1976;295(7):364-366. doi:10.1056/NEJM197608122950705.
- Rabkin M. Orders Not to Resuscitate: The Origin of the DNR Order. Open Pediatrics. https://www.openpediatrics.org/assets/video/orders-not-resuscitate-origin-dnr-order. Published 2017.
- Diem SJ, Lantos JD, Tulsky JA. Cardiopulmonary Resuscitation on Television — Miracles and Misinformation. N Engl J Med. 1996;334(24):1578-1582. doi:10.1056/NEJM199606133342406.
- Shif Y, Doshi P, Almoosa KF. What CPR means to surrogate decision makers of ICU patients. Resuscitation. 2015;90:73-78. doi:10.1016/j.resuscitation.2015.02.014.
- Portanova J, Irvine K, Yi JY, Enguidanos S. It isn’t like this on TV: Revisiting CPR survival rates depicted on popular TV shows. Resuscitation. 2015;96:148-150. doi:10.1016/j.resuscitation.2015.08.002.
- Gehlbach TG, Shinkunas LA, Forman-Hoffman VL, Thomas KW, Schmidt GA, Kaldjian LC. Code status orders and goals of care in the medical ICU. Chest. 2011;139(4):802-809. doi:10.1378/chest.10-1798.
- College of Physicians and Surgeons of Ontario. Consent to Treatment.; 2015. doi:10.1080/09585189108408619.
- Lunney JR, Lynn J, Hogan C. Profiles of older medicare decedents. J Am Geriatr Soc. 2002;50(6):1108-1112.
- Benjamin EJ, Virani SS, Callaway CW, et al. Heart Disease and Stroke Statistics – 2018 Update: A Report from the American Heart Association. Vol 137.; 2018. doi:10.1161/CIR.0000000000000558.
- Ebell MH, Jang W, Shen Y, Geocadin RG. Development and validation of the Good Outcome Following Attempted Resuscitation (GO-FAR) score to predict neurologically intact survival after in-hospital cardiopulmonary resuscitation. JAMA Intern Med. 2013;173(20):1872-1878. doi:10.1001/jamainternmed.2013.10037.
- Gray N. How do you discuss code status? Cartoons of common traps. The Ink Vessel. https://inkvessel.com/2017/12/14/how-do-you-discuss-code-status-cartoons-of-common-traps/. Published 2017. Accessed March 28, 2019.
- Weingart S. Podcast 165 – The Semantics of End of Life Discussions with Ashley Shreves. 2016. https://emcrit.org/emcrit/semantics-end-of-life-discussions/.
- Murray SA, Kendall M, Boyd K, Sheikh A. Illness trajectories and palliative care. BMJ. 2005;330(7498):1007-1011. doi:10.1136/bmj.330.7498.1007.
- You JJ, Downar J, Fowler RA, et al. Barriers to goals of care discussions with seriously ill hospitalized patients and their families: A multicenter survey of clinicians. JAMA Intern Med. 2015;175(4):549-556. doi:10.1001/jamainternmed.2014.7732.


Trackbacks/Pingbacks