Welcome to Part 2 of our series on concussions. In this post, Dr. Erica Lee reviews how to make the diagnosis of concussion and manage these patients in the ED. You can review Part 1 of the series for an up-to-date definition of a concussion and Part 3 for a discussion around the complications and public health concerns of concussions.
Diagnosing a Concussion
Concussions remain a CLINICAL diagnosis, and there are currently no widely used, evidence-based, specialized tests for concussions.1–3 The diagnosis of concussion relies heavily on the history, physical exam, and ruling out more serious brain injuries. That being said, there are some important findings to look for on history and exam that can help make the diagnosis.
History
Your patient history is going to be the most useful aspect of your assessment, seeking information from the patient and witnesses to look for factors that point to a concussion and away from a more serious head or neck injury. In particular, you will need to establish:
- What trauma occurred that resulted in forces to the head
- What was the mechanism of injury?
- Did you feel a hit on your head, neck, or shoulders?
- Evidence of a “brief neurological impairment.”
- Determine what the patient remembers versus what they have been told
- Amnesia can be brief and smart patients will fill in the blanks
- Confusion and disorientation are the most difficult to determine, so put more weight on objective findings from witnesses3
- Was the patient slow to respond to questions? Did they appear stunned or have to stop play? Did they need more time than usual to get up?
- Presence of typical concussion symptoms
- Did they previously or currently have any symptoms in the four major categories?
- Determine what the patient remembers versus what they have been told
Physical Exam
All head injury patients should get a full neurological exam, including cranial nerves, power, reflexes, and cerebellar testing. Also, they should all have their neck examined, including palpation and range of motion. The following tests could help elicit symptoms of a concussion and are already part of or can easily fit into your neurological exam. Of note, the presence or absence of a single positive test does not necessarily point to or away from the diagnosis of a concussion; it is the clinical picture and your judgement that will help make the diagnosis.
- Orthostatic symptoms4
- Autonomic dysregulation may create orthostatic changes or symptoms
- Measuring dynamic visual acuity (VA)4,5
- Measure their VA with no head movement and then turning their head at 2 hertz
- Reduction in VA or development/worsening of symptoms is considered abnormal
- Accommodation4
- Measure the point at which they can no longer converge (start getting diplopia)
- Considered abnormal if it’s greater than 6 cm from the tip of their nose
- Extraocular movements5
- Saccades
- Ask patient to move eyes quickly between two stationary targets
- If it produces or worsens symptoms, considered abnormal
- Smooth pursuits
- Ask patient to focus and follow finger slowly from side to side
- If it produces or worsens symptoms, considered abnormal
- Saccades
Making the Diagnosis – Degree of Certainty
Concussion is a challenging diagnosis to make, and like most things in medicine, it exists on a spectrum of grey. One way to help make this process easier is to think about the diagnosis in terms of certainty – definitely, probably, or possibly a concussion, which is based on work by Dr. Christopher Giza’s group at UCLA. It breaks down the diagnosis based on historical features like mechanism or symptoms and attempts to make some black and white distinctions. Your degree of certainty will vary with your training, exposure, and general gestalt, but my interpretation is as follows:
- Definite concussion:
- History consistent (mechanism, LOC, amnesia), symptomatic
- Good mechanism, history unclear (if neurological impairment), symptomatic
- People who need a CT head and have a normal scan
- Probable
- Good mechanism, history consistent, no symptoms currently
- Mechanism unclear, history unclear, but very symptomatic
- Possible
- Mechanism good, history unclear, asymptomatic currently
Concussion Management
Once a concussion is diagnosed, several key management points are important for emergency physicians to know.2,6 Most of these points have evidence that they reduce long term symptomology. A recent prospective ED study demonstrated that only 42% of patients discharged home with a concussion received any education or information about their diagnosis.7 We can easily improve our discharge instructions by focusing on these key discharge discussion points:
- Giving patient education: what a concussion is, signs and symptoms, and setting expectations for recovery
- Management: What is subthreshold activity and the concept of hurt versus harm
- Recommendations for return to school/work, sport, and physical activity
- Supplying and providing information and resources
- The importance of not sustaining another concussion
Patient Education
While preparing for this post, we interviewed a physiatrist who said: “No one starts their concussion depressed or anxious, it develops over time because they are not meeting their expectations.” Patients are placed or place themselves under pressure because they feel their symptom tolerance dictates their progress. It can be frustrating, disheartening, and discouraging when their recovery is not what they expected. It is important to tell patients about their diagnosis and set expectations for their recovery, so they can anticipate what will be normal.
