A Code Orange is a hospital-scale response to any event or group of events that results in a patient influx that outstrips available hospital resources. It realigns the way the hospital functions to support the emergency department and rapidly increases the number of staff available to care for patients. It also functions to create appropriate clinical space to treat patients. A Code Orange response will vary depending on the needs of the hospital in the context of the event at hand. A Code Orange at a small community hospital may be required for 3 critically ill trauma patients, while at a major tertiary care trauma center, it may be required at a threshold of 8-10 critically ill patients. These numbers will vary based on the severity and type of injuries as well as the time of day.
Importance of Code Orange
In planning for a disaster, many elements of critical societal infrastructure must be considered for the safety of a community. Hospitals and healthcare are one of these elements, and thus, a robust health-sector emergency management plan is vital to the well-being of the community. The ability to maintain continuity of operations at a major regional trauma center, for example, directly mitigates the harm from any potential injury-creating event.

Elements of Critical Infrastructure
If health care providers (HCPs) are unable to safely and effectively provide care, then the lack of these services affects not only our usual patient population but also those members of the community affected by the disaster. Recently, there have been many examples of Mass Causality Incidents (MCIs) with the potential to overwhelm hospital resources. These events are becoming more common and have included terrorist attacks (Christchurch, New Zealand shooting), hate crimes (Orlando, Florida Pulse Nightclub shooting), Motor Vehicle Collisions (Humboldt, Saskatchewan Bus Collision), Mass shootings (Las Vegas, Nevada Shooting), and Natural Disasters (Florida, Hurricane Michael).
Mass Casualty Simulation
In recent years simulation has become a core component of medical education. The ability to be exposed to realistic high acuity scenarios on a more frequent basis helps HCPs to improve performance whenever they encounter a similar scenario in their practice. In Situ Simulation (ISS) is a branch of simulation-based education where the simulated scenario is moved from a ‘simulation theatre’ to the actual clinical environment. By doing this, ISS has been successful in creating more realistic scenarios, enhancing knowledge retention, improving the overall clinical experience for learners, and helping to identify latent safety threats. (1-4)
Just as ISS at The Ottawa Hospital (TOH) has improved our care for the single patient, it was believed that expansion of ISS to an MCI level would allow for us to test our Code Orange response on a full scale. To do this, the largest simulation ever performed at TOH was arranged to test our Code Orange response. Using ISS, 20 simulated patients, being played by medical students and members of the Canadian Armed Forces in full moulage, were transported to the ED over 50 minutes from the scene of a hypothetical mass shooting. A Code Orange was struck at the TOH Civic campus; all patients were triaged, resuscitated, and transported to the OR (or appropriate clinical area) according to their injuries. This simulation allowed for a successful test of our Code Orange system and was a valuable learning experience for all HCPs who were involved while helping to identify latent safety threats (LSTs) in our current Code Orange plan. This simulation was received with great enthusiasm from clinical and administrative staff throughout the hospital and served as a valuable experience and an opportunity for many staff to familiarize themselves with the concepts and plans relating to a Code Orange.
Westboro Bus Collision and Code Orange
The Westboro bus collision occurred Jan 11th, 2019 at 1550. This tragic event resulted in the deaths of 3 people and significant injuries for 23 others. This disaster was a single isolated event in which a double-decker city transit bus collided with an overhang of a pedestrian shelter at 60-80 km/h at the Westboro bus station. As a result of this event, the Civic hospital received 14 patients to our trauma service, with 13 arriving within 74 minutes. Of these patients, two arrived at the hospital without vital signs and were unable to be resuscitated. No patients who arrived at the hospital alive died from their injuries. Six patients from this collision were resuscitated and transferred to the OR within 1 hour and 45 minutes from hospital arrival. TOH’s Code Orange response to this incident was an overall success. However, it is important to continue to improve and learn from experiences such as this disaster.

12 Things you need to know as an Emerg Doc
Below are 12 pearls that ED physicians should know about a Code Orange so that they can be prepared for their next shift. This list was compiled from ED physicians who were present for the Code Orange as well as TOH Trauma surgeons, members of the TOH Emergency Management group, and the formal After-Action Report.
1. How and when to call a Code Orange
-
- Call for help early. As soon as you consider calling a Code Orange, activate a Level 1 Trauma. This will begin to activate hospital resources and get the TTL on Call in the ED. It will also allow you to collect information from the Paramedic Communication Duty Officer.
- Open the code station in your area to find your job action sheet which will have the steps you need to take
- The official decision to call a Code Orange typically will not fall on the Resus ED physician. Follow your job action sheet and contact the Administrator on call or member of the Senior Management Team who will be the one to activate the Code. Activation only falls to the front-line ED physician if the Administrator On-Call does not respond to their page within 10 minutes.
- As for Code Orange Major vs. Code Orange Minor. Don’t worry about this at all. A Code Orange is a scaled response and the decision for a Major vs. Minor response will be made by administration throughout the response based on the scale of the disaster.
2. Wear your vest
-
- Donning an identifying vest is the first step on most job action sheets.