Several randomized controlled trials demonstrate that simple, educational interventions work at reducing persistent symptoms. One study used an educational booklet outlining symptoms, timelines, and coping strategies to successfully reduce symptoms over 3 months.8 Another group randomized patients to receive telephone calls with standardized scripts that also decreased symptoms and improved functional and financial outcomes (more patients had returned to work).9 Finally, a pilot study sent daily text messages for 2 weeks with “self-care support” messages that decreased the number and severity of symptoms, but did not reach statistical significance.10 There are several, easily available online handouts linked below that can be printed in the ED and provided to patients and significantly reduce their symptom burden.
Subthreshold Activities
The cornerstone to concussion management is 24-48 hours of rest followed by the initiation of graded subthreshold physical and cognitive activity regardless if symptoms are still present.1,2,11–13 Subthreshold activity or the “safe zone” is capped at the activity level where new symptoms present or old symptoms intensify. For athletes, this threshold can be measured using the Buffalo Concussion Treadmill Test, but for the average patient, it can be thought of as a rating scale from 0-10.14 If the patient rates their symptom score a 6 or less, then it’s safe to start the activity. Their threshold occurs when their symptom score climbs 2 points or reaches 7 – whichever comes first.
 Original figure from author
Original figure from author
It is important that patients understand that they need to push themselves to the point where it’s uncomfortable, but not past it. You don’t want them to be completely exhausted the next day. If patients push themselves too much or too quickly, they can “crash” leading to prolonged recovery. If patients stay within the safe zone consistently, the zone will get bigger over time because their symptom threshold also increases.
Hurt Versus Harm
It can be scary for patients to do activities that exacerbate their symptoms and this fear can prevent them from doing any activity at all. It is important to tell patients that things are going to hurt and it’s okay to hurt. A good comparison is a sprained ankle. You expect it to hurt every day, but you also test it every day to measure your progress. You may have a bad day, where it hurts more, and you can’t do as much; but the overall trajectory is upwards – getting better. You want to work a concussion like you would any other injury. By doing nothing and avoiding all the “hurt,” it will lead to harm and prolonged recovery.
Return to Activity – Physical Rest
Concussion management has always involved an aspect of rest but how long has varied over time. The first International Conference on Concussion in Sport recommended athletes be completely asymptomatic before they start rehab, and this dogma turned into days or weeks of rest for some patients.15 However, the duration and benefits of restrictive rest have been more thoroughly evaluated and questioned by several studies.16
- Thomas et al. (2015): The prescription of strict bed rest was found to create higher symptom burdens than usual care for pediatric patients 17
- Grool et al. (2016): Data from a large prospective pediatric cohort study demonstrated that early exercise decreased the risk of persistent symptoms at 28 days by ~11%18
- Leddy et al. (2019): An RCT evaluating early subthreshold aerobic exercise 2 days post-injury found that those who exercised sooner recovered quicker19
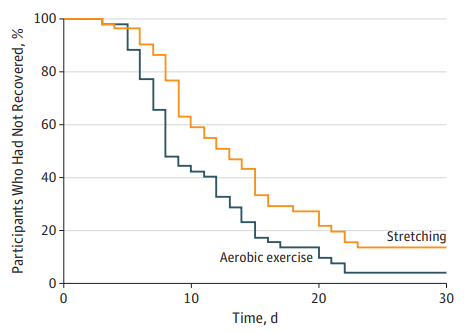 Taken from Leddy et all19
Taken from Leddy et all19
Based on these studies, recommendations for return to activity include a maximum of 2 days of physical rest and a graded return to activities with light aerobics as tolerated. In this case, physical rest means avoidance of highly aerobic activities that increase heart rate, but patients should still do some light activity like walking.
Examples of return to sport/activity schedules are available online here, here and here.
Return to Work/School – Cognitive Rest
Something that can often get overlooked in concussion management is cognitive rest, which is also a central component of concussion care.20 Cognitive stimulation can occur with bright lights, noisy or busy environments, or reading small text on screens. Studies have demonstrated that patients with higher cognitive loads without proper cognitive rest had prolonged symptoms.21
For pediatric patients and young adults, cognitive symptoms can impact their ability to go to school; for adults, it affects their ability to return to work. This can be difficult for some patients who feel they are unable to miss work. Studies show patients will not be able to function at full capacity, especially within the first few days, and we should counsel them about this.12
In summary, cognitive rest should be treated just like physical rest – a maximum of TWO days full rest and then graded return to activities as tolerated.
Examples of return to school schedules are available online here, here, and here.