- The role of the vest is to help people identify who is in what role within the Incident Management System (IMS) framework.
- Easy identification of roles in a chaotic environment created by a Code Orange is essential to help ensure a coordinated and effective response, so make sure you put on your vest!
3. Strike teams
-
- Strike teams are groups of healthcare providers who are assembled into a team and assigned a resuscitation bay. At a minimum, they will consist of an RT, ED MD, and ED RN. However, when resources allow, these teams can and should be expanded to resemble a typical trauma team. Having individual strike teams has shown to be beneficial during previous simulations as well as during the Westboro disaster response.
- Some keys to the success of strike teams are:
- Stick together. Do no change strike teams or rooms unless told to by the Chief TTL
- Focus on your room. Do not let the urge to observe other resuscitations distract you
- Be flexible. You may lose members when a patient is transported elsewhere after resuscitation. Be flexible in your roles and request new members from the Chief TTL if necessary
- Surgical specialists (e.g., Orthopedics, Vascular) typically do not have a role on a strike team to help minimize turnover on the teams. These specialists will be drawn from a separate labour pool and can be assigned to any patients requiring intervention at any stage of resuscitation. This helps to maintain stable strike teams during the response.
4. Prepare your room
-
- In preparation for an incoming trauma patient, a “pre-brief” has become standard of care to align the team’s goals and assign roles to HCPs. This becomes even more critical in a disaster scenario when resources may be limited. It is important to know who is in your strike team and what their skills are.
- It is important to repeat this pre-brief before each patient. This will allow you to reset your room, take stock of who remains with your strike team, and what materials/equipment you require. You should strive to provide the same quality of care for your 5th patient as you did your 1st and preparing for the patient with a pre-brief should be part of that care.
5. Disaster triage and Black tagged patients
-
- During disasters in the prehospital environment, START Triage will be used when the number of patients outstrips the number of available providers. START triage will assign people into 4 categories:
- Black: Non-Salvageable
- Red: Immediate
- Yellow: Delayed
- Green: Walking Wounded
START Triage, however, is not used by the triage physician and RN in the ED during the disaster at TOH. Instead, a similar scale is used, which is a melding of CTAS and START triage. This is done because nurses are not typically trained in START triage and a combination system will help to mitigate their unfamiliarity with START triage categories.
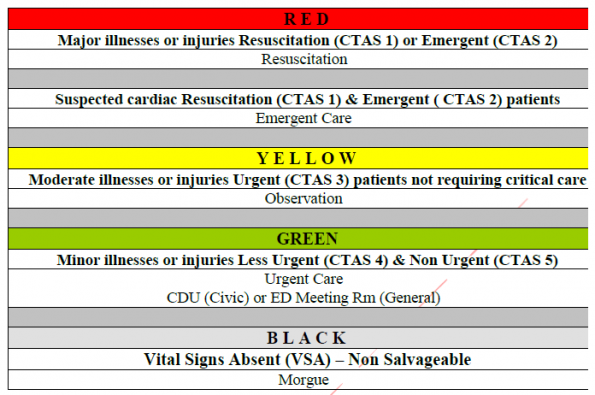
- It is important to understand that these Triage tools are only to be used when resources are strained by the number of patients requiring care. These tools are designed so that patients who require immediate care to survive are not affected by those who have limited or no chance at survival and those who will do not require immediate interventions to survive.
- This is a principle known as SAVE triage. SAVE stands for Secondary Assessment of Victim Endpoint and categorizes patients into 3 categories when care is being provided in a resource deplete environment:
- Patients who will die regardless of how much care they receive
- Patients who will survive whether they receive care or not
- Patients who will benefit significantly from austere field interventions
- It is the 3rd group of patients that you want to focus on because that is where the biggest difference can be made. But remember this only applies when you are in a resource-depleted environment. If the attempted resuscitation of a patient tagged Black is not affecting other patients, then continuing to attempt resuscitation is reasonable. This must be constantly reassessed by the Chief TTL and Triage physician; resuscitation can be halted at any point if it becomes detrimental to others.
- The overall goal that you must keep in mind is to do the greatest good for the greatest number of people
- During disasters in the prehospital environment, START Triage will be used when the number of patients outstrips the number of available providers. START triage will assign people into 4 categories:

6. Identification
-
- Patient identification proved to be one of the most difficult tasks during the Westboro MCI. Patient identification and family reunification are known to be a ubiquitous challenge in MCIs and can be so difficult that even family members can incorrectly identify patients (e.g. due to disfiguring injuries, etc.). We at TOH are no different, and during the Westboro bus collision, identification was a major challenge.
- To help limit the effect that identification has on patient care, it is important that all physicians and support staff have identification at the forefront of their minds in our response. Take the time to be familiar with the TOH disaster packs and their contents, which will have everything required to identify patients and link them to test results.
7. Know your role
-
- Recognize that unless you are in the role of Chief TTL, you may be limited in your ability to see and understand every aspect of the response. Because of this, you may lack a situational awareness of the hospital-wide response. Since your patient will only be one of many, you will need to be more flexible with your typical management as a more military/top-down approach is required to run a Code Orange successfully.
- You may end up having to manage patients differently or longer than you typically would. Requests for tests or supplies may be trumped by either the Chief TTL or other lead figures if they deem them to be more critical elsewhere. As always, it is important to work safely and to the best of your ability but realize that the focus of the Code Orange may place precedence on a patient other than yours, which is something that many of us will not be used to occurring.
8. Runners
-
- Consider assigning a runner as an individual role in your strike team.
- This person’s job will not consist of any patient contact, and thus, they will be free to run all errands necessary for your strike team (e.g., communicate, grab supplies, medications, equipment, etc.).
- This role is a mitigation strategy that can be used to bolster our response against the communication challenges that we know will occur during a Code Orange.
9. Disaster carts
-
- During an MCI and Code Orange, you will be seeing more critically ill patients than normal. With this, you will begin to deplete the supplies typically stored in the trauma bay.
- During a Code Orange, two disaster carts will be brought to the ED. This is where you can resupply all critical materials. These carts are stocked and continuously resupplied to ensure the department has the equipment it needs even if the disaster is ongoing over several days.
10. Documentation
-
- Similar to the role of runners, consider assigning a role within your strike team specifically for documentation.
- Each strike team will likely see multiple critically ill patients in rapid succession, and time will be a major constraint.
- MCIs are likely to result in a court case and documentation will be incredibly important.
- Having a team member whose sole focus is on documenting in the ED ROT will help to offload that task, as well as, help inform future HCPs of what care has been provided to the patient.
11. Effects on Colleagues
-
- It is important to understand that a Code Orange is a hospital scale response. Although a Code Orange initially focuses on the response in the ED, this phase of care can be over within a few hours, as was seen with the Westboro bus collision. Once the response is complete in the ED, the effects can still be felt in the hospital for days to come.
- Surgical services receive an influx of patients that will require prolonged admissions and multiple surgeries, which will force these teams to work above their capacity long after the event.
- Medical services will be affected by the sudden influx in patients to the floor during the ED decanting process. This will result in a substantial increase in workload for these teams as they are managing patients who they have yet to see or review with their junior residents before arriving on the floor.
12. Wellness
-
- As ED physicians, we are good at compartmentalizing these experiences, but an MCI and Code Orange may feel different. You may feel exhausted from the experience at some point, maybe not immediately, but over the next few days. Many people will find working the rest of the shift to be tough, and it’s important that you take some time for yourself to reset before seeing your next patient and ensure that you can provide safe and effective care.
- It may also be that your typical coping mechanisms to process these experiences will not be enough. Media coverage and public awareness of the event can make it more difficult to distance yourself, and you may end up having repeated exposure where typically you wouldn’t. This can potentially lead to a secondary injury from Critical Incident Stress.
- It’s important to recognize that these events can result in occupational injury and are part of the reason that all HCPs are more likely to develop PTSD and why we have higher suicide rates than the lay public. For these reasons, we need to ensure that we are mindful of ourselves during and after a Code Orange.
- For more information on PTSD in Emergency Physicians, please see Dr. Valerie Charbonneau’s previous Grand Rounds summary post.
- Take these opportunities to get together with your colleagues for a critical incident stress debrief that will be supported by Social Work, who have training specific to this. Organize the debrief either in the immediate period after the event or after your shift. Don’t be afraid to reach out to your colleagues if you weren’t working, to check in on how they are doing, and make yourself available if needed. Realize that you might not be functioning at your best in the days after the event and don’t be afraid to reach out for a shift change if you feel as though you are unsafe or unwell. For those who were not working, consider asking if someone who was working needs a day off in the aftermath of the event.
- Finally, we know that resources are available to us to help cope with these incidents. Our support teams, from Social Work to Occupational health to Psychiatry, will all be made available if you require help. If you want access to these resources, you can ask your immediate supervisor at any time.
References
- Petrosoniak A, Auerbach M, Wong AH, Hicks CM. In situ simulation in emergency medicine: Moving beyond the simulation lab. Emerg Med Australas. 2017 Feb;29(1):83-88. doi: 10.1111/1742-6723.12705
- Edwards S, Siassakos D.. Training teams and leaders to reduce resuscitation errors and improve patient outcome. Resuscitation. 2012 Jan;83(1):13-5. doi: 10.1016/j.resuscitation.2011.10.015.
- Steinemann S, Berg B, Skinner A, DiTulio A, Anzelon K, Terada K, et al. In situ, multidisciplinary, simulation-based teamwork training improves early trauma care. J Surg Educ. 2011;68:472–7. doi: 10.1016/j.jsurg.2011.05.009.
- Knobel A, Overheu D., Gruessing, M., Juergensen, I., & Struewer, J. Regular, in-situ, team-based training in trauma resuscitation with video debriefing enhances confidence and clinical efficiency. BMC Med Educ. 2018;18(1):127. doi: 10.1186/s12909-018-1243-x.