Concerning return to work, a picture of a template work note is provided:
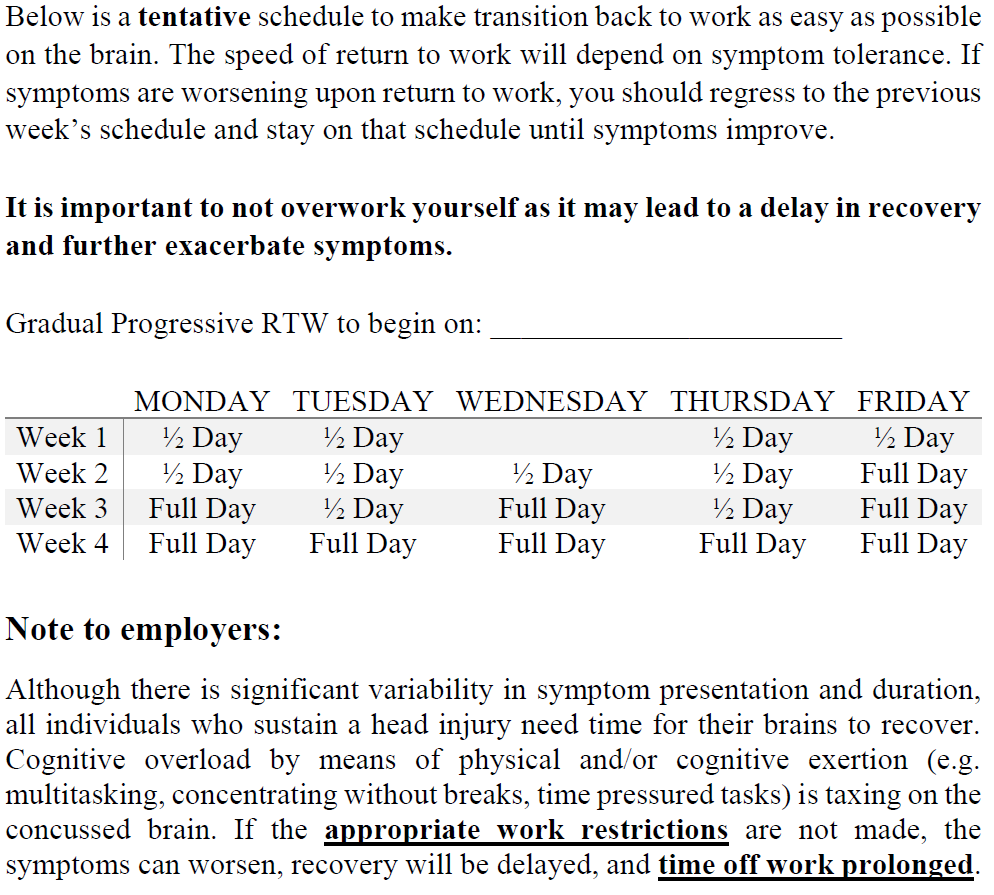 Original figure from author
Original figure from author
Where to Find Resources
There is a lot of misinformation about concussions on the internet and it can be overwhelming for patients and their loved ones. We can help by providing them with accurate information and easily accessible resources. Below is a list of easily accessible websites with good patient information from reputable sources:
- Ontario Neurotrauma Foundation (ONF)
- Ontario Brain Injury Association (OBIA)
- Concussion Awareness Training Tool (CATT)
- Parachute
- Concussions Ontario
- Videos:
 Image taken from http://ottawahospital.libguides.com/concussion_patient/.Courtesy of Dr. Shawn Marshall and The Ottawa Hospital
Image taken from http://ottawahospital.libguides.com/concussion_patient/.Courtesy of Dr. Shawn Marshall and The Ottawa Hospital
Avoid Brain Re-injury
It is extremely important to avoid re-injuring a concussed brain because it increases the risk for complications, including persistent symptoms and Second Impact Syndrome (SIS). The greatest risk for complications occurs in the first 10 days post-injury.22 Patients should avoid all of these high-risk activities for at least a week:2
- No driving for at least 24-48 hours, preferably until asymptomatic at rest
- No bike rides or contact sports
- No heavy lifting
- No working on ladders or at elevations with the risk of falls
Patients should also be advised to avoid alcohol and drugs (including caffeine) because they both slow down recovery and put them at risk for re-injury.2 Caffeine impacts your ability to sleep and stimulating an injured brain to work harder can create prolonged symptoms.2
Take Home Points
- Concussion remains a CLINICAL diagnosis
- Elicit key historical features that allow you to determine:
- What trauma occurred that resulted in forces to the head
- The occurrence of a “brief neurological impairment”
- Presence of typical concussion symptoms
- All head injury patients should get a full neurological and neck exam
- Consider adding the following to your physical exam of head injury patients:
- Orthostatic symptoms
- Dynamic visual acuity
- Accommodation
- Extraocular movements – saccades and smooth pursuit
- The key discharge discussion points are:
- Providing patient education: what is a concussion and setting expectations for recovery
- Describe subthreshold activity and the concept of hurt versus harm
- Give recommendations for return to school/work, sport, and physical activity
- Supply information and resources
- Reiterate the importance of not sustaining another concussion
References
- McCrory, P. et al. Consensus statement on concussion in sport—the 5 th international conference on concussion in sport held in Berlin, October 2016. Br. J. Sports Med. 51, bjsports-2017-097699 (2017).
- Marshall, S. Guideline for Concussion / Mild Traumatic Brain Injury & Persistent Symptoms.
- Ruff, R. M., Iverson, G. L., Barth, J. T., Bush, S. S. & Broshek, D. K. Recommendations for Diagnosing a Mild Traumatic Brain Injury: A National Academy of Neuropsychology Education Paper. Arch. Clin. Neuropsychol. 24, 3–10 (2009).
- Matuszak, J. M., McVige, J., McPherson, J., Willer, B. & Leddy, J. A Practical Concussion Physical Examination Toolbox: Evidence-Based Physical Examination for Concussion. Sports Health (2016). doi:10.1177/1941738116641394
- Mucha, A. et al. A Brief Vestibular/Ocular Motor Screening (VOMS) Assessment to Evaluate Concussions. Am. J. Sports Med. 42, 2479–2486 (2014).
- Parachute. Canadian Guideline on Concussion in Sport. (2018).
- Seabury, S. A. et al. Assessment of Follow-up Care After Emergency Department Presentation for Mild Traumatic Brain Injury and Concussion: Results From the TRACK-TBI Study. JAMA Netw. open 1, e180210 (2018).
- Ponsford, J. et al. Impact of early intervention on outcome following mild head injury in adults. J. Neurol. Neurosurg. Psychiatry (2002). doi:10.1136/jnnp.73.3.330
- Bell, K. R. et al. The effect of telephone counselling on reducing post-traumatic symptoms after mild traumatic brain injury: A randomised trial. J. Neurol. Neurosurg. Psychiatry (2008). doi:10.1136/jnnp.2007.141762
- Suffoletto, B. et al. Mobile phone text messaging to assess symptoms after mild traumatic brain injury and provide self-care support: A pilot study. J. Head Trauma Rehabil. (2013). doi:10.1097/HTR.0b013e3182847468
- Harmon, K. G. et al. American Medical Society for Sports Medicine position statement: concussion in sport. Br. J. Sports Med. 47, 15–26 (2013).
- Levin, H. S. & Diaz-Arrastia, R. R. Diagnosis, prognosis, and clinical management of mild traumatic brain injury. Lancet Neurol. 14, 506–517 (2015).
- Maas, A. I. R. et al. Traumatic brain injury: integrated approaches to improve prevention, clinical care, and research. Lancet Neurol. 16, 987–1048 (2017).
- Leddy, J. J. & Willer, B. Use of graded exercise testing in concussion and return-to-activity management. Curr. Sports Med. Rep. (2013). doi:10.1249/JSR.0000000000000008
- Aubry, M. et al. Summary and agreement statement of the 1st International Symposium on Concussion in Sport, Vienna 2001. Clin. J. Sport Med. 12, 6–11 (2002).
- Silverberg, N. D. & Iverson, G. L. Is Rest After Concussion “The Best Medicine?” J. Head Trauma Rehabil. 28, 250–259 (2013).
- Thomas, D. G., Apps, J. N., Hoffmann, R. G., McCrea, M. & Hammeke, T. Benefits of Strict Rest After Acute Concussion: A Randomized Controlled Trial. Pediatrics 135, 213–223 (2015).
- Grool, A. M. et al. Association Between Early Participation in Physical Activity Following Acute Concussion and Persistent Postconcussive Symptoms in Children and Adolescents. JAMA 316, 2504 (2016).
- Leddy, J. J. et al. Early Subthreshold Aerobic Exercise for Sport-Related Concussion. JAMA Pediatr. 173, 319 (2019).
- McLeod, T. C. V. & Gioia, G. A. Cognitive Rest: The Often Neglected Aspect of Concussion Management. Athl. Ther. Today 15, 1–3 (2010).
- Brown, N. J. et al. Effect of Cognitive Activity Level on Duration of Post-Concussion Symptoms. Pediatrics 133, e299–e304 (2014).
- Giza, C. C. & Hovda, D. A. The New Neurometabolic Cascade of Concussion. Neurosurgery 75, S24–S33 (2014).